
Abstract
Aims
To describe clinical outcomes, management, and socio-economic impact of severe acute chemical eye injuries in a tertiary hospital.
Methods
37 patients required emergency admission to the Royal Victoria Infirmary eye ward between April 2013 and September 2015. Demographics, best corrected distance visual acuity (BCDVA), causative agent, degree of limbal stem cell deficiency (LSCD), management and socio-economic data were evaluated.
Results
Mean age on admission was 34.5 years (SD 16.3; range 16–82); 30 males (81.1%); 22 bilateral (59.5%). Causative agent: alkali in 30 cases (81.1%); acid in three cases (8.1%); and unknown in four cases (10.8%). Fifteen cases (40.5%) were assaults, 12 (32.5%) work-related accidents, nine (24.3%) domestic accidents and one (2.7%) undetermined. Eleven patients (29.7%) were unemployed, 18 (48.6%) were labourers, three (8.1%) were students, three (8.1%) were retired and two (5.4%) were professionals. Mean admission time was five days (SD 3.2; range 1–12). Mean follow-up time was 170.5 days (range 1–946). Mean cost of admission was £2478 (range £274–5785). Five patients (13%; seven eyes) developed total or partial limbal stem cell deficiency, all being assaults.
Conclusions
Main causative agent in our study was alkali, with young men in the working age being most frequently involved. Many patients required prolonged hospital admission and costly follow-up. The majority of cases were assaults, mostly occurring in unemployed patients. All the limbal stem cell deficiency cases were due to assaults. We believe that socio-economic factors play an important role in the cause, severity and cost of chemical eye injuries.
Lay Summary
Acute chemical eye injuries have a significant and extensive impact on patients’ visual function outcomes and vision-related quality of life, with consequent enormous burden to affected individuals, their families and society. We believe that by understanding the socio-economic environment, we may not only be able to enforce safety measures to tackle the increasing rate of severe chemical eye injuries in our community, but also to develop collaborative programmes with the community, educating the population on the seriousness of chemical eye injuries, and with the local authorities, trying to understand the clustering of assaults in areas and tackling the associated socio-economic risk factors, such as unemployment. Given the increasing rate of assaults using chemicals in recent times, it is also important to assess availability of adequate victim support programmes and develop good interaction with relevant local, regional and national authorities to ensure all aspects of community security service are in place to be able to address any potential deficiencies in line with police and home office guidelines. Keeping in mind that the best action plan is always prevention. However, when an ocular injury does occur it is evident that significant morbidity and visual sequelae can result and affect the socio-economic status of the victims despite our best current medical and surgical care.
Keywords
Introduction
Chemical eye injuries constitute a true ophthalmic emergency. 1 The type of chemical agent involved and duration of exposure will determine the severity of the damage to the eye, which can range from a mild disruption of the ocular surface to extensive involvement of the deeper structures of the eye. 2 Therefore, immediate therapy is directed toward prompt irrigation and removal of any remaining residues of the chemical agent that may still be in contact with the eye. 2
Mild injuries can be mostly treated as outpatient with topical medication and carry good visual prognosis. However, the most severe cases require emergency hospital admission for intensive topical, systemic and often surgical treatment (e.g., human amniotic membrane transplantation),2–4 which carries a poor long-term prognosis, with significant visual impairment that substantially impacts the quality of life of these patients.2,5 Due to the extensive damage that alkali agents may inflict to external and deep ocular structures of the eye, vision is frequently impaired, limiting the ability of these patients to perform their jobs and duties, and ultimately having a significant impact on their quality of life, with enormous implications at an age when they are able to economically contribute to society.2,5
The reported occurrence of chemical eye injuries as a proportion of all ocular traumas may vary significantly depending on the geographical area. In developing countries, unfortunately the reported incidences are not very precise, ranging from values as low as 1.4–4.8%, as reported by a hospital in India, 6 to higher incidences of 14.7%, as in the Guangdong province of China. 7 Strangely enough, in Europe the reported incidences are slightly higher, with values ranging between 7% and 18% depending on the studies.8,9 In the UK, the values are similar to other countries in western Europe, with a reported incidence of chemical injuries ranging between 7% and 10% among all ocular traumas.10–12 The limited access to medical facilities in developing countries may account for the higher percentage of unreported cases and the discrepancies in the incidences encountered between countries. We hypothesise that the socio-economic characteristics of the population in UK's northeast area may explain the higher incidence of severe chemical injuries to the eye. Thus, we conducted the present study.
