
Abstract
Introduction:
Autologous platelet-based concentrates represent increasingly popular adjuncts to a variety of medical, surgical and aesthetic interventions. Their beneficial potential rests on the ability to deliver a high concentration of growth factors to the target tissues. There are currently no reports in the literature appraising the evidence behind the use of platelet-rich plasma (PRP) in scar management.
Methods:
A detailed English literature review was conducted using PubMed Medline, Embase and Web of Science; the manuscripts were appraised and classified according to the Joanna Briggs Institute Levels of evidence. The results are presented in descending order of evidence separately for atrophic, keloid, surgical and traumatic scars.
Discussion:
On the basis of level 1 evidence currently available, it appears that PRP can improve the quality of atrophic acne scars treated with ablative fractional CO2 laser and decrease the duration of laser-related side effects including oedema and erythema. Regarding surgical scars, the current data suggest that PRP may improve wound healing and early scar quality; furthermore, incorporation of PRP in fat-grafting procedures undertaken in conjunction with non-ablative, fractional laser can contribute to better wound healing as well as a significant improvement in texture, colour and contour in traumatic scar resurfacing. There are no high level studies at present to support the incorporation of autologous platelet-based concentrates in the management of keloid scars.
Conclusion:
PRP is a promising adjunct in scar management practice. Further research with long-term follow-up is warranted to delineate the value of this modality in different subtypes of scars.
Lay summary
Platelet-rich plasma (PRP) is an increasingly popular product used in a variety of medical, surgical and aesthetic interventions; it is derived by spinning down a patient’s own blood and applying it back to an area of the body undergoing an intervention. We undertook this study to find out whether the use of PRP can have a beneficial effect on scars. We conclude that at present there is some evidence that it may improve the quality of depressed acne scars and ameliorate the duration of side effects associated with fractional laser treatment. Furthermore, PRP can improve healing parameters and early scar quality following a Caeserean section as well as enhance outcomes if used in combination with fat grafting and fractional laser for the revision of traumatic scars. The evidence behind the role of PRP for the management of keloid scars is low at present. Most studies do not assess long-term results, so further research is needed before PRP is widely adopted in scar management protocols.
Introduction
Platelet-rich plasma (PRP) is an autologous blood-derived product enriched in platelets, growth factors and chemo/cytokines delivered in a concentrated volume of plasma. Since the 1970s, PRP has received significant attention as applied to tissue repair and regeneration.1,2 Initial studies focused predominantly on applications within the musculoskeletal and maxillofacial fields; however, in recent years, it has been used for a range of dermatological indications including wound healing, fat grafting, alopecia, scar management as well as soft-tissue volume augmentation. 3
PRP has the potential to deliver a high concentration of growth factors to target tissues by virtue of the contents within the alpha and dense granules.
Degranulation of these organelles results in the release of pre-packaged growth factors, many of which have short half-lives; therefore, greater effectiveness may result if they are activated at or just before application. PRP has 3–5 times the concentration of platelets normally found in wounds and the resulting growth factor release following activation can further stimulate cell proliferation and differentiation towards tissue regeneration. 8
PRP is prepared either manually or using automated devices or kits. In the manual method, blood is withdrawn from the patient, an anticoagulant is added and the mixture is centrifuged. In the double spin-method, blood is separated into three layers: platelet-poor plasma (PPP) at the top of the tube; PRP in the middle; and red blood cells (RBCs) at the bottom (image 1). The RBCs are discarded and following the second centrifugation, the PPP is discarded. The end product consists predominantly of PRP and thrombin or calcium chloride is subsequently added as a platelet activator.7,8 The value of the second centrifugation relates to the concept that after a single spin, the RBCs interfere with the fine separation of the platelets regardless of the rate or the time of centrifugation, hence producing a preparation with less percentage of PRP.9,10

Appearance of whole blood centrifugates illustrating the separation of platelet (top) and red blood cell (bottom) portions before the platelet rich plasma (PRP) is extracted for clinical use.
Various automated devices and kits have been manufactured in the last few years in order to facilitate the delivery of ready-to-apply PRP without the need for manual separation. The limitation associated with the wide range of available automated devices/kits is that their products are likely to have different growth factor concentrations; this poses challenges in comparing clinical efficacy. Some of them have been approved by the U.S. Food and Drug Association (FDA), e.g. Smart PReP® (Harvest Technologies Inc, Plymouth, MA, USA), PCCS® (3i Implant Innovations Inc, West Palm Beach, FL, USA), BioMet GPSII®, etc. 11
The current consensus classification system for the four main categories of autologous platelet concentrates is based on their fibrin architecture and cell content:
PRP can be applied as an isolated modality or as an adjunct to minimally invasive and surgical interventions given its potential to improve repair and regeneration.13–15 Scar management is an expanding field encroaching a number of disciplines including plastic surgery, dermatology and physical therapy to mention a few.
