
Abstract
Introduction:
Estimation of total body surface area (TBSA) burnt and burn depth are among the most central parts of acute burn assessment/treatment as they determine the level and type of care needed. Traditional methods for determining burn extent on admission often lead to inaccurate estimations, especially in paediatric or overweight patients.
Aim:
To compare %TBSA at admission with validated %TBSA at discharge in different patient populations to investigate if significant over- or underestimation occurs.
Method:
This retrospective observational study is based on a patient registry of all the patients (n = 863) treated at the Uppsala University Hospital’s Burn Centre between 2010 and 2018. The patients were divided into subgroups based on age, gender, body mass index (BMI) and validated burn extent. The %TBSA estimated at admission was compared to the validated %TBSA in all groups separately.
Results:
As has been published before, we also found that the %TBSA in paediatric patients was more often overestimated as were the smaller injuries, whereas larger injuries were often underestimated. BMI did not clearly affect the estimations and there was no clear difference between the genders in estimated %TBSA.
Conclusion:
Inaccurate estimations of %TBSA are common, particularly for paediatric patients and small or large injuries. We recommend a careful accurate approach when calculating %TBSA in the paediatric population to avoid over- and under-resuscitation. Increased education and training are recommended to improve accurate estimation in the future.
Lay Summary
The correct estimation of both extent and depth of burn is very important. This assessment guides the lever of care needed, the necessary amount of fluid resuscitation, the predicted outcome and more. It has been proven notably difficult to correct assess, especially the extent of a burn. Despite different tools as the “Rule of Nine” (body area divided into multiples of 9% body surfaces), the “Rule of Palm” (Patient’s palm, fingers included, approximates 1% of body surfaces), the Lund & Browder chart (detailed, age-specific body areas) and different more technical solutions. Often inaccurate estimations are done which thus affect the treatment. This depth and extent estimation is usually performed when the patient is admitted. However, it is known that burns change appearance during the first few days of care. In our Burn Center we have also performed this estimation when the patient is discharged. At this point it is known the true extent and depth of the initial burn. In this retrospective observational study, we compared the burn extent estimated on admission with the one on discharge to investigate whether the initial assessment is accurate. This study highlights the issue of frequent inaccurate burn extent estimations, especially in subgroups as overweight patient or pediatric patients.
Introduction
Estimation of burn extent is crucial for the administration of burn injuries as it determines the level of care (e.g. transfer to specialised burn units) and treatment protocol. Total body surface area burnt (%TBSA), together with age and the presence of inhalation injury, are some of the best-known prognostic factors for mortality in burns.1,2 False estimations frequently lead to unnecessary transfers to burn units/centres and under- or over-resuscitation, an important cause of morbidity and mortality in burn patients. A systematic literature review of over 26 articles by Pham et al. 3 found %TBSA miscalculations up to threefold. %TBSA for smaller burns was generally overestimated and for larger burns underestimated.
