
Abstract
Introduction:
The ageing global population presents a novel set of challenges for trauma systems. Less research has focused on the older adult population with burns and how they differ compared to younger patients. This study aimed to describe, and compare with younger peers, the number, causes and surgical management of older adults with burn injuries in Australia and New Zealand.
Methods:
The Burns Registry of Australia and New Zealand was used to identify patients with burn injuries between 1 July 2009 and 31 December 2018. Temporal trends in incidence rates were evaluated and categorised by age at injury. Patient demographics, injury severity and event characteristics, surgical intervention and in-hospital outcomes were investigated.
Results:
There were 2394 burn-injured older adults admitted during the study period, accounting for 13.4% of adult admissions. Scalds were the most common cause of burn injury in older adults. The incidence of older adult burns increased by 2.96% each year (incidence rate ratio = 1.030, 95% confidence interval = 1.013–1.046, P < 0.001). Compared to their younger peers, a smaller proportion of older adult patients were taken to theatre for a surgical procedure, though a larger proportion of older adults received a skin graft.
Discussion:
Differences in patient and injury characteristics, surgical management and in-hospital outcomes were observed for older adults. These findings provide the Australian and New Zealand burn care community with a greater understanding of burn injury and their treatments in a unique group of patients who are at risk of poorer outcomes than younger people.
Lay Summary
The number and proportion of older persons in every country of the world is growing. This may create challenges for healthcare systems. While burn injuries are a unique subset of trauma that affect individuals of all ages, less is known about burns in older adults and how they differ from younger patients.
We wanted to look at the number, type, management, and outcomes of burns in older adults in Australia and New Zealand. To do this, we used data from the Burns Registry of Australia and New Zealand, or BRANZ. The BRANZ is a database that collects information on patients that present to Australian and New Zealand hospitals that have a specialist burns unit.
Our research found that one in eight adult burns patients was over the age of 65, and that the rate of burn injuries in older adults has increased over the last decade. Older adult burns patients were most commonly affected by scalds after coming in contact with wet heat such as boiling liquids or steam. Fewer older adults went to theatre for an operation or surgical procedure compared to their younger counterparts. However, a larger proportion of older adults that went to theatre had a skin graft (where skin is removed from an uninjured part of the body and placed over the injured part).
This research provides important information about a unique and growing group of patients to the local burn care community. It also highlights potential avenues for injury prevention initiatives.
Introduction
The global population is ageing, with people living for longer than in previous periods in history. 1 In addition, people are remaining in better health and are more active as they age. This is partly due to improvements in medical care and an enhanced understanding of the importance of lifestyle factors. 2 In the coming decades, there will be large increases in the proportion of the population that will be over the age of 65 years. 3 Within Australia alone, projections estimate that there will be eight million people over the age of 65 by the year 2054, accounting for 21% of the total population. 3 Similar estimates from the US Census Bureau predict that the proportion of the population in the Western world over the age of 65 will double within the next 20 years. 4
Burn injuries are a significant cause of trauma worldwide5,6 and affect people of all ages. 7 A higher proportion of older adults with burn injuries (relative to the age distribution of the general population) is observed, 4 which may be due to the fact that older adults are more vulnerable to burn injuries. 8 Another complicating factor is the thinner atrophic skin of older adults, 4 which results in deeper and more severe burns 9 that take longer to heal.10,11 Decreasing physical strength, poorer reaction time, and abuse and neglect have also been suggested as contributors to the increased vulnerability of older adults. 12 This overrepresentation may also be due to the possibility that older adults are more active than previously thought and are engaging in activities that may lead to a burn injury. Previous literature varies as to the age cut-off for ‘older adult’, but 65 years is the most widely recognised classification. 13 The World Health Organization (WHO) has noted that 65 years of age is the most widely accepted lower limit for the term ‘older adult’ or ‘elderly’. 14 Several studies have shown that mortality is higher in older burns patients compared to younger patients.15–18 However, studies examining burn injury in older adults have predominantly been single-centre studies, limiting their ability to generalise to the wider older adult population. 19
Little is known about the prevalence, causes, management and outcomes of older adults in Australian and New Zealand burns units. In particular, there is yet to be an examination of potential differences in patients over the age of 65; that is, comparing different groups of patients over the age of 65, rather than grouping all older adults together. The aims of this study were to describe temporal trends in the prevalence, causes, surgical interventions and in-hospital outcomes of burn injuries in older adults in Australia and New Zealand.
