
Abstract
Introduction
Chemical burns, particularly injuries related to psychiatric illnesses, are underreported in the literature. We present two cases of self-inflicted alkali chemical burns managed conservatively. Frequent clinical review of the burn was aimed to ensure appropriate healing and compliance with the treatment plan based on regular dressing changes.
Case 1
A 24-year-old woman presented during the first day of the initial injury with a minor self-inflicted chemical burn to the right forearm. The causative agent was an oven cleaner containing sodium hydroxide triggering an alkali-based burn. The surface area of the injury was 0.5% total body surface area (TBSA) full-thickness burn. The patient had a complex psychiatric history diagnosed with personality disorder, anxiety and depression.
Case 2
A 55-year-old woman presented with a self-inflicted left forearm full-thickness burn (0.5% TBSA). This was five days after the initial injury from an oven cleaner containing sodium hydroxide. The patient had a psychiatric history of anxiety and depressive disorder.
The mainstay of burn management was conservative with regular dressing changes and a topical agent. Telemedicine via a designated email address was given to the patient for virtual clinical burn review and any urgent issues. Photograph of the initial burn was taken, and clinic visits were scheduled to determine healing progress.
Conclusion
Self-inflicted chemical burns are to be managed within a multidisciplinary setting including early psychiatric involvement. We advocate a holistic approach to determine conservative or operative management, taking into account patient factors, burn complexity and clinician's judgement to streamline the treatment plan.
Lay Summary
Chemical burns due to self-harm are rare to see in clinical practice. A review of two cases secondary to intentional burns sustained using an oven cleaning material. Patients had psychiatric issues and were on medications to control symptoms. Close observation with regular dressings and topical cream would allow burns to heal without the need for an operation. Our recommendation would be to treat these burns with dressings and regular follow up in the clinic or virtually till healed.
Keywords
Background
Chemical burns account for 3% of all burn injuries and are typically caused by unintentional exposure to a hazardous substance either industrial or domestic. 1 The group of self-inflicted burns tend to occur in patients with previous psychiatric diagnoses. 2 One of the key factors to initiate appropriate treatment is to identify causative chemical agent either alkali or acid based. In general, the management of burns is conservative or surgical depending on the depth of injury. 1 The pathway of self-inflicted chemical burns may vary pending a multidisciplinary team approach and patient factors. 2 We highlight two cases of self-inflicted full- thickness chemical burn managed conservatively in a tertiary burns unit.
Case 1
A 24-year-old woman presented with a minor self-inflicted chemical burn to the right forearm within one day of the initial injury. The causative agent was an oven cleaner containing sodium hydroxide triggering an alkali-based chemical burn. The total body surface area (TBSA) was 0.5% full-thickness burn eschar to the proximal dorsal aspect of the right dominant forearm (Figure 1).

Case 1: left forearm chemical burn (alkali) – day 1 after injury.
The patient had a background of complex psychiatric issues associated with a personality disorder, anxiety and depression. She was admitted to our unit few times previously with other self-inflicted burn injuries. On this occasion, the psychiatric team reviewed the patient and adjusted her medication as part of a holistic treatment plan.
The mainstay of burn management was conservative with the use of Flamazine™ (silver sulfadiazine) daily for three weeks until the full-thickness burn eschar was lifted off the wound (Figure 2). Telemedicine and weekly reviews in the clinic were used to monitor healing. Once the eschar was lifted, a soft foam dressing (Mepilex® XT) was applied to allow further healing and fewer dressing changes (Figure 3). The burn fully healed 12 weeks after the initial injury without any functional deficit. The delay in healing was due to secondary insults to the original burn wound inflicted by the patient. This was detected on the ninth week, and the dressing was protected with an additional bandage till the burn healed (Figure 4).

(a) Case 1: eschar noted three weeks after burn injury. (b) Mechanical removal of eschar and underlying wound.

Case 1: progressive healing at nine weeks after burn with regular dressings.