Some established methods for estimation of %TBSA burnt, either alone or in combination, are ‘Rule of Palm’, ‘Rule of Nines’ and ‘Lund and Browder Chart’.4–6 An elementary method of estimating the extent of a burn is to use the patient’s hand (palm and palmar surfaces of the five digits) as a reference for approximately 1% of the body surface according to the Rule of Palm. As a hand actually represents only about 0.7% of the body surface in females and 0.8% in males, the method overestimates %TBSA. 4 This method also frequently leads to inaccurate estimations of %TBSA in patients with excessive body mass index (BMI). 7
Due to different proportions of body areas in children, the Rule of Nines is only applicable for adults. The Lund and Browder chart is often considered the gold standard for the estimation of TBSA (Figures 1 and 2). 6
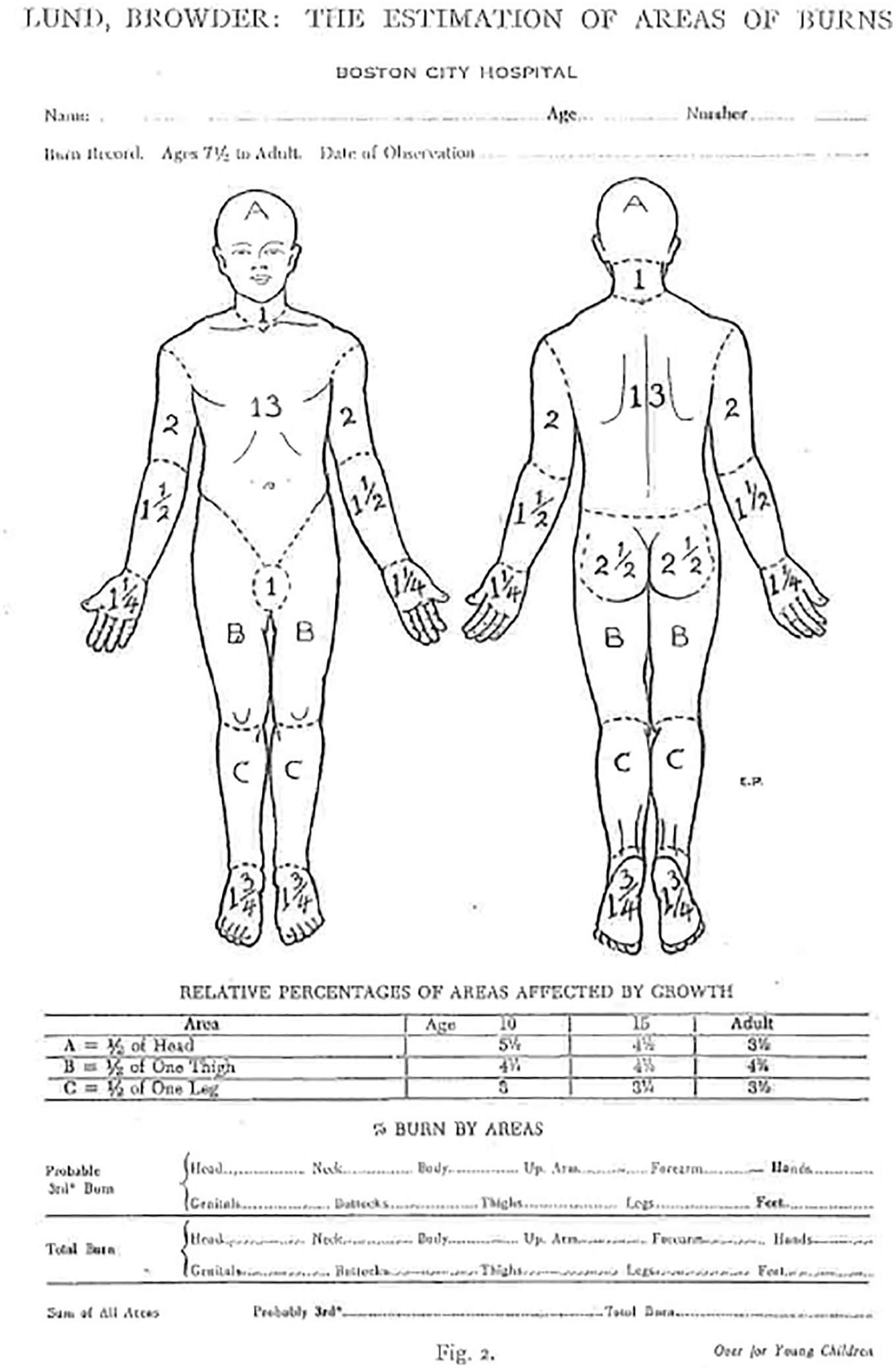
An illustration from the original Lund and Browder Chart from 1944. 6

An illustration from the original Lund and Browder Chart from 1944. 6
As traditional methods are calculated based on average-weight males, they often give incorrect results for other patient groups and are highly variable and dependent on the experience of the estimator.8–10 In recent years, alternative methods for estimating the extent of burns have been developed to minimise the impact of human error. Computer-assisted methods, such as Burn Case 3D® (RISC Software GmbH, Hagenberg, Austria), are considered reliable and are often used as comparison when studying the reliability of other methods. Using technology-assisted methods, laymen have been described to calculate the burn extent more consistently and accurately than most healthcare personnel working with burns on a daily basis. 11 Multiple studies have found a significant improvement in objectivity and quality of burn injury management with technology-assisted methods compared to traditional methods.8,11,12
Two groups, in which the estimation of %TBSA has previously been shown to be particularly challenging, are obese and paediatric patients. Obesity leads to an increase of the total body surface and changes in skin distribution with relatively more skin surface on the trunk and less on the extremities. Since BMI is usually not accounted for, traditional methods underestimate %TBSA of the trunk and overestimate that of the extremities. 13
Children have a proportionally larger head and neck and smaller lower extremities. The proportions change with age and therefore age-appropriate tools for estimating %TBSA burnt should be used to avoid overestimations (Tables 1 and 2).14,15
Body proportions according from Rule of Nines, adapted from Knaysi et al. 5

Classification of BMI, adapted from Butz et al. 32

BMI, body mass index.