A number of animal models have been used over the last few years to assess the effectiveness of PRP in the treatment of different types of scars. There is preliminary evidence in a canine model 16 that application of autologous PRP using the subcutaneous infiltration route at the wound margins can produce a significant enhancement of wound re-epithelisation and a reduction of scar formation at weeks 1 and 3 in comparison to controls. Malondialdehyde (MDA) concentration, which is a marker of oxidative damage, was also significantly decreased in PRP-treated wounds in this work; furthermore, the activity of matrix metalloproteinase 9 (MMP-9) reached its peak at the second week and was significantly higher in the PRP-treated group.
In another experimental rat uterine horn adhesion model, the inflammatory cytokine tumour growth factor 1 beta (TGF-1beta) expression was significantly reduced in the PRP-treated group compared to the control and hyaluronic acid groups; these findings prompted the authors to conclude that PRP is a promising and effective adjunct in the prevention of postoperative adhesion development. 17 The aim of this article is to review the current available evidence on the efficacy of platelet preparations in the management of scars and present future directions for research in the field.
Methodology
A detailed English literature review was conducted of the following databases: PubMed Medline; Embase; and Web of Science. The following keywords were used: ‘platelet-rich plasma AND scar’; ‘PRP AND scar’; ‘PRP AND keloid’; ‘hypertroph* AND platelet-rich AND plasma’; ‘platelet-rich plasma AND hypertroph* AND scar’. Our search retrieved 52 citations; all abstracts were screened by both authors to ensure relevance. A total of 36 articles were selected for inclusion into our work; following full detailed manuscript review, 20 were deemed relevant to be presented in our analysis. The selected papers were appraised and classified according to the Joanna Briggs Institute Levels of evidence with the help of an independent research consultant in evidence synthesis. 18
We present our findings based on a categorisation system according to the type of scars platelet-rich preparations were applied to, namely atrophic, keloid, surgical and traumatic scars.
Results
Atrophic acne scars
Atrophic scars are the most common type of acne scars; they can be further subdivided into ice pick, boxcar and rolling subtypes. 16 A variety of management modalities have been employed including laser resurfacing, chemical peeling, dermal fillers, dermabrasion, needling, subcision and punch excision. 17 PRP is a recently introduced adjunct and has been used predominantly in combination with other modalities.
Lee et al. 19 carried out a split face study in 14 Korean patients who underwent ablative fractional laser resurfacing and were randomly assigned to receive either injectable PRP or normal saline following the treatment episode. The PRP was extracted with a double spin-method and produced 6 mL for each patient; injection points were spaced 1.5–2 cm apart.
The laser settings were: pulse energy 25 mJ per fixed 150-μm diameter microbeam and a density of 400 MTZ/cm2 with concurrent forced air cooling for epidermal protection; assessment was performed with the help of a standardised photographic method by blinded dermatologists. Erythema on the PRP side improved faster compared to controls and was significantly less at day 4 as confirmed by chromometer readings (P = 0.01 and 0.047, respectively). Duration of oedema as well as crusting were significantly shorter in the PRP group (6.1 ± 1.1 vs 7.1 ± 1.5 days and 5.9 ± 1.1 vs. 6.8 ± 1.0 days, P = 0.04) and the overall clinical improvement four months after treatment was superior on the PRP arm (2.7 ± 0.7 vs. 2.3 ± 0.5, P = 0.03).
In another study, Gawdat et al. 20 compared the efficacy of topical versus intradermal PRP (double-spin method) after ablative fractional CO2 laser (FCL) using a single-blind randomised split-face study design in 30 patients with facial atrophic acne scars (Fitzpatrick skin types III to V). Group 1 underwent ablative fractional CO2 laser followed by intradermal PRP on one side and intradermal saline on the other; Group 2 had FCL followed by intradermal on one side and topical PRP on the other side. Each patient received three treatment sessions at monthly intervals. The settings for the laser were as follows: 15 W, dwell time 600 ms, spacing 700 μm, smart stack level 2. The injectable PRP and saline were administered in 0.2-mL volumes and injected at 1.5 cm apart; topical PRP was applied in 2-mL volumes. Photographic assessment comparison by a blinded physician using a four-point scale (excellent to poor) at three months after the last session showed that the combination of ablative fractional CO2 laser and PRP (topical and intradermal administration) showed significantly better results than ablative fractional CO2 laser alone (P = 0.03). Interestingly, no significant difference was observed between topical and intradermal PRP adjuvant administration (P = 0.10). Results based on a patient clinical satisfaction scale showed a similar trend to the above physician-reported outcomes. Side effects including erythema, oedema, post-inflammatory hyperpigmentation and acneiform reaction were all of a significantly shorter duration in the PRP-treated areas (P = 0.02) leading to significantly shorter downtime. Results regarding scar depth using optical coherence tomography showed that the PRP-treated areas were improved in a statistically significant manner (P = 0.01). In conclusion, this study showed that the combination of PRP and ablative fractional CO2 laser produced a better resurfacing response, fewer side effects and quicker recovery than laser alone; additionally, given that there was no statistically significant difference between the results obtained with topical versus intradermal PRP, the authors advocate the topical administration in order to minimise discomfort associated with the injectable route.
