
Abstract
Background:
Acinetobacter baumannii is one of the most important agents of hospital infections. Rapid and accurate identification and genotyping of A. baumannii is very important, especially in burn hospitals in order to prevent the spread of related nosocomial infections and to further epidemiological studies.
Material and methods:
For two months, 82 A. baumannii isolates were collected from burn wound swabs of patients in a major burn hospital in Tehran. A. baumannii isolates were identified by conventional microbiological test and polymerase chain reaction (PCR) using the primers of blaOXA-51 gene, while the genetic linkage of A. baumannii isolates was investigated by enterobacterial repetitive intragenic consensus (ERIC)-PCR technique. Similarity, a cut-off of ⩾ 95% was considered for classifying the genotypes.
Results:
The molecular test (PCR) confirmed 97.56% of phenotypic results for the detection of A. baumannii isolates. ERIC-PCR results revealed 14 different ERIC patterns (ERIC-types) including 11 common types and three unique types.
Conclusion:
Our findings show that we can simply and quickly detect A. baumannii isolates by PCR using blaOXA genes and genetic diversity by ERIC-PCR, respectively. These rapid and simple techniques for the routine screening and identification of clinical A. baumannii isolates could be useful with epidemic potential.
Background
The history of the recognition of the genus Acinetobacter dates back to the early 20th century. 1 Today, the genus Acinetobacter contains Gram-negative coccobacilli which are aerobic, non-fermentative, non-motile, catalase positive, oxidase negative and with a G + C content of 39–47%.1,2 Four species of Acinetobacter including A. calcoaceticus, A. baumannii, A. pittii and A. nosocomialis are similar to each other and it is difficult to distinguish them by phenotypic characteristics. 3 A. baumannii is the most common species isolated from human clinical specimens, followed by such species as A. luffy, A. pittii, A. nosocomialis, A. haemolyticus and A. johnsonii.1–3 These bacteria are present everywhere in the environment including soil, water and food, as well as in the hospital environment including ventilators, moisturisers, catheters and other medical equipment. About 25% of adults carry Acinetobacter on their skin surface and 7% in their throats. In addition, 45% of patients who suffer from tracheotomy are also colonised by these bacteria.1,4 A. baumannii infections may lead to delays in wound healing in burn patients. 5
Infections caused by this organism are often found in intensive care units (ICUs) in patients with immunosuppression, in elderly patients with underlying illnesses such as malignancy and burns, in patients undergoing aggressive therapeutic procedures and in those who use broad-spectrum antibiotics. 6 Due to the clinical importance of A. baumannii, especially in burn patients, various methods have been developed to recognise them. The detection of A. baumannii infections in medical diagnostic laboratories of hospitals is usually carried out using phenotypic methods (including growth on MacConkey and blood agar media, and Gram staining) and differential biochemical tests, including oxidase, catalase, OF, TSI, motility, Simon Citrate, MR, VP and growth at temperatures of 37 °C and 44 °C. Today, different molecular methods have been developed to better understand the epidemiology and clinical significance of Acinetobacter species. However, most of them are very difficult for routine diagnostic applications in the microbiology laboratory and their uses are limited to reference laboratories.7,8 A simple and useful molecular technique for identifying A. baumannii isolates is the identification of the blaOXA-like-51 carbapenemase gene by PCR method. 9 OXA-TYPE genes, especially the subgroup OXA-51, have been studied in A. baumannii isolates around the world. This gene has a chromosomal position and can be used as a molecular reagent of A. baumannii. In other words, to differentiate the associated strains of Acinetobacter that are not interdependent, it is necessary to compare the isolates at the subtype level. Some typing methods have been designed to achieve this goal. Different typing systems are based on phenotypic tests and molecular techniques. Biotyping, serotyping and bacteriocin typing are examples of phenotypic typing methods, 10 most of which have now been replaced by molecular typing systems such as plasmid profile analysis, ribotyping, pulsed-field gel electrophoresis (PFGE) and enterobacterial repetitive intragenic consensus-polymerase chain reaction (ERIC-PCR).11,12
In A. baumanni, repetitive sequences of the gene which are called symmetric elements are often seen in the non-coding fragment of the DNA. Regarding the variable number and length of these repeat sequences, some primers have been designed. The length and number of bands obtained for each isolate are variable and the strains could be grouped according to the diversity of the bands.13,14
In this study, the molecular determination of A. baumannii isolates, which were collected and identified phenotypically and biochemically during August and September 2016 from burn wounds of hospitalised patients in a major burn hospital in Tehran, Iran, was performed by PCR using the primers of blaOXA-51 gene. The aims of the current study are to compare the results of phenotypic tests with those of the PCR method based on blaOXA-51 gene in detecting the isolates of A. baumannii from the burn wounds of hospitalised burn patients in a major burn hospital in Tehran and to investigate the genetic relationship between A. baumannii isolates by the ERIC-PCR method.