A debated question regarding burn injuries is whether there are differences between men and women. A large study on trauma patients in the United States found that men have an increased risk of developing life-threatening complications and death after traumatic injuries, but women suffering from life-threatening complications had higher risk of death. 16 Regarding thermal injuries, clinical studies have surprisingly found that female patients have generally worse outcomes and up to 50% higher risk of death.17,18
Other studies claim that there are no gender-based differences in mortality rates.19,20 The arguments are many, with one possible explanation being that errors in estimating the extent of the injuries, such as the ‘Rule of Palm’, gives the same estimations to both genders despite different body proportions. 4
Aim of the study
At Uppsala University Hospital’s burn centre, %TBSA is systematically estimated at both admission and discharge. Both estimations are done by burn professionals. The %TBSA at discharge is considered a validated estimate as the injuries are healed, and it is known which parts were deep and needed surgery and which were uninjured or superficial and could heal spontaneously. No previous studies, to our knowledge, have compared %TBSA at intake with a validated %TBSA at discharge. Instead, most studies use results of computer-based methods or, if the first estimation is done by a non-burn professional, a burn professional’s estimation as the validated %TBSA. The aim of this study was to compare the estimation of %TBSA burnt at admission to the burn centre and the validated %TBSA at discharge to determine the accuracy of the initial estimation.
Methods
Study population
The Uppsala University Hospital burn centre’s registry contains information on patient identity, age, gender, dates of admission and discharge, type of injury and %TBSA estimated at the admission and discharge of the patient.
Patients admitted between 2010 and 2018 were selected for inclusion in this study (n = 863). From this group, 42 were excluded due to non-burn injuries (Toxic Epidermal Necrolysis [TEN], Staphylococcal scaled skin syndrome [SSSS], Lyell’s disease) and 99 due to missing data on %TBSA, leaving 722 patients for inclusion in the analysis. The anonymised study-register consisted of three parameters: gender (female/male); age (0.0–93.6 years); and the estimation of %TBSA at admission and discharge. A fourth parameter, BMI, was obtained from patient records for 321 patients.
Study design
This study is a retrospective observational study based on the inpatient registry at Uppsala University Hospital’s burn centre.
Data analysis
The data were analysed with SPSS Software (IBM Corp., Armonk, NY, USA). The patients were divided into subgroups based on age, gender and the extent of the burn injury (%TBSA). The age groups were termed baby (<1 year), young (1.0–17.9 years) and adult (>18 years). The %TBSA groups were termed small (<10%), medium (10.0%–19.9%) and large (⩾20%). Gender was subcategorised as female and male. Only patients aged over 18 years with normal (18–24.9 kg/m2) or excessive (>25 kg/m2) BMI were included in the analysis based on BMI, due to the insufficient number of patients in the paediatric category.