Case 1: fully healed burn 12 weeks after injury.
Case 2
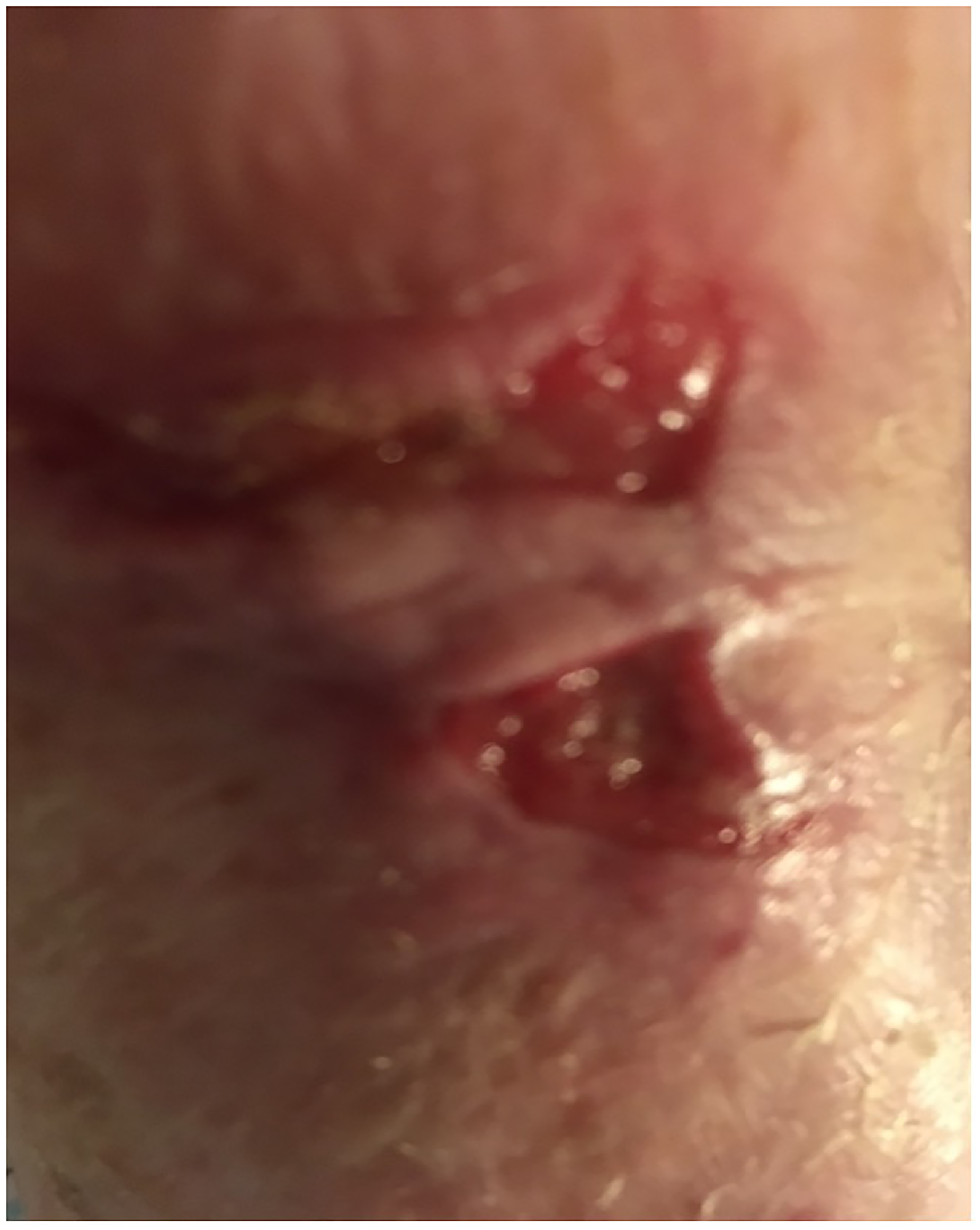
A 55-year-old woman had a self-inflicted injury to the left (non-dominant) forearm and presented five days after the incident. A full-thickness burn (0.5% TBSA) was sustained from an oven cleaner based on sodium hydroxide (Figure 5). The patient had a psychiatric history of anxiety and depressive disorder. She had previous hospital admissions due to repetitive deliberate self-harm injuries.