Material and methods
Identification of bacterial strains
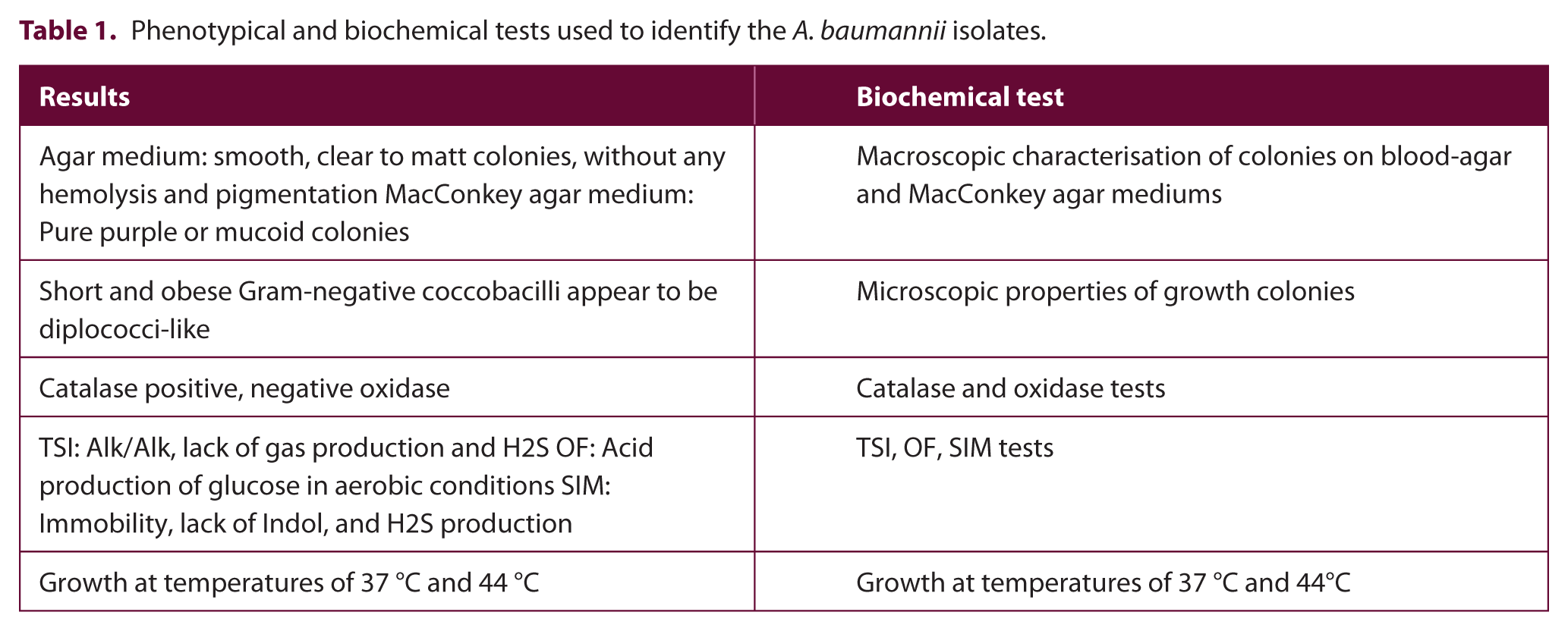
The present study was conducted based on the isolates of A. baumannii from burn wound swabs collected from patients hospitalised in a burn hospital in Tehran, Iran. All samples have been identified based on conventional microbiological tests (Table 1). The isolates were collected from patients aged 2–75 years and hospitalised for at least one week.
Phenotypical and biochemical tests used to identify the A. baumannii isolates.