For the multifactorial analysis, 18 specific subgroups were made by combining the different groups within the variables: age; gender; and %TBSA. In order to minimise the risk of false results, the minimum group size was determined to 10, and any smaller groups were excluded. This resulted in disqualifying five of the subgroups, leaving 695 patients to the analyses. For each subgroup, mean and median value, as well as standard deviation were calculated. The %TBSA at admission (inTBSA) was compared to the validated %TBSA (valTBSA) to calculate number of patients that were underestimated (inTBSA < valTBSA), overestimated (inTBSA > valTBSA) and estimated correctly (inTBSA = valTBSA). Results are presented as mean (range) if not otherwise stated.
For the analysis based on BMI, the patients were divided into 12 groups (e.g. female with %TBSA >20% with BMI >25). In addition, in this case, the minimum size of a group was determined to 10, leaving nine groups with a total of 312 patients, for the analyses. Further, for these subgroups, mean and median values, and standard deviation were calculated, and the %TBSA at admission was compared to the validated %TBSA.
Ethical permission
The Swedish Ethical Review Authority waived the necessity of a formal ethical approval.
Results
Of the 30 subgroups in total, 26 had over 10 patients and thus fulfilled the criteria for analysis. In total, data on 695 patients were analysed. Thirteen groups were included in the multiple factor analyses and 11 groups in the BMI-based analyses. The summary of the multiple factor analysis can be found in Tables 3–10 and the summary of the BMI-based analysis can be found in Tables 11 and 12.
Results for the groups in the infant category.*

In total, 12% of the cases were underestimated when comparing the %TBSA estimation on admission to the %TBSA estimation on discharge; 46% were overestimated and 42% were estimated correctly.
TBSA, total body surface area.
Results for the groups in the young category.*

In total, 12% of the cases were underestimated when comparing the %TBSA estimation on admission to the %TBSA estimation on discharge; 36% were overestimated and 52% were estimated correctly.
TBSA, total body surface area.
Results for the groups in the adult category.*

In total, 29% of the cases were underestimated when comparing the %TBSA estimation on admission to the %TBSA estimation on discharge; 30% were overestimated and 41% were estimated correctly.