The Ophthalmology Department at the Royal Victoria Infirmary in Newcastle-upon-Tyne, UK, serves a large residential and rural area with a population of approximately three million people. As a tertiary hospital of reference in the region, the eye emergency service receives a high volume of ocular injuries annually, including those related to chemical agents. Here we present a retrospective, consecutive, interventional case series of severe acute chemical eye burns that required emergency admission to hospital. The main aim of this study was to assess the demographics, causative agent involved, place where the injury occurred, type of injury and grading of severity, best-corrected visual acuity, hospital and medical management, clinical outcomes and rate of complications, such as limbal stem cell deficiency (LSCD). In addition, we collected data on health economics, including cost of hospital admission and treatment, and on the socio-economic background of the patients, and analysed whether there is any correlation between the socio-economic status and the high incidence of severe eye burns in our community.
Materials and methods
The study was conducted following the principles of the Declaration of Helsinki for studies including human subjects and was approved by the local clinical governance and audit committees (Newcastle upon Tyne Hospitals Foundation Trust). We conducted a retrospective review of medical notes from all consecutive acute cases examined at the Eye Emergency Department (EED) of the Royal Victoria Infirmary (RVI) and that were diagnosed with severe chemical eye injuries and admitted as an emergency to the RVI eye ward between April 2013 and September 2015. During the period of study, a total of 37 patients (59 eyes) were identified from the hospital admission database with a diagnosis of severe chemical eye injury (Figure 1). The duty doctor at the EED initially assessed all the cases and initiated the emergency treatment accordingly. The degree and extent of tissue damage is a prognostic indicator of recovery of the ocular surface after chemical injuries. The Roper-Hall (R-H) classification provides a valuable mean to grade chemical eye injuries based on the corneal appearance and the extent of limbal ischaemia. 13 However, the Dua's grading system also takes into consideration the conjunctival involvement, providing a more precise classification that allows for a more accurate prediction of clinical outcomes.14–16 Thus, all patients were initially graded in EED on admission by using the Dua's grading system for chemical eye injuries. 14 Subsequently, a single specialist corneal consultant reassessed the case, including re-grading its severity within the initial 24 hours after admission if necessary. Data was collected on demographics (age, gender, affected eye), best-corrected distance visual acuity (BCDVA), chemical agent and type of injury, management, and incidence of complications, such as increased intraocular pressure and LSCD, among others. In addition, information on the time and cost of admission (including hospital expenses and cost of topical, systemic, and surgical treatments), and the socio-economic background (including professional status, and post code address at the time of injury) was collected and analysed accordingly to determine any association between severity of chemical injury and patient's professional and economical status.

Colour photographs of two of our severe patients: one during the acute phase (A & B), and the other one at a later time point (C). The image in (A) shows severe corneal oedema with folds (*), and subtotal limbal ischaemia (arrows), while the image in (B) demonstrates the complete absence of epithelium when fluorescein drops are instilled. The image in (C) shows corneal neovascularization in all four quadrants (arrows), and a persistent epithelial defect with opacification of the central cornea (*). Both patients developed secondary total limbal stem cell deficiency (LSCD).