Methods
Study setting and design
Australia and New Zealand have a combined population exceeding 29 million people.20,21 Specialist burn care in Australia and New Zealand is provided by 17 burn units across the two countries. Adult patients (i.e. aged 18 years and older) who sustained a burn injury and were admitted to a specialist burns unit between 1 July 2009 and 31 December 2018 were identified from the Burns Registry of Australia and New Zealand (BRANZ). The BRANZ is a clinical quality registry that has collected epidemiological, quality of care and in-hospital outcome data for adult and paediatric burns patients across Australia and New Zealand since July 2009. Admissions to a designated burns unit that occur within 28 days of injury are recorded by the BRANZ. These admissions are recorded on the provision that the patient is: (1) admitted to hospital for > 24 h; (2) admitted to hospital for < 24 h but requires a burn management procedure in theatre; or (3) admitted to hospital and dies within 24 h. Admissions that do not meet these criteria, desquamating skin conditions and extravasation injuries are not included in the BRANZ. While the BRANZ has previously piloted long-term outcome data collection,22–24 the registry does not currently collect quality of life or long-term survival data. Therefore, this study only examines the in-hospital management and outcomes of burn injuries. An older adult was defined as 65 years of age or older, consistent with previous research. 13 Data relating to the first admission to a specialist burns unit with a new burn injury were extracted. Patients who were discharged from one specialist burns unit to another were excluded from the current study, as were patients whose age at time of injury could not be calculated. Since 2009, the BRANZ has collected data relating to the decision to withdraw or withhold medical treatment for patients whose injuries were deemed non-survivable and when this decision was made. For this study, we identified whether patients who perished in hospital were palliated before their death or whether they received active treatment until they died. Ethical approval for this study was granted by the Monash University Human Research Ethics Committee (Project no. CF08/2431-2008001248) before final approval by the BRANZ Steering Committee.
Statistical analysis
Age at the time of injury was divided into age ranges for older adults, consistent with reports from the Australian Institute of Health and Welfare 25 : 65–74 years; 75–84 years; and ⩾ 85 years. Patient age for all other adults was categorised as 18–64 years. The comorbid status of patients was defined using the Charlson Comorbidity Index (CCI), mapped from International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, Australian Modification (ICD-10-AM) codes, with a CCI weighting of zero representing no CCI condition.26,27 Descriptive comparisons of demographic, burn injury event, and injury characteristics between the age groups were made using chi-square and Kruskal–Wallis tests as appropriate.
Population-based incidence rates and 95% confidence intervals (CIs) were calculated for each year based on the total population at 30 June for the years 2010–2018. Annual population estimates were obtained from the Australian Bureau of Statistics 20 and Statistics NZ. 21 Poisson regression models were used to determine whether the incidence rate increased or decreased over the nine-year period for all older adults who had sustained a burn injury, and for each age group. Incidence rate ratios (IRRs) and 95% CIs were calculated. Patients admitted to a specialist burn unit between 1 July 2009 and 31 December 2009 were excluded from incidence calculations as a complete calendar year of admissions data was not available.
The surgical interventions of interest were whether the patient underwent any type of acute surgical procedure (including dressing-related procedures performed in theatre) and, for the patients who underwent a surgical procedure, whether they received a skin graft. The in-hospital outcomes of interest were admission to the intensive care unit (ICU), length of stay (LOS) in the ICU, in-hospital LOS, in-hospital mortality and discharge disposition (for patients surviving to discharge). Surgical intervention and in-hospital outcomes were compared between the age groups using chi-square and Kruskal–Wallis H tests as appropriate. All analyses were conducted using Stata 14. 28 A P value < 0.05 was considered significant. Figures were produced in the R statistical environment version 3.6.1 29 using the ‘ggplot2’, 30 ‘tidyverse’, 31 and ‘cowplot’ 32 packages.