TBSA, total body surface area.
Results for the female category.*
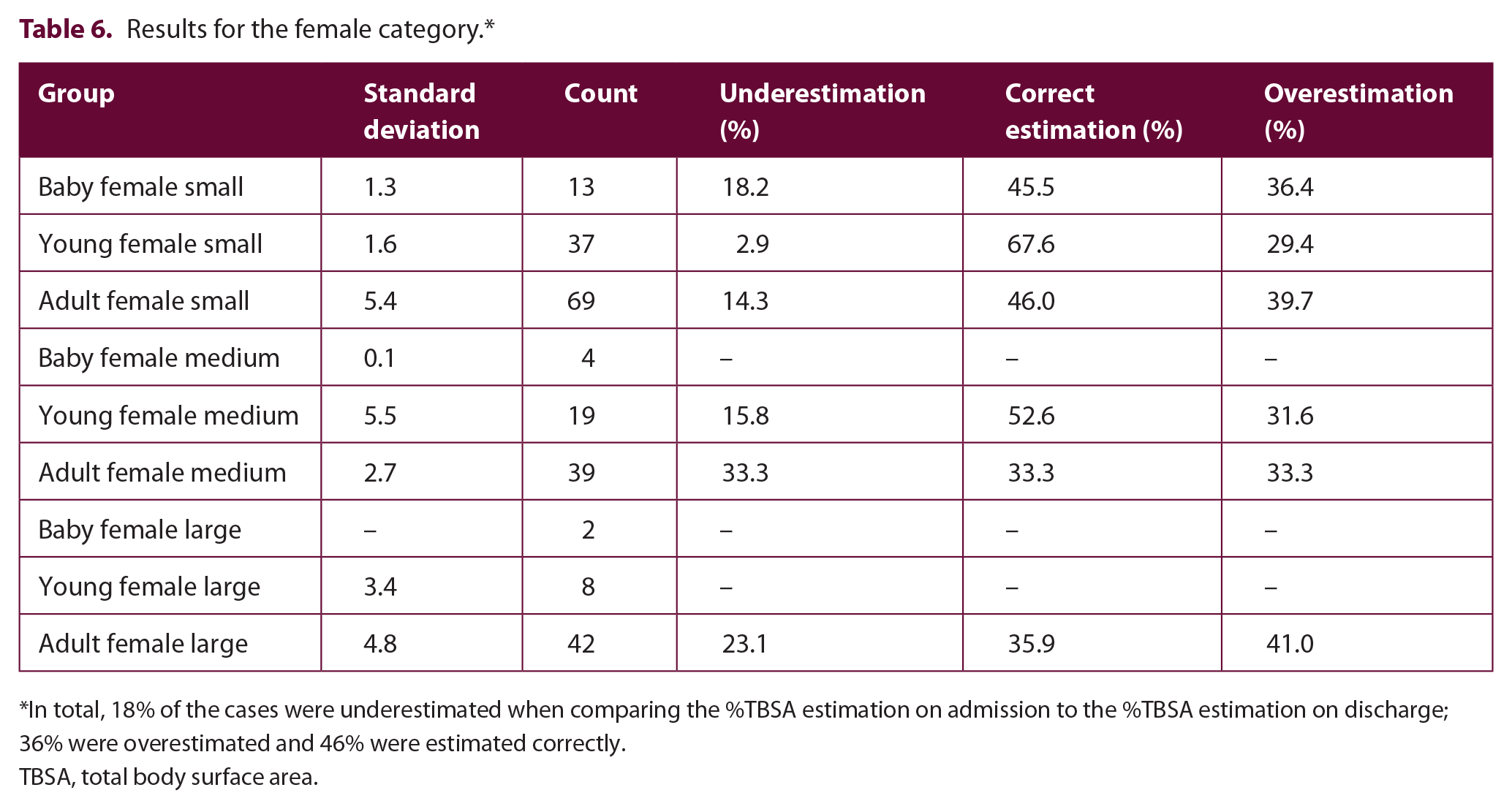
In total, 18% of the cases were underestimated when comparing the %TBSA estimation on admission to the %TBSA estimation on discharge; 36% were overestimated and 46% were estimated correctly.
TBSA, total body surface area.
Results for the male category.*

In total, 25% of the cases were underestimated when comparing the %TBSA estimation on admission to the %TBSA estimation on discharge; 31% were overestimated and 44% were estimated correctly.
TBSA, total body surface area.
Results of the small category.*

In total, 13% of the cases were underestimated when comparing the %TBSA estimation on admission to the %TBSA estimation on discharge; 36% were overestimated and 51% were estimated correctly.
TBSA, total body surface area.
Results of the medium category.*

In total, 28% of the cases were underestimated when comparing the %TBSA estimation on admission to the %TBSA estimation on discharge; 29% were overestimated and 43% were estimated correctly.
TBSA, total body surface area.
Results of the large category.*

In total, 37% of the cases were underestimated when comparing the %TBSA estimation on admission to the %TBSA estimation on discharge; 31% were overestimated and 32% were estimated correctly.
TBSA, total body surface area.
Results of the normal BMI category.*

The tendency of over- and underestimation was similar in the subgroups with normal and excessive BMI. In the normal BMI category, 26% of the cases were underestimated when comparing the %TBSA estimation on admission to the %TBSA estimation on discharge; 30% were overestimated and 44% were estimated correctly.
BMI, body mass index; TBSA, total body surface area.
Results of the excessive BMI category.*

In total, 29% of the cases were underestimated when comparing the %TBSA estimation on admission to the %TBSA estimation on discharge; 33% were overestimated and 38% were estimated correctly.
BMI, body mass index; TBSA, total body surface area.
Multiple factor analysis
%TBSA was overestimated in 9 (69%) and underestimated in 4 (31%) out of 13 groups; however, both under- and overestimation occurred in all the groups. In only four groups (31%) %TBSA was estimated correctly in more than 50% of the cases. The results for each group are shown in the separate tables.