Statistical analysis
Statistical analyses of the data were performed using Microsoft Excel for Mac 2011 (version 14.4.2, 2010; Microsoft Corporation) and GraphPad Prism for Mac OS X (version 5.0c, 1994–2010; GraphPad Software, Inc.). ANOVA tests were performed to compare between groups. Bonferroni's multiple comparison tests or Kruskal-Wallis non-parametric tests were used where appropriate. Values are shown as mean ± standard deviation (SD), unless stated otherwise. A level of p < 0.05 was accepted as being statistically significant.
Results
Demographics
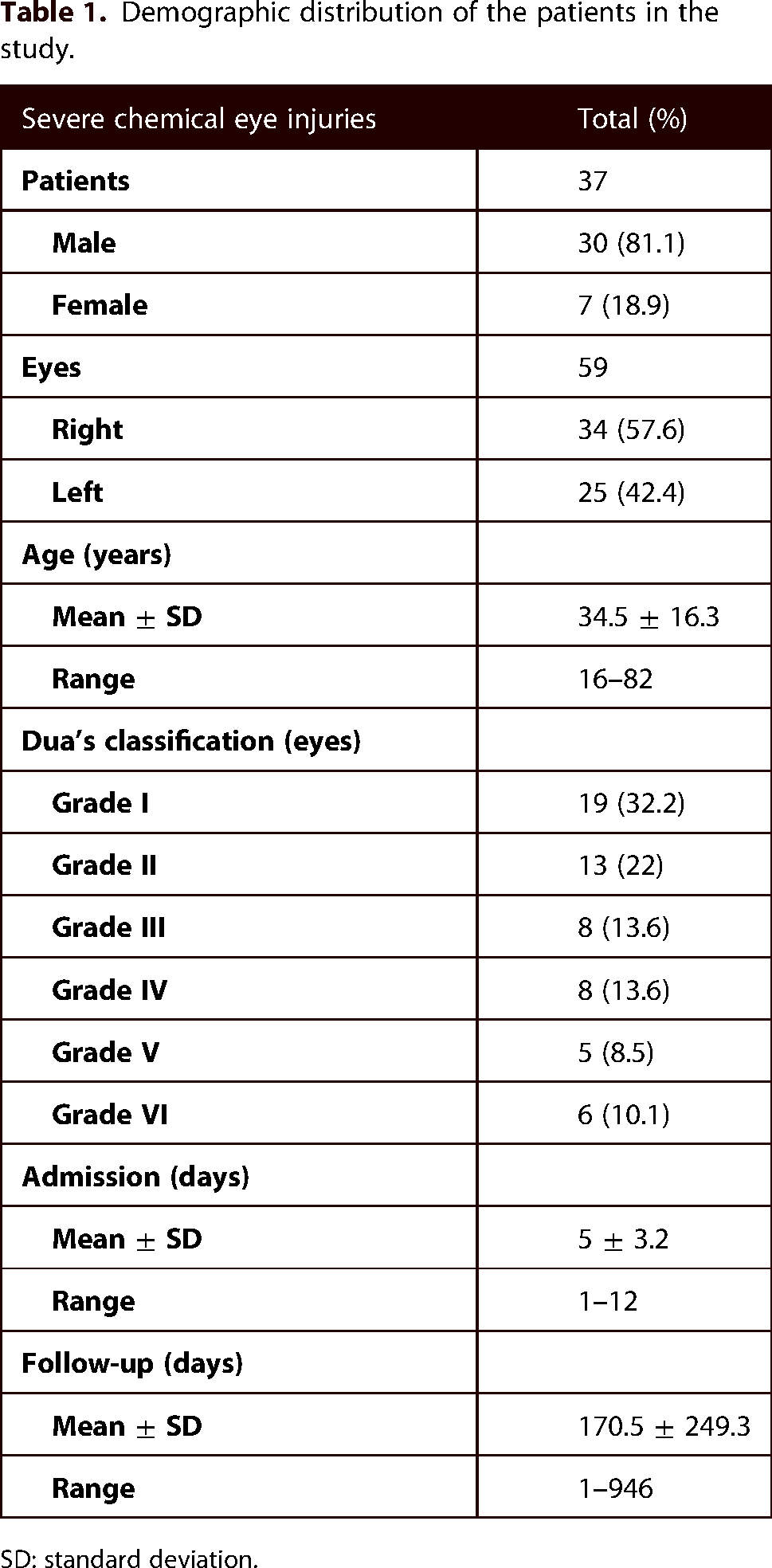
During the period of study, a total of 37 patients (59 eyes; 34 OD/25 OS), of which 30 were male (81.1%) and seven female (18.9%), required emergency admission to the eye ward at the Royal Victoria Infirmary (RVI) for management of severe acute chemical eye injuries (Table 1). The mean age on admission was 34.5 years (SD 16.3; median 29; range 16–82). Twenty-two patients (59.5%) presented with bilateral involvement, while in 12 cases (32.4%) only the right eye was affected, and the remaining three patients (8.1%) presented with only the left eye affected. The causative agent was alkaline in 30 cases (81.1%), acid in three cases (8.1%), and unknown in four cases (10.8%) (Figure 2A). The type of injury included 15 cases (40.5%) that suffered an assault, 12 (32.5%) were work-related accidents, nine (24.3%) were domestic accidents, and one (2.7%) was undetermined (Figure 2B). Of the 22 patients that presented with bilateral injuries, 13 cases (59.1%) were assaults, four (18.2%) were work-related, four (18.2%) were domestic accidents, and one (4.5%) was unknown, all with different degrees of severity in either eye.

Distribution of the cases in our study A) per causative agent, and B) per type of injury.
Demographic distribution of the patients in the study.
SD: standard deviation.
Grading of severity and visual acuity
