
Abstract
Introduction:
Chemical burns are comparably rare but often result in full-thickness skin defects with frequent involvement of underlying structures. Hands are the most commonly affected injury site and impaired functional outcome is common. We present a case of an unusual chemical burn to the dorsum of the hand of a child secondary to application of a topical anti-wart treatment containing formic acid.
Case report:
An 11-year-old girl was referred to our outpatient department with a full-thickness injury resulting from a chemical burn having used a topical formic acid solution in the treatment of common warts. On examination, a 20-mm circular full-thickness defect was noted to the dorsum of the hand. The extensor tendons were not involved and there were no signs of infection. She required surgical debridement and local flap coverage. The postoperative recovery was unremarkable.
Conclusion:
Through a comprehensive literature review, four common topical solutions used in anti-wart treatment were identified to be associated with burns. Together with our case, this highlights the importance of careful patient education in the usage of common topical over-the-counter treatments.
Lay Abstract



Viral warts to the skins are common and are expected to heal by themselves with time. However, they can be associated with stigma and discomfort, leading many people to seek treatment for their removal. There are many different types of treatment options, the most common being to freeze them (cryotherapy) or using a solution that is painted on to the wart. Recently, there has been a rise in the number of different types of solutions that are used in the treatment of warts, including formic acid. Here we describe a case of an 11-year-old girl who used a formic acid-based solution to treat a wart on her hand. This resulted in a deep chemical burn that required surgery under local anaesthetic. She did not have any immediate complications from her surgery. On reviewing the literature, we identified two other acid-based solutions, salicylic acid and monochloroacetic acid, and a third chemical called other glutaraldehyde, that are commonly found in anti-wart treatments and have been described to cause chemical burns. These anti-wart treatments are widely available over the counter and we would like to highlight the importance of proper patient education when used to minimise the risk of chemical burns.
Background
Chemical burns account for approximately 3% 1 of patients within the burn population but can result in severe injuries associated with significant morbidity and mortality. The most commonly affected body parts in chemical burns are the upper extremities, most often the hands. Chemical burns on the hands and wrists are often deep and can result in temporary or permanent loss of function.2,3 Chemical burns occur most commonly in the working environment. Iatrogenic chemical burns have rarely been described but are usually associated with topical skin treatments.4,5
Cutaneous viral warts are common lesions, particularly in young people of whom an estimated 5%–30% are affected.6–8 They often resolve spontaneously; 9 however, the associated stigma and often unsightly appearance lead patients to seek treatments for their removal. There exists a wide array of anti-wart treatments available including cryotherapy, chemical destruction, laser therapy, electrosurgery and immunotherapy, often with little evidence for their use. 10 The most common treatments used are topical application of salicylic acid-based formulations and cryotherapy. 11
Topical formic acid-based solutions have been reported as effective, safe and inexpensive anti-wart treatments.12–14 The mechanism of action remains unknown but is hypothesised to act by dehydrating and destroying the infected tissue. 12 We report a case of a third-degree chemical burn in a child having used a formic acid-based solution for treatment of a cutaneous wart of the hand.
Case report
An 11-year-old patient was referred to our clinic for assessment of a full-thickness wound to the dorsum of her left hand. Eleven days previously she had used an over-the-counter topical solution containing formic acid to treat a common wart. She applied the solution once, limiting exposure to the confines of the affected tissue. The wound was subsequently covered with an occlusive dressing, although this was advised against on the pack insert. Two days after application, a necrosis had developed at the site. The patient attended her local primary care clinic where she was advised to dress the wound daily with aluminium acetotartrate-soaked gauze. Nine days after application she presented to the paediatric emergency department for a wound review. The attending doctor noted a dry necrosis and debrided the wound bedside under local anaesthesia. Two days after debridement she re-attended the emergency department due to increasing pain and was prescribed a course of oral antibiotics for a local wound infection. She was previously fit and well with topical eczema to her hands for which she occasionally used topical steroids. She was left-hand dominant.
Upon review, her main concern was pain from the wound limiting her ability to write. Examination of the dorsum of her left hand revealed a 20-mm diameter circular wound with a bed of granulation tissue, proximal to the first metacarpophalangeal joint (Figure 1). There were no signs of local or systemic infection. Given the size of the wound and the localisation directly over the thumb extensor tendons, the decision was made to surgically close the wound with a local flap.