The first variable studied variable was age (baby, young and adult).
In the baby category, four groups were excluded. In the two analysed groups, a total of 12% (n = 3, 10.0%–18.2%) were underestimated and 46% (n = 11, 36%–50%) were overestimated. In 42% (n = 10, 40.0%–45.5%) %TBSA was estimated correctly (Table 3).
In the young category, five out of six groups were analysed. In all groups, a total of 12% (n = 22, 2.9%–20.6%) were underestimated, 36% (n = 67, 26.5%–45.3%) were overestimated and 52% (n = 96, 41.7%–67.6%) were estimated correctly (Table 4).
All groups in the adult category were analysed. The tendency for over- and underestimation differed between the groups, but in total, 29% (n = 121, 14.3%–43.4%) were underestimated, 30% (n = 124, 26.4%–41.0%) were overestimated and 41% (n = 172, 30.2%–53.8%) were estimated correctly (Table 5).
The second variable studied was gender. Altogether, three female groups and two male subgroups were excluded.
Of the six female groups, one presented equal results for under- and overestimations, and in all other groups overestimation was more common. In total, 18% (n = 39, 2.9%–33.3%) of the female cases were underestimated, 36% (n = 79, 29.4%–41.0%) were overestimated and 46% (n = 101, 33.3%–67.6%) were estimated correctly (Table 6).
In the male groups, underestimation was more common in two groups and overestimation in the rest of the groups. In total, 25% (n = 117, 9.4%–43.4%) of the male cases were underestimated, 31% (n = 150, 26.4%–50.0%) were overestimated and 44% (n = 209, 30.2%–53.8%) were estimated correctly (Table 7).
When comparing corresponding groups according to age and %TBSA, the results were similar for both genders except for the groups of adults with large-sized burns where the extent of the injury was more commonly overestimated in the female group but underestimated in the male group.
The third variable was %TBSA (small, medium and large).
All small groups were analysed, and overestimation was more common than underestimation. In total, 13% of the cases (n = 46, 2.9%–18.2%) were underestimated, 36% (n = 126, 29.4%–50.0%) were overestimated and 51% (n = 180, 40.0%–67.6%) were estimated correctly (Table 8).
Two of the medium groups were disqualified. In the remaining groups, underestimation was more common in one, equal results were presented in one and overestimation was more common in two. In total, 28% of the cases (n = 47, 15.8%–33.3%) were underestimated, 29% (n = 49, 26.5%–33.3%) were overestimated and 43% (n = 74, 33.3%–52.9%) were estimated correctly (Table 9).
Out of the large groups, three were disqualified. In the remaining groups, underestimation was more common in one group and overestimation in two groups. In total, 37% of the cases (n = 63, 16.7%–43.4%) were underestimated, 31% (n = 54, 26.4%–41.7%) were overestimated and 32% (n = 56, 30.2%–41.7%) were estimated correctly (Table 10).
BMI-based analysis
In this analysis, six groups of patients with normal BMI and six groups of patients with excessive BMI were examined. One group was excluded.
Among patients with normal BMI, underestimation was more common in two groups, overestimation in two groups and one group presented equal results. In total, 26% of the cases (n = 31, 16.7%–52.0%) were underestimated, 30% (n = 36, 20.0%–37.8%) were overestimated and 44% (n = 52, 28.0%–50.0%) were estimated correctly (Table 11).
In the groups with excessive BMI, overestimation was more common in all the female groups and in one of the male groups. Underestimation was more common in two groups. In total, 29% of the cases (n = 56, 6.7%–47.9%) were underestimated, 33% (n = 63, 25.0%–46.7%) were overestimated and 38% (n = 73, 26.7%–51.2%) were estimated correctly (Table 12).