The original Dua's grading on admission at the EED was as follows: grade I, 19 eyes (32.2%); grade II, 13 eyes (22%); grade III, eight eyes (13.6%); grade IV, eight eyes (13.6%); grade V, five eyes (8.5%); grade VI, six eyes (10.2%). In the grade I and grade II groups (32 eyes), 10 eyes (16.9%) were the fellow of a more severely affected other eye (grade III-VI), while the remaining 22 eyes were either a unilateral grade I or II (six eyes), or a combination of both bilaterally (16 eyes). When we analysed the distribution of the Dua's grading of the eyes per type of injury, the differences were not statistically significant between the groups (p > 0.05; Figure 3).

Distribution of the severity of the chemical injuries based on the Dua's grading system per type of injury. [Data are means + /-SD; p > 0.05].
The overall mean best-corrected distance visual acuity (BCDVA) in LogMAR on admission was 0.58 (SD 0.66) (Figure 4A). Moreover, when we analysed the results per type of injury, the assault group presented the worst BCDVA initially (0.85, SD 0.81), and remained the worst group at the last follow-up (0.61, SD 0.96) (Figure 4A), whilst the other three groups (i.e., work-related accidents, domestic accidents, unknown) regained a mean final BCDVA of 0.1 LogMAR at the last follow-up (mean 170.5 days; SD 249.3). These differences were not statistically significant (p > 0.05). However, when we analysed the data from the grade III and grade IV eyes only, the differences became statistically significant, with the assault group also presenting the worst results (1.03, SD 1.14; p = 0.017) (Figure 4B).

Best-corrected visual acuity (BCVA) per type of injury including (A) all eyes in the study, and (B) only the severely damaged (grades III-VI). Note that the assault group presented with the worst visual outcomes at any time point; differences between groups were only significant in (B) (p = 0.017). The graph in (C) represents the BCDVA of the 7 patients (9 eyes) that developed severe LSCD. In addition, it shows the results in BCDVA of partial and total LSCD separately. [The dotted lines in B and C represent the average values for all the patients graded as III-VI. Data are means + /-SD].