Molecular detection of A. baumannii isolates
PCR was performed based on the identification of blaOXA-51 gene for the molecular detection of A. baumannii isolates. In the first step, the genomic DNA extraction of bacterial isolates and standard strain (A. baumannii ATCC 19606 as positive and Pseudomonas aeruginosa ATCC 27853 as the negative control) was performed by boiling method as follows. For this purpose, about 5–7 fresh colonies of the bacteria grown on the nutrient agar medium were removed and dissolved in 1.5-mL micro tubes containing 350 μL of sterilised deionised water. The micro tubes were placed in boiling water for 10 min. After shaking the micro tubs, centrifuge was operated at 12,000 rpm at 4 °C for 10 min. The supernatant containing DNA was transferred to another sterile micro tube. If the extracted DNA content had a good concentration and quality, it was stored at -20 °C until performing PCR. PCR mixtures were in a 25-µL volume comprising 11 μL DNase/ RNase-free water, 8 μL 2× PCR Master Mix (1.5 mM mgcl2, Denmark), 0.5 μL of each set of primers (blaOXA-51) and 5 μL of DNA template. The primers used in this study are shown in Table 2. The PCR program was set up in a thermo cycler (Senso-Quest Labcycler, Germany) as follows: 94°C for 5 min, followed by 30 cycles of 94 °C for 1 min, 55 °C for 1 min, 72 °C for 1 min and a final extension at 72 °C for 10 min. After doing PCR, 10 μL of PCR products were removed from each reaction mixture and examined by electrophoresis (80 V, 45 min) in 1% agarose gel in TBE buffer (40 mM Tris, 20 mM boric acid, 1 mM EDTA, pH of 8.3) containing 0.5 µg/mL DNA SafeStain dye. The gels were visualised under ultraviolet illumination using a gel image analysis system (UVitec, Cambridge, UK) and all the images were archived. Where a band was visualised at the correct expected size for blaOXA-51, the specimen was considered positive for A. baumannii. The positive results for blaOXA-51 were confirmed by sequencing of PCR products. Finally, the sequenced gene was read using the Chromas software (Version 2.1) and then compared and analysed by the NCBI website (http://www.ncbi.nlm.nih.gov/BLAST/).
Primer sequences of blaOXA-51 and ERIC.

Evaluation of genetic diversity by ERIC-PCR
To study the genetic diversity and clonal relationship of A. baumannii isolates, the numbers of genetic patterns of isolates were determined by specific primers of ERIC-PCR. The primers used for this step are shown in Table 2. The ERIC-PCR was performed as well as the PCR condition of blaOXA-51 gene. The ERIC patterns of A. baumannii isolates were analysed by online data analysis service (inslico.ehu.es). The ERIC patterns were clustered by UPGMA program and compared using Dice method, and finally, the dendogram was drawn.15,16
Results
During a two-month period, in total, 82 isolates that were phenotypically and biochemically confirmed as A. baumannii were gathered from a burn hospital in Tehran, Iran. The isolation process and biochemical identification of the isolates were carried out in a general hospital’s diagnostic laboratories. The methods and results of the phenotypic and biochemical tests which were used to identify the A. baumannii isolates are shown in Table 2. PCR test of the blaOXA-51 gene to validate the phenotypical identification of A. baumannii isolates showed that 80 (97.56%) isolates had the desired gene. Figure 1 shows the PCR product of the blaOXA-51 (353 bp) in some isolates of A. baumannii. Then one of the amplified products was sent to sequencing for the final confirmation of the molecular diagnosis.

The gel electrophoresis image of PCR product of blaOXA-51 (353 bp) DNA amplification in some isolates of A. baumannii and Pseudomonas aeruginosa ATCC 27853 as the negative control. Lane M: 100 bp DNA Ladder, Lanes 1–4: 353 bp bands of blaOXA-51.
Clonal diversity was recognised among 80 A. baumannii isolates by identifying 14 different ERIC patterns (ERIC-types) including 11 common types and three unique types with a similarity cut-off of ⩾ 95%. ERIC-type I was known as the predominant type comprised of 19 isolates (42.3%). Moreover, 17 isolates were clustered in genotype E, followed by G (nine isolates), J (six isolates), A, C and K (five isolates), H and B (three isolates), and F and M (two isolates). Other strains were distributed in other patterns and showed three single types. Our results classified 77 (96.25%) isolates into nine main genotypes (Figures 2 and 3).