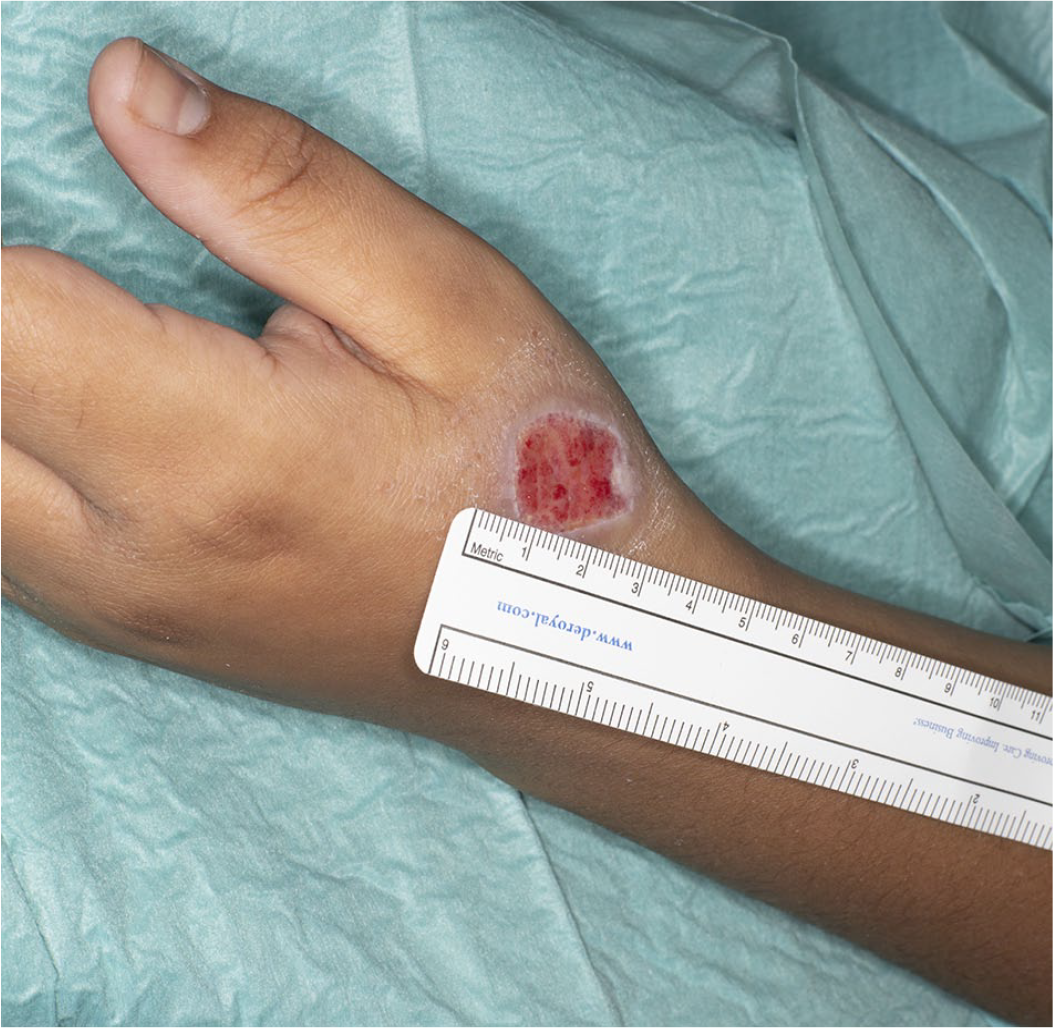
Preoperative image taken during the time of operation, 18 days after application of the ointment, revealing a 20-mm circular defect distal to the first metacarpophalangeal joint.
The wound was closed with a rhomboid flap under local anaesthesia 18 days after the initial application of the ointment (Figures 2 and 3). The postoperative period was uneventful and hand function was fully restored six weeks after surgery (Figure 4).

Intraoperative image of the defect and rhomboid flap design. The flap margin marked A was transposed to align with the wound margin marked a.

Image of the transposed rhomboid flap now covering the wound bed and sutured into place using single non-resorbable nylon sutures.

Postoperative image taken six weeks after surgery showing a well-healed rhomboid flap covering the entirety of the previous defect.
Discussion and conclusions
We describe a case of a full-thickness chemical burn following topical application of a solution containing formic acid on a common wart to the dorsum of the hand. Based on this case, a literature review was undertaken on burns associated with the use of formic acid. To the best of our knowledge, this is the first case of a full-thickness burn reported in a child.
A search of the literature was conducted on 1 October 2019 via PubMed® using the search terms ‘formic acid burn’ and ‘chemical burn wart treatment’. The article titles in the search results were screened for relevance. Only papers published in English describing iatrogenic burns as a result of chemical wart treatment were included. Reports of iatrogenic burns resulting from topical application of garlic—a household remedy frequently applied for the cure of skin conditions—were not included, since this topic has already been extensively reviewed.15,16 Burns secondary to cryotherapy were not included. Based on the aforementioned criteria, six articles were identified. Balagué et al. reported a case of third-degree burn on a digit in an adult using a solution containing formic acid continuously for 6 h in combination with an occlusive dressing. This healed spontaneously; however, a sensory deficit in the course of the underlying ulnar collateral nerve was noted. 17 Tong et al. reported a case of inappropriate use of anti-wart treatment containing formic acid in an adult resulting in a full-thickness injury over the little finger proximal interphalangeal joint (PIPJ) and secondary cellulitis requiring extensive debridement and reconstruction. In this case the injury resulted in significant functional impairment due to PIP and distal interphalangeal joint (DIPJ) stiffness. 18
When reviewing the literature, we identified further reports of other common anti-wart treatments whose use have been associated with chemical burns, including salicylic acid, 19 monochloroacetic acid4,20 and glutaraldehyde. 21 Table 1 details data from all reported cases, including patient characteristics, agent used, theorised reason for injury, resulting injury and outcome. All wounds subsequently healed with the majority requiring debridement and surgery. Functional and aesthetic impairments were common, including nail loss, scar hypertrophy and permanent malposition of joints. In most cases, patients used the treatments incorrectly, for example combing the ointment with an occlusive dressing or applying the treatment repeatedly in quick succession. In our own case, prolonged exposure to the ointment in combination with an occlusive dressing was the probable cause of injury.