Hospital management and limbal stem cell deficiency
All patients, irrespective of initial severity grading, received the same high frequency topical and systemic treatment on admission, as per our emergency department chemical injury protocol: hourly g. prednisolone acetate 1%, hourly g. sodium citrate 6.5%, 2-hly g. ascorbic acid 10%, g. chloramphenicol 0.5% 4 times/day, doxycycline 100 mg tablets once/day, vitamin “C” 1 g tablets once/day (all eye drops were preservative free). Ten severe burn patients (27%; 12 eyes; eight assaults, two work-related) underwent additional amniotic membrane transplantation (AMT) within admission (mean time 4.3 days; SD 0.98; range 2–5) as part of the emergency management protocol for severe chemical eye injury, while one patient (2.7%; one eye; domestic) received it at 26 days. The latter had been initially treated at a different hospital. Despite this intensive treatment, seven patients (18.9%; nine eyes; all assault with ammonia) developed total (five eyes) or advanced partial (four eyes) LSCD. As expected, the BCDVA in the subgroup of patients with total LSCD remained very low at the last follow-up (mean 2; SD 0.71; range 1–3; in LogMAR), since these patients developed severe corneal neovascularisation and opacification involving the visual axis as part of their severe LSCD clinical manifestation. On the contrary, the patients with advanced partial LSCD achieved better BCDVA than those with total LSCD (mean 0.8; SD 0.82; range 0.18–2; in LogMAR). However, the differences were not statistically significant (Figure 4C).
Socio-economic data
Mean hospital duration of admission was five days (SD 3.2; median 4; range 1–12), and the mean cost was £2478 (SD £1496.9; median £2125; range £274 - £5785) per patient. The expenses were fully covered by the National Health Service (NHS). This data includes the cost of the hospital bed, as well as the cost of the systemic, topical and surgical treatments. Mean follow-up time was 170.5 days (SD 249.3; median 50; range 1–946). Twelve patients (32.4%) were lost to follow-up, nine patients (24.3%) are still under review in the corneal clinic as outpatients, and 16 patients (43.3%; 24 eyes) were discharged from clinic after fully recovering from their original injuries (Table 2). The latter were either mild chemical injuries that had been initially overestimated in severity by the emergency eye doctor (10 patients; 15 eyes), severe cases that responded well to intensive treatment (four patients; five eyes), or a combination of both mild and severe injuries that also responded well to treatment (two patients; four eyes). If we take into consideration the 15 mild cases only, the mean admission time was 1.9 days (SD 1; median 2; range 1–4), the mean follow-up time was 31.4 days (SD 40.5; median 23; range 1–160) and the mean admission cost was £984 (SD £601.9; median £675; range £274 - £1747), which are much lower values than the total values for the entire cohort due to the shorter duration of admission.
Rate of limbal stem cell deficiency distributed by post-admission review status for all the patients in our study.

*At last control; LSCD: limbal stem cell deficiency; F/U: follow-up.
We also collected data on the professional status of the patients at the time of their injury. Eighteen patients (48.6%) were labourers (10 work-related, three domestic, four assaults, one unknown), 11 (29.7%) were unemployed (10 assaults, one domestic), three (8.1%) were students (one work-related, two domestic), three (8.1%) had retired from work (two domestic, one assault), and two (5.4%) were professionals (one work-related, one domestic) (Figure 5A). As expected, the group of labourers mainly presented with injuries that happened at the site of work. However, in the unemployed group, the number of assaults was interestingly higher. Although the differences were not statistically significant between the groups (p > 0.05), the higher number of assaults in the unemployment group suggests an association between this type of injuries and the socio-economic status.