Discussion
The aim of this study was to evaluate the accuracy of the %TBSA estimation at admission compared to the validated %TBSA at discharge in different patient groups at the Uppsala University Hospital’s burn centre. At the burn centre, all estimations are made by dedicated burn surgeons both at admission and discharge, generally using the Lund and Browder chart. The estimation of %TBSA at admission is critical for determination of the patients’ need for fluid resuscitation and treatment protocol (for example, timing of surgery). Differing from most other burn centres, %TBSA is also estimated at discharge when the injuries have healed and/or been treated. At this point, it is obvious which parts required surgery (deeper burns), which healed spontaneously (superficial burns) and which areas were unaffected, making it easier to make an exact estimation of the extent of the injuries. Interestingly, this study indicated that even burn professionals make false initial estimations in all patient groups.
Paediatric patients
Previous studies have indicated that %TBSA is often overestimated in paediatric patients.15,21,22 The literature describes a higher percentage of overestimation in children aged under 36 months. 9 Children have nearly three times the body surface area to body mass ratio of adults, which explains why many methods estimate %TBSA inaccurately in paediatric patients. The Lund and Browder chart was originally developed so that the different body surface areas in different age groups could be taken into consideration. 23 It is still used as the gold standard, even though it has not been updated since 1944. Saffle et al. 24 described patients receiving erroneously high volumes of resuscitation fluids because of inaccurate estimation of %TBSA, which can lead to events such as compartment syndrome. All cases of excessive fluid resuscitation in paediatric patients lead to significant complications. 25 . A study from 1993 describes the issue of overestimation in the paediatric population in the burn assessment when burns are >5% TBSA, comparing children with smaller burns. 26 This issue of determining %TBSA of burns in paediatric patients need to be addressed.
In this study, paediatric patients were present in two groups, ‘baby’ (aged < 1 year) and ‘young’ (aged 1–18 years). Originally, the intention was to divide paediatric patients into multiple, more specific age groups, but due to too small group sizes some had to be combined. Even then, only two baby groups could be analysed, making the results uncertain. In these groups, overestimation (n = 11, 46%) was dominant compared to underestimation (n = 3, 13%), which is a similar finding compared to previous studies. In the young groups, 36% (n = 67) were overestimated and 14% (n = 25) were underestimated. In light of these results, we can assume that the estimations on paediatric patients are often overestimated even by burn professionals at the Uppsala University Hospital’s burn centre. Further studies are required to investigate the age-specific estimations.
TBSA
The size of the burn affects the accuracy of the %TBSA estimation. The accuracy of the estimation of burns are not always without errors. Studies have shown a pattern of underestimating large (TBSA > 20%) and overestimating small (TBSA < 20%) burns, leading to excessive fluid resuscitation of patients with small injuries and insufficient of patients with large injuries.9,27 Many physicians use the patient’s hand to estimate the burn extent, but there is small concordance whether the fingers should be included in the assessment.4,28
In this study, patients were divided into three groups based on the validated %TBSA: small (TBSA < 10%); medium (TBSA 10.0%–19.9%); and large (TBSA 20%–100%). In the BMI analysis, 41% were underestimated and 27% were overestimated. All in all, small injuries were more often overestimated and large injuries were slightly more often underestimated.
It is not only the size of the injury that matters for the accuracy of the estimation. A study by Wachtel et al. 23 found that irregular burns and burns on the trunk and thighs have greater variability than more evenly distributed burns and burns on other parts of the body. The same study showed that burn experts do not always have more accurate estimations compared to less experienced healthcare workers. The advantage of the experts was less variability of the results. In this study, it is essential to notice that all %TBSA estimations, both before and after the treatment, were made by dedicated burn surgeons. In many other studies, the experts’ estimations are used as the validated %TBSA and the studied estimations are made by non-burn doctors before referral to the burn unit. 21 In these cases, some of the inaccurate estimations might simply be explained by the lack of practice and routine. 28
Differences between genders
We could find no previous studies examining the differences in %TBSA estimations between male and female patients at admission and discharge. There are, however, studies focusing on burns and gender. A study by Rossignol et al. 29 showed that men were 2.6 times more likely to get a burn injury than women. In addition, the type of injury varied; women more commonly suffered from scald burns and men from flame or flash burns. 29 Of the 821 burn patients included in this study, before excluding patients with missing data on %TBSA, 264 were female and 557 male, making burn injuries approximately 2.1 times more common in male patients. Many studies have also examined the outcome of burn injury treatment in different genders.16–20 Some of these studies found that women have higher mortality rates than men whereas others found no gender-based difference. This was also studied on small animal models, describing a difference in the immune response after thermal injury between the genders. 31 Gregory et al. 31 could demonstrate a delayed cell-mediated function in female mice, suggesting it increased mortality because of the delayed initiation of cell-mediated immune response in a female with a thermal injury.