Results
Over the nine-year study period, 17,821 burn injury admissions were recorded by the registry. Of these, 2394 (13.4%) were older adults. With increasing age, the proportion of women and scalds increased and the proportion of flame burns decreased (Table 1). The most common sub-causes of burn injuries across the four age groups are listed in Supplementary Table 1. Total burn size and depth was consistent across age groups, as was the proportion of unintentional injuries (Table 1). Older adult burn patients had a greater full thickness percentage total body surface area (%TBSA) compared to the younger adults (Table 1). The proportion of injuries occurring in the home (or usual place of residence) increased with age, as did the proportion of patients with CCI index weights greater than zero (Table 1). The proportion of patients admitted to a specialist burns unit directly from the scene increased with age, while the proportion of patients self-admitting to a specialist burns unit or being admitted via the emergency department or outpatient clinic decreased with age (Table 1).
Demographic, event and injury characteristics for adults with burn injuries.
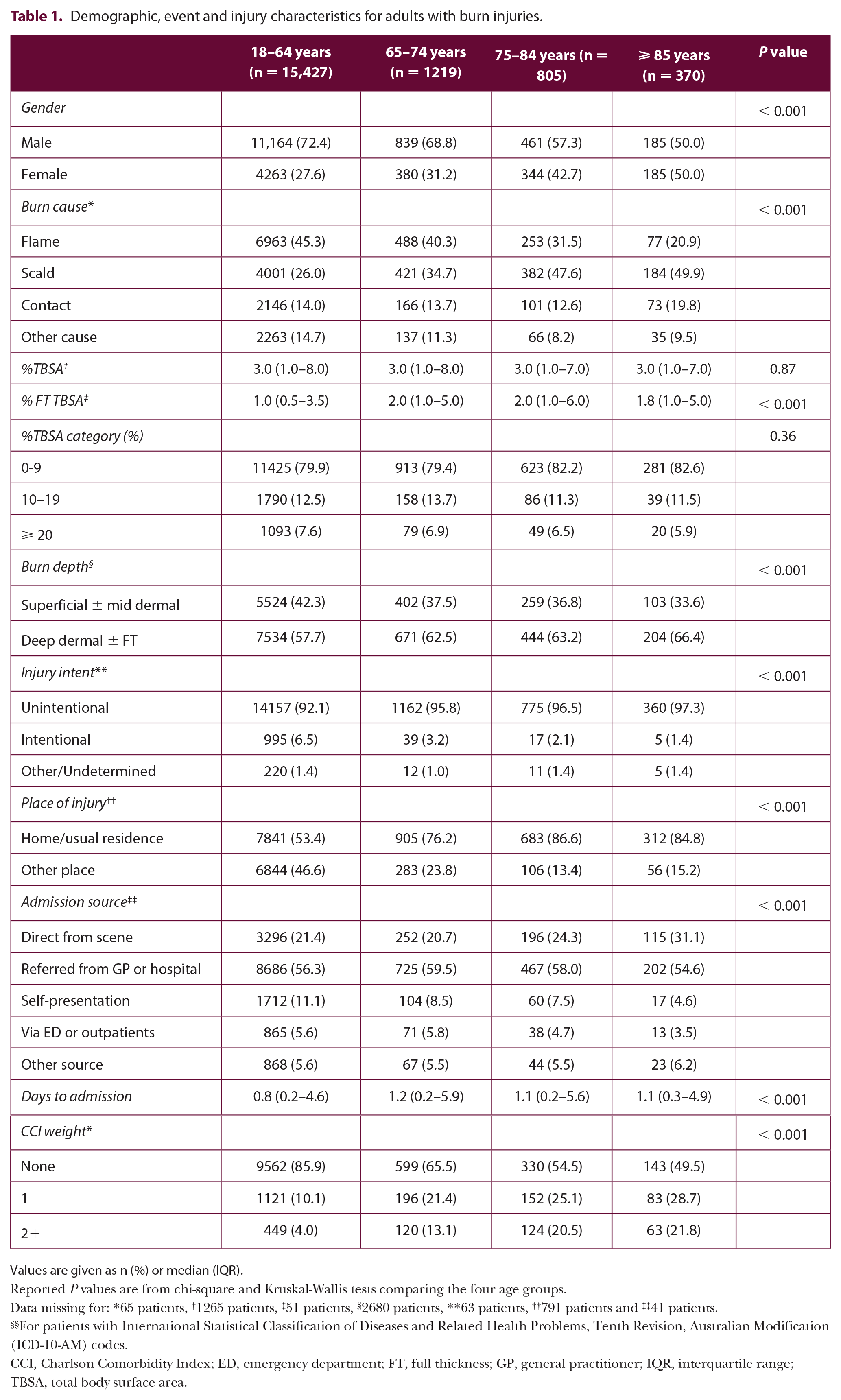
Values are given as n (%) or median (IQR).