A) Distribution of eyes per type of injury and professional status. Note that in the labourer group, the majority of injuries were work-related, while the unemployed patients suffered more assaults. B) Postcode map distribution of all the patients in the study. Note that most of the assaults live in areas that are geographically close, which suggests a relation between socio-economic status and severity of the ocular injury [Royal Victoria Infirmary – NE1]. C) “Small area average weekly household income” (£) distribution per type of injury. The patients in the assault group presented statistically significant lower average income (p < 0.05) when compared to the overall cohort and the other three groups (Data are means + /-SD).
To investigate this further, we collected the home postcode for every patient at the time of injury as recorded in the hospital database and analysed it accordingly (Figure 5B). The results demonstrated that the majority of the patients who suffered an assault were living around the same geographical area (red triangles on the map). Moreover, we also collected the ‘total average weekly household income’ for every patient, based on the postcode and the estimations by the Office for National Statistics (2007-2008). 17 The overall average income in our study was £530.8 (SD 161.5; median £500; range £0 - £960) per week. When analysed separately per type of injury, the mean results were as follows: assault, £441.3 (SD 134.7; median 460; range £0 - £640); work-related accident, £606.7 (SD 174.0; median £585; range £400 - £960); domestic accident, £576.7 (SD 133.9; median £510; range £480 - £820); unknown, £550 (Figure 5C). The statistical analysis demonstrated statistically significant differences in terms of weekly household income between the assault group and the overall cohort (p = 0.0427), as well as with the work-related accident group (p = 0.0214), and the domestic accident group (p = 0.0059). The unknown group included one patient only, and statistical analyses could not be performed.
Discussion
Chemical burns to the eye constitute a serious form of injury with potentially catastrophic long-term consequences to patients, including poor vision, often associated with ocular surface discomfort, and overall poor quality of life.2,5 The reported incidences of chemical eye injuries vary depending on the geographical area.6–9 The limited access to medical facilities in developing countries may explain the higher percentage of unreported cases and the discrepancies in the incidences encountered. 6 In the UK, the values are similar to the latter, with a reported incidence of chemical injuries ranging between 7% and 10% among all ocular traumas.10–12 In a recent study, the authors reported an annual incidence of chemical eye injuries from the northeastern area in the UK of 5.6 new cases per 100,000 population. 18 This is a significantly higher value than the previously estimated annual incidence in the UK (0.02 per 100,000 population). 19
In chemical eye injuries the type of causative agent involved and the time of exposure will determine the severity of the damage to the eye initially, which can range from a mild disruption of the ocular surface to extensive involvement of the deeper structures, including iris, lens, ciliary body and retina. 2 The extent of damage to those structures is a prognostic indicator of potential recovery of the ocular surface, and will determine the final visual outcome. Due to the extensive damage that alkali agents normally inflict to both external and deep structures of the eye, vision is frequently impaired, limiting the ability of these patients to perform their jobs and duties, and ultimately impacting their quality of life and ability to work, therefore with enormous impact to their family and society.2,5
Several classifications of chemical injuries have been proposed in the past. Currently, the two most commonly used are the well-established Roper-Hall and the more comprehensive Dua classifications.13,14 The Roper-Hall (R-H) grading system provides a valuable mean to classify all chemical eye injuries based on the corneal involvement and the extent of limbal ischaemia. 13 However, Dua's grading system, in addition to cornea and limbal damage, also takes into consideration the surrounding conjunctival involvement, providing a more precise classification that allows for a more accurate prediction of clinical outcomes.14–16 In our institution, the Eye Emergency Department guidelines include the Dua classification 14 as a mean to grade acute chemical eye injuries. Since the eye emergency doctor performs the initial examination of the patient before presenting the case to the consultant on call (not always a cornea specialist), there is a need for a simple, user friendly and easy-to-use grading system of screening between those cases that are mild and can be treated topically in the outpatient department, and the more severe cases that will require real emergency treatment and subsequent hospital admission for intensive care therapy. After admission and within the first 24 hours, a corneal specialist consultant re-assesses the patient and re-grades the ocular injury accordingly. The discrepancy between the initial grading done by the EED doctor and the one performed by the corneal consultant, with the first one grading some of the milder cases as severe, suggests that it is necessary to review and strengthen the training programme of junior doctors in EED to avoid erroneous and unnecessary admissions to the hospital. This would reduce the overall costs of treatment and spare patients the emotional stress.