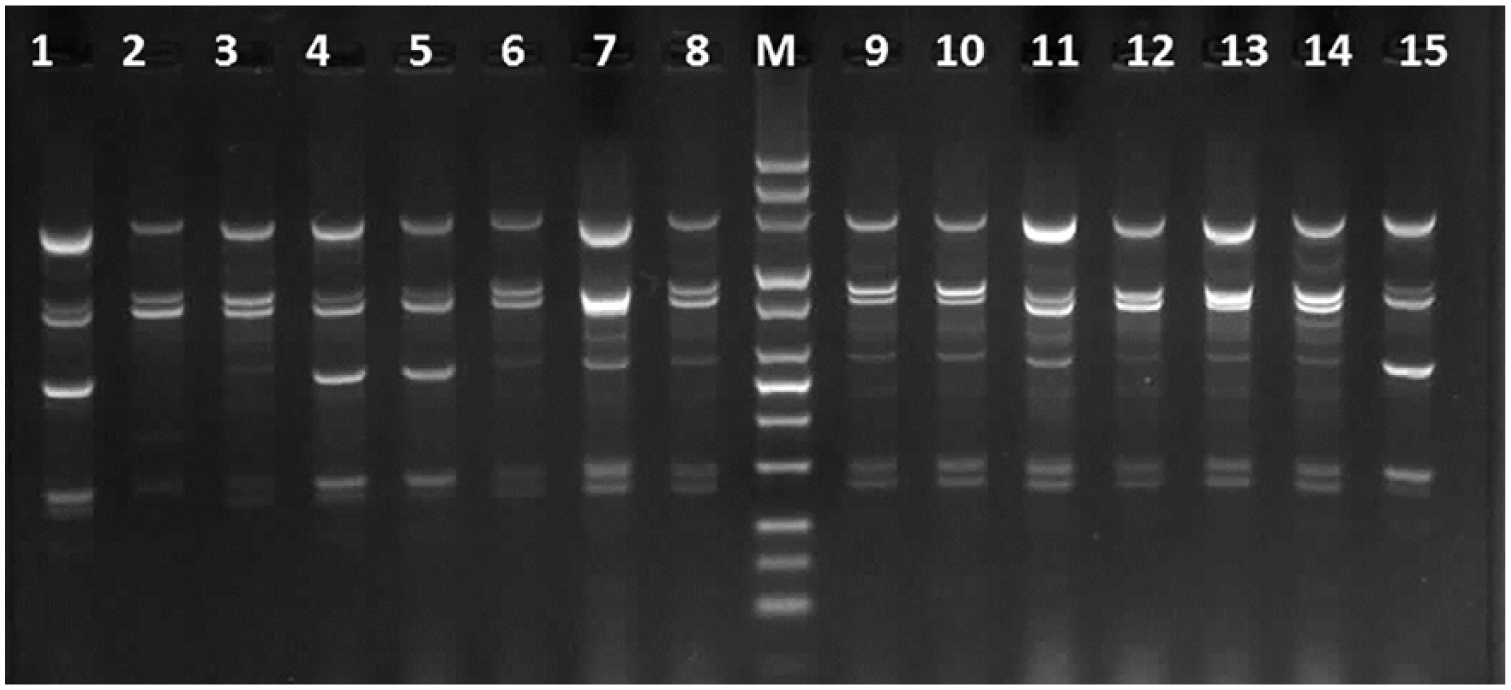
Gel electrophoresis image of different ERIC patterns of A. baumannii isolates from burn patients by ERIC-PCR. Lane M: 100 bp DNA ladder, Lanes 1–8 and 9–15: different ERIC patterns.