Reported P values are from chi-square and Kruskal-Wallis tests comparing the four age groups.
Data missing for: *65 patients, †1265 patients, ‡51 patients, §2680 patients, **63 patients, ††791 patients and ‡‡41 patients.
For patients with International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, Australian Modification (ICD-10-AM) codes.
CCI, Charlson Comorbidity Index; ED, emergency department; FT, full thickness; GP, general practitioner; IQR, interquartile range; TBSA, total body surface area.
Temporal trends
The proportion of older adults with a burn injury increased from 10.9% (n = 82) in 2009 to 13.2% (n = 309) in 2018 (Figure 1). The proportion of older adult patients aged ⩾ 85 years decreased from 2.0% in 2009 to 1.5% in 2018. The incidence of burn injuries in older adults increased by 3.0% each year (IRR = 1.03, 95% CI = 1.01–1.05, P < 0.001; Figure 2). This rate was greater than in patients aged 18–64 years, in whom the incidence increased by 2.9% each year (IRR = 1.03, 95% CI = 1.02–1.04, P < 0.001; Figure 3). The incidence of burn injuries increased in two of the older age groups: 2.9% in patients aged 65–74 years (IRR = 1.03, 95% CI = 1.01–1.05, P = 0.011) and 4.2% in patients aged 75–84 years (IRR = 1.04, 95% CI = 1.01–1.07, P = 0.003; Figure 3). There was no change in the incidence of burn injuries in patients aged ⩾ 85 years (IRR = 1.01, 95% CI = 0.97–1.05, P = 0.70; Figure 3).

Distribution of adult burn injuries in Australia and New Zealand by age group between 2009 and 2018.

Changes in the incidence of burn injuries in older adults, overall and by primary injury cause, in Australia and New Zealand between 2010 and 2018. Data are presented as incidence rates and 95% confidence intervals. Data from 2009 are not shown as a complete calendar year of admissions data was not available.

Changes in the incidence of burn injuries in Australia and New Zealand by age group between 2010 and 2018. Data are presented as incidence rates and 95% confidence intervals. Data from 2009 are not shown as a complete calendar year of admissions data was not available.
When focusing specifically on the primary cause of the burn injury in older adults, increases in the incidence of flame (IRR = 1.04, 95% CI = 1.01–1.06, P = 0.011) and contact (IRR = 1.05, 95% CI = 1.01–1.09, P = 0.029) burns were observed over time (Figure 2). The incidence of scalds (IRR = 1.02, 95% CI = 0.99–1.04, P = 0.18) and burns from other causes (IRR = 1.03, 95% CI = 0.98–1.08, P = 0.28) in older adults remained relatively unchanged since the implementation of the BRANZ (Figure 2).
Surgical intervention after burn injuries
The proportion of patients requiring a procedure in theatre decreased with age (Table 2). Of the patients admitted to theatre, the proportion receiving a skin graft or amputation increased with age (Table 2). This result did not change appreciably after excluding patients who were palliated (Supplementary Table 2).
Surgical intervention after burn injury.

Values are given as n (%).
Reported P values are from chi-square and Kruskal–Wallis tests comparing the four age groups.
Data missing for: *180 patients and †95 patients.