Previous studies have demonstrated that severe chemical eye injuries are more common in men of working age, occurring accidentally at work or at home, with ammonia being the main causative agent.2,3,11,20 In our current study, severe chemical eye injuries were also seen more commonly in young men, mainly of working age, with alkali as the main causative agent. However, the main cause of injury was an assault (41%), closely followed by accidents at work (32%). This marks a different trend when compared with previous studies. In a recent study in the UK, Macdonald et al. 19 reported that chemical eye injuries occurred more frequently at the place of work (50%), followed by assaults (33.3%). Similarly, Le et al. 21 and Hong et al. 22 reported incidences of work-related accidents in China of 87.5% and 74.8% respectively. This high incidence of injury at work reflects a serious health and safety problem not encountered in our study. The different trend in our study may be explained by several factors. First, most of the patients in the assault group were unemployed at the time of injury and consequently the average weekly household income in the assault group was significantly lower when compared to the other groups; and secondly, most of the patients in the assault group were living in nearby areas at the time of injury. This data seems to indicate that the socio-economic status may play a significant role in the type and severity of the damage in chemical eye injuries, with severe chemical injuries after an assault happening more frequently in unemployed patients who reside in areas with lower household income, suggesting that the victims may share the same socio-economic status with their attackers. Haring et al. 1 observed a similar trend in a recent multicentre study from the USA. In their study, they demonstrated that chemical eye burns occur more frequently in individuals in the lower annual household income quartiles. This common trend with our study indicates a strong relationship between the socio-economic status of the patients and the type of severe chemical eye injury, suggesting that patients with lower income are at a higher risk of getting involved in activities that may lead to suffering a chemical eye injury, most commonly as an assault.
Early management, including immediate eyewash followed by topical and systemic intensive treatment may be the single most important outcome-influencing factor in chemical eye burns. 23 The goal is to wash out the causative chemical agent immediately and to reduce the intense inflammatory reaction, preserving the globe integrity by protecting the ocular surface, promoting corneal regeneration, and inducing keratocyte proliferation and collagen production.2,19 After the initial emergency treatment and within the first three to five days a decision has been made regarding subsequent management – mainly surgical treatment, including early use of human amniotic membrane (HAM) as a biological dressing 16 aiming to reduce ocular surface inflammation and maximising healing. Unfortunately, despite the best management, severe chemical burns (RH grade IV and Dua grades IV-VI) almost invariably lead to severe and total LSCD16,24 often associated with blindness due to corneal scar and vascularisation involving the visual axis. There is also a danger of associated complications, such as lid malposition, glaucoma, cataract formation and retinal damage.2,19 Saini and Sharma 20 demonstrated that chemical eye injuries caused by assault tend to be more severe, with a higher proportion leading to LSCD and consequent severe visual impairment accompanied by chronic ocular surface discomfort or pain despite intensive treatment. Our data correlates well with their study, since all the LSCD cases were assaults, and occurred despite early admission and intensive topical and surgical intervention. The final lower BCDVA in this subgroup of patients was secondary to LSCD, due to severe corneal neovascularisation and scar formation that encroached on the visual axis. At the time of reporting, all the LSCD patients were unilateral and were awaiting autologous ex vivo cultivated limbal epithelial stem cell transplantation (auto-CLET) to restore the ocular surface integrity.24,25 If the ocular surface cannot be successfully restored with auto-CLET, other more aggressive surgical treatment options can be offered, such as a keratoprosthesis, which can also restore the visual function. 26 However, these devices are not exempt from complications and require lifetime treatment and close follow-up.