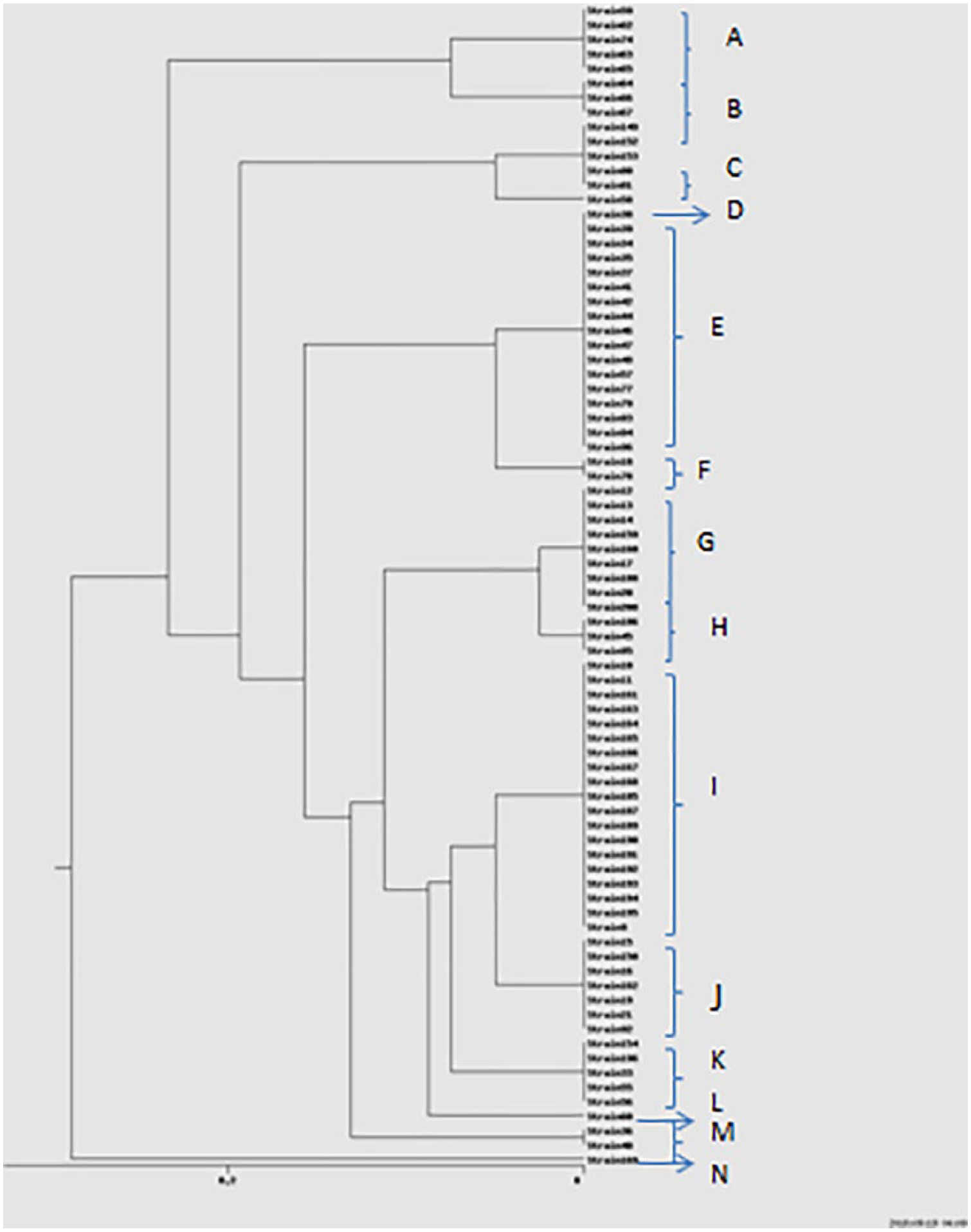
Dendrogram of ERIC-PCR analysis for 80 A. baumannii from burn wounds of patients in a burn hospital in Tehran.