In-hospital outcomes after burn injury
The proportion of patients admitted to the ICU (12.7% of all patients) was not different across age groups; neither was the median ICU LOS (Table 3). The median hospital LOS increased from 4.7 days for patients aged 18–64 years to 12.3 days for patients aged ⩾ 85 years (Table 3). The overall in-hospital mortality rate for all admissions was 1.7%, increasing with age from 1.1% of patients aged 18–64 years to 10.0% in patients aged ⩾ 85 years (Table 3 and Figure 4). Most patients who survived were discharged to their home or usual place of residence (83.7%), but this proportion decreased with age (Table 3 and Figure 4). The proportion of surviving patients who were discharged to another hospital, unit or service increased with age (Table 3 and Figure 4). Similar results for all in-hospital outcomes were observed after excluding patients who were palliated (Supplementary Table 3).
In-hospital outcomes after burn injury.

Values are given as n (%) or median (IQR).
Reported p values are from chi-square and Kruskal–Wallis tests comparing the four age groups.
Data missing for: *90 patients, †7 patients, ‡11 patients and §6 patients.
For patients surviving to discharge.
ICU, intensive care unit; IQR, interquartile range; LOS, length of stay.

Discharge disposition for adult patients with burn injuries by age group in Australia and New Zealand between 2009 and 2018.
Discussion
This study investigated the comparative epidemiology, causes, surgical intervention and in-hospital outcomes of burn injuries in older adults over a nine-year period. The proportion of older adults with a burn injury increased from 10.9% of patients in 2009 to 13.2% of patients in 2018. There were differences in the demographic and injury event profile, surgical intervention and in-hospital outcomes of older adult burn patients compared to younger adult patients. Importantly, the findings from this study help to define the problem and unique characteristics of burn injury in older adults, while also demonstrating that older adults are a high-risk group for poorer in-hospital outcomes. Furthermore, it emphasises the importance of having burn teams that are knowledgeable and skilled in identifying and managing these significantly greater risks in this unique patient group, as well as the valuable support of specialist medical and aged care consultation services that provide expertise and advice on aspects of non-burn related care.
A greater proportion of burn injuries were seen in men compared to women up until 84 years of age, whereby there was a similar proportion of burn injuries in men and women in patients over the age of 85. This finding is consistent with previous studies.33–37 Consistent with previous studies,38–43 flame burns were the most common cause of burn injury in the younger adult population (aged 18–64 years) whereas the proportion of scald injuries increased in older age groups. This mechanism of injury is consistent with the finding that many burns in older adults are sustained during cooking and bathing, 44 as well as spills involving hot drinks. This finding is in contrast to that of a 2009 North American study involving > 180,000 patients over the age of 55 years recorded by the National Burn Repository between 1991 and 2005, where flame burns were the most common aetiology. 19 The discrepancy in this finding may be explained by the fact that almost one-third of the cases in the Pham et al. 19 study had an unknown injury aetiology, a figure much greater than that in this study. It may also be due to Pham et al. including patients aged 55–64 years in their study of older adults.
There was a lack of evidence of a difference in the median %TBSA between age groups in this study. This finding is in contrast to Pham et al., who reported that the mean %TBSA differed between age groups. 19 Similar to Pham et al., this study observed an increase in the size of full thickness burns in older adults. 19 This is consistent with the notion that older adults have thinner atrophic skin, which places them at greater risk of deeper burns. 9 However, direct comparisons should be treated with caution given the differences in statistical analyses and reporting between these studies. In this study, > 80% of burn injuries in the group aged ⩾ 85 years occurred in the home or usual place of residence, an increase from just over 50% in the younger adult group. This finding is consistent with previous studies identifying that burn injuries in younger adults are more commonly the result of a work-related accident.33,37,42,45-47 The proportion of patients with comorbid conditions increased with age, which is consistent with expectations and previous reports.48,49 The increase in the presence of comorbid conditions within the older adult population may also partly explain the increased LOS in hospital, the increased proportion of in-hospital mortality, and the decreased proportion of patients being discharged to their home or usual place of residence in this cohort of patients. The proportion of patients admitted to the ICU did not differ with age, nor did the amount of time patients spent in the ICU.