The mean cost of emergency hospital treatment (topical, systemic, and surgical treatments) was rather significant in our study (£2478; SD £1496.9). This is lower than a recent study by Le et al. from China in which the mean cost of medical treatment was £4725 (range £472–53,171). 21 In Le's study, almost 52% of the victims paid all medical expenses, or the majority of expenses, by themselves, significantly affecting their household income. This is not the case for the patients in our study, since the expenses were fully covered by the National Health Service (NHS) which is free at the point of use throughout the UK. However, the majority of patients with the most severe injuries, including those with bilateral involvement, came from low-income areas and were unemployed at the time of injury, which limited significantly their ability to apply for jobs in the future and consequently support their families and contribute to society. Similarly, Le et al. 21 demonstrated that severe chemical injuries carry a huge impact on the victims’ personal and household income, since most of the individuals in their study lost their jobs or were obliged to change them after the injury due to visual impairment and consequent loss of working ability. Moreover, Haring et al. 1 have recently reported that in the United States, chemical eye burns comprise almost 36,000 visits to the emergency department (ED) and $26.6 million in ED-associated charges every year. However, the true effect of severe chemical injuries, including loss of workdays of the patients and their family members, loss of productivity, administrative costs, and the significant costs of continued medical care of sequelae are likely to be much greater than estimated.
Finally, we would like to comment on the potential danger to society of a ‘terror attack’ using chemicals both acid and alkali (“acid attacks”). Media coverage on recent unfortunate episodes has increased the awareness of the people on the problem of chemical injuries. As terrorist attacks have been very effective by air and land, what if they mimic the enormous damage to potentially a significant number of people at the same time in a public place by spraying corrosives? According to recent reports from 37 UK police forces, assaults involving corrosive substances have more than doubled in England over the last five years (183 in 2012, 238 in 2013, 285 in 2014, 460 in 2015 and 504 in 2016). 27 Therefore, it is crucial that doctors all over the world improve their knowledge in treating these severe acute conditions at the urgent stage, in order to minimise the serious impact to patients’ quality of life. At the same time, collaborative programmes should be promoted within the community and in the media, in order to educate the population on the importance of using preventive measures at the workplace and at home to protect themselves from suffering chemical eye injuries. 27 Interestingly, the assaults in our study had the eyes as the only targeted area in the body. This may be different from the recent “acid attacks” in London where the chemical used, as well as the motivation of the assault, may be different since the targeted area was not specifically the eye. 27
In conclusion, acute chemical eye injuries have a significant and extensive impact on patients’ visual function outcomes and vision-related quality of life, with consequent enormous burden to affected individuals, their families and society. We believe that by understanding the socio-economic environment, we may not only be able to enforce safety measures to tackle the increasing rate of severe chemical injuries in our community, but also to develop collaborative programmes with the community, educating the population on the seriousness of chemical eye injuries, and with the local authorities, trying to understand the clustering of assaults in poorer areas and tackling the associated socio-economic risk factors, such as unemployment. In addition, it is necessary to educate admitting junior ophthalmology doctors in EED to avoid unnecessary admission to hospital of milder chemical injuries that would reduce the overall costs and spare emotional stress to patients. Given the increasing rate of assaults using chemicals in our community, it is also important to assess availability of adequate victim support programmes and develop good interaction with relevant local and national authorities to ensure all aspects of community security service are in place to be able to address any potential deficiencies in line with police and home office guidelines. Keeping in mind that the best action plan is always prevention. However, when an ocular injury does occur it is evident that significant morbidity and visual sequelae can result and affect the socio-economic status of the victims despite our best current medical and surgical care.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
How to cite this article
Salvador-Culla B, Hogg J, Okonkwo A, Mulroy J, Figueiredo GS and Figueiredo FC. Severe chemical eye injuries – clinical outcomes and associated socio-economic factors. Scars, Burns & Healing, Volume 9, 2023. DOI: 10.1177/20595131231180367