Results from a literature review detailing the age and gender of the patients described in each identified journal article as well as localisation of injury, anti-wart agent used, assumed reason for injury, degree and extent of injury, treatment and outcome.
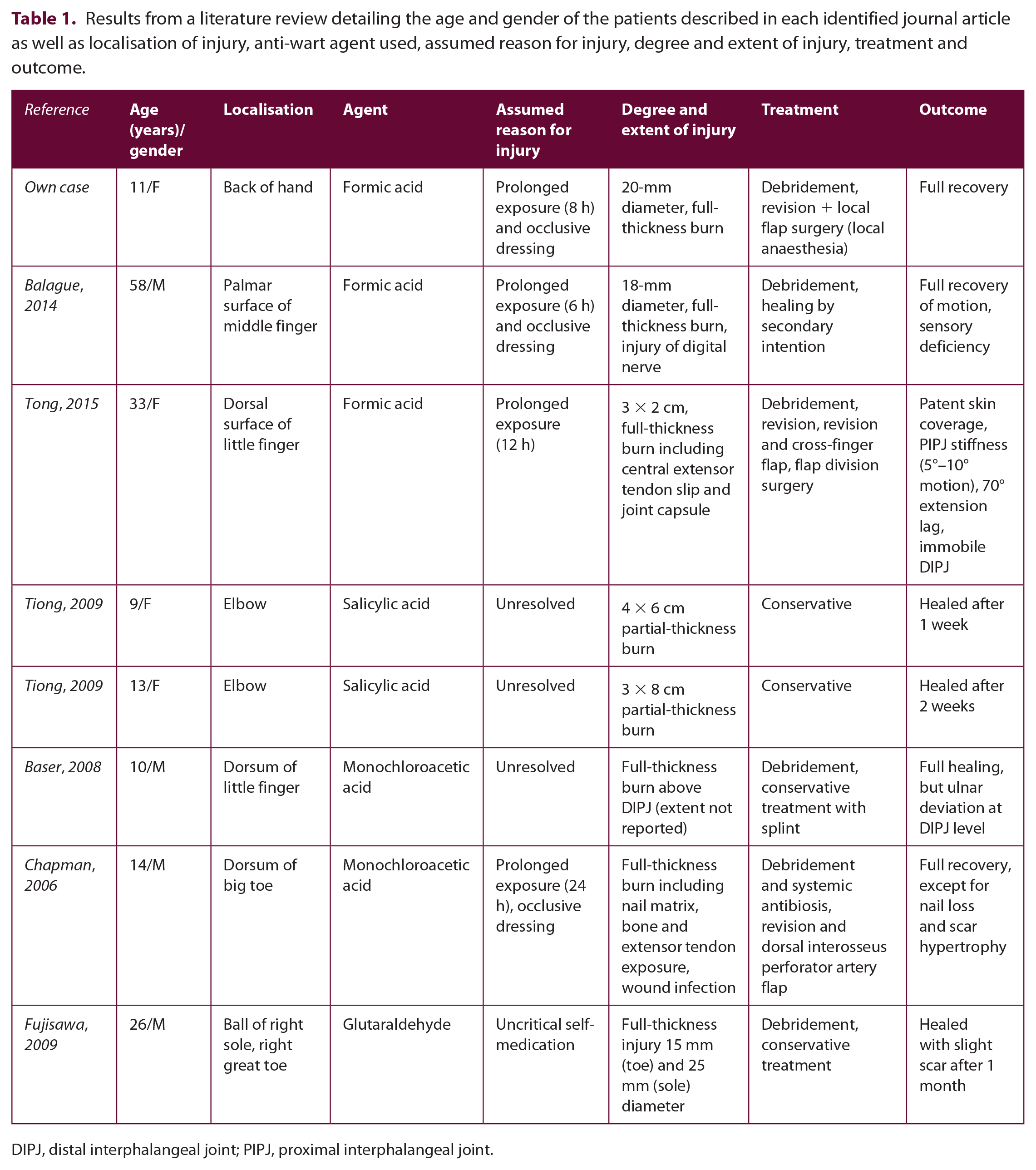
DIPJ, distal interphalangeal joint; PIPJ, proximal interphalangeal joint.
Given the popularity of self-diagnosis and self-medication, the instructions of proper use of over-the-counter medications need to be abundantly clear. This particularly applies to the self-treatment of common warts to limit severe but preventable complications such as full thickness wounds.
Footnotes
Acknowledgements
The authors give special thanks to the team of the Uppsala Burn Center outpatient department as well as to Mr. Tony Lif for shooting and providing the pictures of the described case.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Written informed consent for the case to be published (including accompanying images, case history and data) was obtained from the patient and legal guardian.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.