The finding of an increase in the proportion of older adult burns patients within the registry is consistent with the National Burns Repository study from Pham et al. 19 However, Pham et al. used 55 years as the lower cut-off for an ‘older adult’, which may have contributed to their reported increase. This difference aside, there are several other possible explanations for the observed increase in the incidence of burn injuries in older adults. One such explanation in the context of this study is the growth in the number of burns units contributing adult data to the registry. This number has risen from 12 units when the registry began collecting data in 2009 to 17 units at the time of writing. Another possible explanation is that the global population is ageing, particularly in Western countries. Thus, there is a greater relative number of older adults admitted with burn injuries because there are more older adults who could sustain a burn injury. 1
It is difficult to compare the finding that a smaller proportion of older adult patients are taken to theatre as previous studies tend to report the number of operations patients received.15,19,36,50 The proportion of patients taken to theatre who received a skin graft increased with age, with > 80% of patients aged > 85 years receiving a skin graft. There are a number of possible explanations for this finding. This observation may be explained by a greater proportion of older adult patients having deep dermal or full thickness burns that require surgical management in a more urgent manner compared to younger patients who have superficial dermal to mid-dermal burns. Older adults may also be less likely to receive adequate first aid after their burn injury. 51 A recent study utilising data from the BRANZ found that the application of adequate first aid reduced the probability of requiring a skin graft. 51 Our finding may also be explained by older adults having decreased mobility and balance, 52 spending longer time in contact with the heat source (e.g. falling in the shower and not being able to get up), or delayed presentation to the burn service after attempting to manage their burn themselves or under the guidance of their general practitioner. However, these latter explanations are speculative and further research into these areas are required. As this study only looked at acute admissions data (i.e. relating to the first admission to the hospital), it is also possible that during the initial admission younger patients had their burn covered by a temporary skin closure product and were readmitted at a later date for grafting. Future studies using large, registry-based datasets are required to further investigate the differences in surgical intervention between patients of different age groups and the association with in-hospital outcomes such as LOS and mortality.
The finding that LOS increased with patient age is consistent with previous studies.4,19 One potential explanation for this finding may be the more prevalent physical deconditioning and psychosocial issues associated with older adults that may delay discharge from hospital. For example, older patients take longer to be physically and functionally safe for discharge than younger adults, and the coordination of care to plan for discharge to nursing homes, respite care or rehabilitation facilities is complex with long waiting periods for beds. Issues such as these are not priorities in the intensive care setting and are unlikely to delay discharge from here but could delay discharge from the hospital.
While in-hospital mortality was low (< 2% of all patients), the proportion of patients dying in-hospital increased from 1.1% in patients aged 18–64 years to 10% in patients aged ⩾ 85 years. This finding is consistent with that of Pham et al., 19 although in-hospital mortality was more prevalent in their sample (24.4% of patients aged ⩾ 75 years). This finding is also consistent with other previous studies reporting that the mortality rate is higher in older burns patients compared to younger cohorts.15–18,36 The declining proportion of surviving patients being discharged to their home or usual place of residence and subsequent increase in patients being discharged to other hospitals or healthcare facilities (e.g. rehabilitation centres or nursing homes) is also consistent with Pham et al. 19 and Lundgren et al. 36 There are challenges associated with investigating patients who are discharged to a non-independent living arrangement, such as the broad definition of non-independent living (e.g. living with family who act as carers, living in a nursing home, etc.) and the disposition field definitions in the registry being influenced by the patient’s usual place of residence before their injury. Those challenges aside, these findings may, in part, be explained by the increased prevalence of co-existing or pre-morbid conditions in older individuals.37,49 Pre-existing comorbidities have not only been identified to increase susceptibility to various complications after burn injury,33,34,40,53 they are also risk factors for poorer in-hospital outcomes. 44