Discussion
The prevalence of A. baumannii infection in different parts of hospitals is one of the major public health issues worldwide, especially in developing countries. A. baumannii is one of the most important microorganisms that cause nosocomial infections in hospitals and is difficult to control due to multiple drug resistance and persistence of the organism in the hospital environment. Some researchers believe that infections caused by A. baumanni, especially multi-drug resistant strains, are responsible for increasing the number of deaths from hospital infections. Another issue in this regard is that determining the true frequency of A. baumannii is challenging as the isolation of this microorganism from a patient can indicate the colonisation of patients by bacteria rather than the infection. However, many researchers have reported that colonisation of patients by multi-resistant Acinetobacter spp. can lead to serious infections.6,7
In Iran, like in other parts of the world, A. baumannii is one of the bacteria involved in hospital infections causing many health problems among hospitalised patients. People with cystic fibrosis, immunocompromised or defective immune defences, and especially burn patients, are at a high risk of A. baumannii infection. 19 In recent years, A. baumannii has become a major hospital pathogen, especially in the burn and ICU wards, so that it is the second most common nosocomial bacteria causing hospital infections leading to 10–43% mortality rates in patients admitted to ICUs. 17 Furthermore, several reports in Iran and many other countries are about the role of A. baumannii in hospital infections, especially in burn and ICU wards. In a study done by Hosseini et al. on 405 burn injuries in patients hospitalised in several hospitals of Tehran in 2006, 48 (11.8%) A. baumannii isolates were detected. 18 Asadollahi et al., in a study conducted between 2010 and 2011, demonstrated that the frequency of A. baumannii isolated from the wounds of patients admitted to the ICU of a teaching hospital in Tehran was 26.1%. 19 In the present study, 80 A. baumannii isolates were collected from the diagnostic laboratory of a burn hospital which is very high considering the duration of the research period (two months) compared to similar studies in other hospitals.20,21 Since this level of infection was found in hospitals during a two-month period, further investigation is needed to determine whether there is a problem with cross-transmission, either within the hospital in question and/or other hospitals from which patients are received into this hospital. Our hospital is the major burn center and many burn patients from other hospitals are hospitalised in the ICU of the targeted hospital; in addition, many clinical samples are transferred from other hospitals to this one for the culturing and confirmation of bacterial identification. Therefore, due to the high incidence of nosocomial infections such as A. baumannii in burn patients and other patients hospitalised in different hospital wards, a comprehensive infection detection and controlling protocol in the hospitals’ different areas where this organism is permanently active is necessary. Identification of Acinetobacter species in microbiological laboratories is usually based on phenotypic characteristics. However, these methods are not completely reliable and sometimes cause problems in interpreting the results. Based on the phenotypic identification method, Acinetobacter species can be distinguished in terms of acid production from glucose, gelatin hydrolysis, hemolysis, different carbon sources and finally its ability to grow at temperatures of 37 °C, 41 °C and 44 °C.1,2 Today, molecular techniques have been developed to identify microbial species. The accuracy, speed, identification and interpretation of molecular methods is higher than those of phenotypic identification method. Most studies in Iran have been conducted to evaluate the antibiotic susceptibility patterns in clinical strains of A. baumannii and there is little information about genetic characteristics and clonal diversity patterns.
Acinetobacter species are often isolated from the damp areas of the skin and occasionally from the throat, respiratory and gastrointestinal tracts of hospitalised patients. Other sources of these bacteria include medical equipment in the hospital and hospital staff. In the hospital environment, these microorganisms have been isolated from multiple contaminated medical supplies such as ventilator tubes, respirometers, arterial blood pressure control devices as well as a wide range of environmental objects such as gloves, mattresses, pillows and other medical equipment.22,23 In a study in Spain, > 90% of A. baumannii infection was reported through hospitalisation and only 4% of the infection originated from outside the hospital environment. 24 In most epidemic cases of A. baumannii, patients are usually the initial source of A. baumanii outbreaks. The best way to prevent the spread of nosocomial infections, especially in burn patients, is through the use of precautionary measures, with continuous monitoring of the hospital environment by quick and accurate detection of Acinetobacter spp. and taking control measures. 25
Several studies have reported genetic diversity and heterogeneity among A. baumannii isolates using different molecular typing methods as well as ERIC-PCR. It is well-known that the ERIC-PCR technique is much cheaper and easier to perform than other PCR-based typing methods. 26 In this study, ERIC-PCR showed genetic diversity among A. baumannii isolates, of which two ERIC-types were predominant. The study of the isolates of these types is very useful for the identification of the major A. baumannii clones circulating in burn hospitals.
Conclusion
According to the results of this study, molecular techniques such as PCR and ERIC-PCR are very useful for identifying A. baumannii and for studying the genetic linkages of clinical isolates of A. baumannii in hospitals, respectively, especially for burn patients due to their susceptibility to nosocomial infections. Clonal diversity was also found among A. baumannii isolates in burn patients. Therefore, controlling the endemic strains of Acinetobacter baumanii is required, especially in burn hospitals
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.