Case 2: left forearm chemical burn (alkali) – day 5 after injury.
Similar to the first case, the burn was managed conservatively. The slightly sloughy nature of the burn wound dictated the need to use a Flaminal® topical agent with a dressing change every two days. This was changed to MEDIHONEY® HCS (Hydrogel Colloidal Sheet dressing) for the following two weeks to soften the eschar, which helped to lift it off the burn bed (Figure 6). UrgoTul™ dressing was used in the fifth week until the wound was completely healed in the ninth week after injury (Figure 7).
Case 2: left forearm burn healing at five weeks after dressing management.

Case 2: left forearm burn healed at nine weeks after injury.
The decision for conservative management was based on the senior clinician's judgement and a multidisciplinary team discussion. This stems from prior experience of ongoing deliberate self-harm on the operated site. Spilt thickness skin graft (STSG) for burn wound based on similar cases. Both patients were scheduled for regular weekly follow-ups in the burns clinic to monitor healing. The patients regularly sent photographs at least once a week via a designated telemedicine email address to encourage self-monitoring of burn healing and offer advice remotely.
Discussion
Chemical burns, particularly self-inflicted injuries, are underreported in the literature. There are only five case reports of various chemical agents and associated psychiatric conditions with various burn depth and treatment options (Table 1). Park et al. presented three cases of self-inflicted chemical burns with a diagnosis of delusional parasitosis. Two of these cases had TBSA >4.5% and were treated with STSG, whereas one case had TBSA 0.4% and was managed conservatively. 3 Another case with hydrocarbon enema to the perineum and buttocks was described by Mygatt et al. and had 6% TBSA partial-thickness burns treated conservatively. 4 Idicula et al. described a case of factious disorder with a history of frequent self-inflicted burns while at work from an unknown chemical agent. This patient was previously treated with a STSG, which failed and was subsequently managed conservatively with dressings. 5 Fino et al. reported a case of self-inflicted 0.5% TBSA full-thickness chemical burn from acoustic substance. This was managed conservatively, and healing was achieved six weeks after injury. 6 Katia et al. reported two cases of intentional chemical burns. The first case involved a 74-year-old man who had 3% TBSA burns on the lower limb with two full-thickness areas. Initially, burns were treated conservatively, followed by a STSG. The second case was for a patient with anorexia nervosa and self-induced vomiting who developed a full-thickness wound treated conservatively. 7
Self-inflicted chemical burns reported cases in the literature.

SSG, split skin graft.
The majority of self-inflicted chemical burns (<1% TBSA) were successfully managed with conservative measures and surgical intervention was considered for larger surface area. According to NICE guidance recommendations, self-harm injuries should be treated with the same care as unintentional injuries. However, further treatment should be based solely on a holistic psychiatric, psychological and social evaluation, including a risk assessment for future intentional self-harm episodes. 8 Despite the fact that NICE recommendations did not specifically include self-inflicted burns management, it has been recommended that superficial wounds <5 cm in size should be managed initially with adhesive dressing until more complex injuries are addressed. 8 A national audit to determine the adherence to guidelines concerning self-inflicted burns concluded that most patients received conservative treatment rather than surgery compared with similar unintentional injuries. This was attributed to a deficiency in the knowledge with NICE guidelines recommendations among healthcare professionals. 9 Contrary to this opinion, patient factors such as co-morbidities, healing potential and burns wound attributes should influence the decision making in the management of such injuries. This would take precedence over clinician's attitude toward the mechanism of injury and patient's mental health status. A thorough psychiatric evaluation alongside the patient's medical fitness assessment is essential. 10
Conclusion
Self-inflicted chemical burns are to be managed within a multidisciplinary setting including early psychiatric involvement. We advocate a holistic approach to determine conservative or operative management, taking into account patient factors, burn complexity and clinician's judgement to streamline the treatment plan for these burns.
Footnotes
Acknowledgments
The authors thank Semanti Chakraborty, Librarian at University Hospitals Birmingham, for her help with the literature search.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
How to cite this article
Galo A, Farid M and Almasharqah R. The conservative management of self-inflicted chemical burns: Case report and literature review. Scars, Burns & Healing, Volume 37, 2021. DOI: 10.1177/20595131211080545.