The limitations of this study must also be considered. While the registry currently collects data from all 17 designated burns units across Australia and New Zealand, it is possible that not all serious burn cases will be referred to a specialist burns unit. Consequently, there may be burn injuries that go uncaptured if they are managed in non-specialist unit. Consistent with this, previous reports estimate that > 9000 people in Australia and New Zealand are admitted to hospital for treatment of a burn injury each year and that the highest rates of death and hospitalisation occurred in the elderly.54–56 The BRANZ collects data from approximately one-third of these.7,57 Therefore, although population estimates were used in the calculation of ‘incidence’ data, care needs to be taken when considering these results. A recent study examining the epidemiological characteristics of burn-related fatalities in Australia and New Zealand found that 41% of fatalities between 2009 and 2015 occurred in a pre-hospital setting. 58 Patients who die at the scene or in transit to a specialist burn service are not captured by the BRANZ; therefore, the mortality rate reported in this study may also be lower than the actual mortality rate. In addition, although the WHO has stated that many high-income countries use the chronological age of 65 years as the lower limit of ‘elderly’ or ‘older person’, 14 these terms appear to have a loose, non-standard definition or cut-off based on arbitrary values. 59 Several studies challenge the use of only chronological age when considering older adults and instead suggest the use of either biological age (i.e. physiological or functional age, which considers other factors beyond chronological age) or a measure of frailty, especially when considering in-hospital and long-term outcomes after burn injury.60–64 The registry does not include a measure of, or collect data relating to, frailty at the current time and therefore cannot incorporate this into reporting or analyses. Finally, the number and type of patients taken to theatre for a significant dressing change (without skin grafting) may vary between specialist burn centres due to differences between the centres in dressing change practices. One potential difference between centres may be the ability to perform dressing changes under sedation on the ward. Centres where dressing changes cannot be performed on the ward may subsequently have to be undertaken in theatre.
These limitations aside, this is the first study to explore the epidemiology, causes, surgical intervention and in-hospital outcomes of older adult burn patients in Australian and New Zealand burns units. Increased awareness of the profile of older adult patients may mean burns units in these countries are more prepared to handle the projected number of older adults. This study also highlights several opportunities to implement prevention strategies and activities to reduce the burden of burn injuries in older adults. These data will be used to inform targeted burn awareness and prevention initiatives for different older adult age groups and high-risk scenarios such as scalds or burns within the home for the Australian and New Zealand adult older community. The need for burn centres to work collaboratively across interprofessional boundaries to have maximum effect cannot be understated. These data will be shared with key stakeholder groups with a vested interest and responsibility for the health and safety of older Australians and New Zealanders, and can be used to advocate for mandatory burn prevention and awareness training within the community aged care sector. Further research is required to explore the age-related differences in surgical interventions and if and how these differences are associated with in-hospital outcomes. Burn registries such as the BRANZ provide unique opportunities to study large populations to create new knowledge and science regarding burn care treatments and their effects on patient outcomes. This new knowledge will become richer when the BRANZ and other global burn registries begin to collect long-term outcomes.
Supplemental Material
OlderAdults_SuppMaterials_V5 – Supplemental material for Epidemiology of burn injury in older adults: An Australian and New Zealand perspective
Supplemental material, OlderAdults_SuppMaterials_V5 for Epidemiology of burn injury in older adults: An Australian and New Zealand perspective by Lincoln M Tracy, Yvonne Singer, Rebecca Schrale, Jennifer Gong, Anne Darton, Fiona Wood, Rochelle Kurmis, Dale Edgar, Heather Cleland and Belinda J Gabbe in Scars, Burns & Healing
Footnotes
Acknowledgements
The authors would like to thank the BRANZ Steering Committee for their support and provision of data for the project. Portions of this dataset were presented at the 43rd Annual Scientific Meeting of the ANZBA (Hobart, Tasmania, 15–18 October 2019).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The BRANZ has received funding from ANZBA, the Australian Commission on Safety and Quality in Health Care (2008–2009), the Julian Burton Burns Trust (2008–2013), the Helen Macpherson Smith Trust (2010–2012), the Thyne Reid Foundation (2011–2013), the Australasian Foundation for Plastic Surgery (2013–2017), the New Zealand Accident Compensation Corporation (2013–2020), the Clipsal by Schnieder Electric National Community Grants Program (2017), and the HCF Research Foundation (2018–2019). Individual burns units also contribute funding to the BRANZ to ensure its ongoing sustainability. Author BJG was supported by an Australian Research Council Future Fellowship (FT170100048) during the preparation of this manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.