In this study, we found no clear differences in the estimations between genders. Some groups, for example adult patients with large %TBSA, presented different results between genders (underestimation being more common for male patients but overestimation for female patients), but there did not seem to be a pattern (for example, for the other large groups or adult groups the results did not vary as much). Further studies are required to confirm this finding, but we can assume that gender does not affect the estimation of TBSA as much as other factors (age, BMI and burn extent).
BMI
BMI is convenient and widely used to categorise a person as normal, under-, or overweight although it does not consider body composition and can therefore incorrectly classify individuals. Obesity (BMI > 30 kg/m2) is a well-known factor causing inaccurate estimations of %TBSA. When using the Rule of Palm, the injuries are overestimated as the relative palmar surface area decreases when BMI increases due to changing body proportions.7,32 It can be difficult to calculate the body surface area in obese patients; the DuBois-DuBois formula, which is described to be more accurate for the obese population, can be used for this purpose. 30 Other studies suggest that using a 3D scanner to measure the body surface area in the obese population is much simpler than other methods. 33
Obesity is also a known risk factor for increased morbidity and mortality among burn patients usually associated with diabetes, heart diseases and other related health disorders.34–36 As described above, it is known that the obese patients have higher recurrence of inaccurate estimations of %TBSA. The intention with this study was not to describe the best type of formula that can be used, but to investigate if there are any difference in the estimation of %TBSA in obese patients before and after discharge.
In this study, patients were divided into only two weight groups, normal (BMI 18–24.9 kg/m2) and overweight (BMI > 25 kg/m2). Surprisingly, overestimation was not clearly more common for the overweight patients than for the normal weight patients. This might be explained by the fact that the estimations are made by burn professionals using the Lund and Browder chart. Another explanation might be that the overweight groups possibly included several patients with only minor overweight, which does not affect body proportions such as obesity. In the future, having larger patient groups and dividing patients into more weight-specific groups (for example, using the classification in Table 2) could give more precise results. It would also be interesting to include a group of underweight patients and paediatric patients with abnormal BMI.
Sources of error
One problem with this study was the relatively low number of patients for such a high number of subgroups making the analysed groups very small. For the statistical analysis, low quantity means high risk for false-positive results and unsure reliability. In the future, a similar study with an extended study population from a longer timespan could give more exact information on the accuracy of the estimations of %TBSA. Another interesting study would be comparing the results between different decades to see if the estimations have become more accurate at the burn centre.
Inescapably, it must be remembered that all burn wounds tend to be dynamic, and the initial assessment can be associated with some degree of errors.
Conclusion
To accurately assess the %TBSA of burns remains clinically important and difficult. In conclusion, we can state that small injuries were more often overestimated than larger injuries. There do not seem to be large differences in estimations based on the gender of the patient. As this study is pioneering in comparing estimations between male and female patients, more studies are required to verify the results. For paediatric patients, overestimation was more frequent than for adult patients. The inaccuracy in the estimation of %TBSA in children remains a reason why we recommend a careful accurate approach when calculating %TBSA in the paediatric population to avoid over- and under-resuscitation. This study indicates that even burn professionals often make false estimations on %TBSA. Therefore, increased education and training are recommended, both for non-burn professionals working with burn injuries and experienced burn professionals to improve accurate estimation in the future. As many studies, including this one, have shown a high number of false %TBSA estimations using traditional methods, it is important to speculate whether these methods should be re-studied and updated, especially for paediatric and obese patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.