Nofal et al. 8 conducted a quasi-experimental prospective controlled study on 45 patients with atrophic acne scars of varying severity. The cohort was divided into three groups of 15 patients each undergoing one of the following treatments: (1) intradermal injection of PRP; (2) application of 100% trichloroacetic acid (TCA)-CROSS; and (3) combination therapy of skin microneedling and topical PRP. Each patient underwent three sessions at two-weekly intervals. Results were assessed using the qualitative global acne scarring grading system (QGSGS) by two blinded dermatologists using photographs before and two weeks after the last treatment. Patient satisfaction ratings were also obtained. QGSGS findings suggested that a highly significant improvement in scar severity was seen after all modalities (P < 0.001); namely, an excellent to very good rating was found in 46.7% of the PRP group, 26.7% of the TCA CROSS group and 60% of the PRP with microneedling group. Nevertheless, none of the three treatments were significantly superior in comparison (P = 0.87) with regards to the quartile grading scale as well as patient satisfaction ratings. Limitations of this study include apart from the small cohort size, the large number of variables (including the number of treatment sessions used, the depth of needling as well as the mode of PRP administration), which make any valid conclusions challenging.
Similarly, Ibrahim et al. 21 compared microneedling alone to combined microneedling and PRP for post-acne atrophic scars as part of a split-face comparative study involving 35 patients. All patients (Fitzpatrick skin types I–IV) were treated with four sequential microneedling sessions using a 1.5 mm dermaroller to pinpoint bleeding alone on the right side of the face, and a combination of microneedling and topical PRP on the left side with an interval of three weeks between sessions. The follow-up period was three months following which, two blinded dermatologists performed photographic evaluation using the Goodman and Baron grading system. Patients also graded their response as poor, good, very good or excellent. Both treatment modalities produced a significant improvement in the global acne scoring system, namely from 3.2 ± 0.7 to 1.8 ± 0.6 for the right side and 2.1 ± 1.1 for the left side (P < 0.001); nevertheless, the difference between both modalities were not statistically significant (P = 0.73). A similar trend was observed with regards to the patient satisfaction scores for both modalities. Interestingly, there was a statistically significant difference in the post-procedural erythema and oedema in favour of the PRP-treated side (P < 0.001); hence the authors concluded that PRP can minimise side effects of microneedling in acne management.
Another split-face randomised controlled study was performed by Faghihi et al. 22 in which 16 patients (Fitzpatrick skin type II–IV) with atrophic acne scars received ablative fractional CO2 laser combined with intradermal PRP treatment on one half of their face and laser with intradermal normal saline (NS) on the other half. The PRP was prepared using a two-stage centrifugation process and was injected intradermally within 2-cm intervals to an overall volume of 0.2-mL following ablative CO2 laser session (settings: power 25 W; duration of 3; energy 30 mJ; pixel pitch of 1; and ablation depth of 600 μm). Participants received two treatment cycles one month apart. Serial digital photography at baseline, one month after the first session and four months after the second session were obtained and a quartile improvement grading scale was used by two blinded dermatologists to evaluate the overall clinical improvement. Participants were asked to grade overall satisfaction based on a range between 0–3 (slightly to very satisfied) and a 0–10 visual analogue scale was used to record adverse effects (erythema and oedema). The overall clinical improvement of acne scars was higher on the PRP-laser treated side, but the difference was not statistically significant either at one month following the first session or four months following the final session (P = 0.15 and 0.23). Moreover, the adverse effects including erythema and oedema were more severe and of longer duration in the PRP-laser treated side in a statistically significant manner. In this work, PRP addition to the laser modality appears to produce more severe side effects and longer downtime.
Abdel et al. 23 conducted a similar study in which he treated 30 patients suffering from post-acne scars with ablative fractional CO2 laser (settings: 15 W, 600 ms dwell time, spading 700 μm, smart stack level 3); Only the right side of the face received intradermally injected autologous PRP (0.1 mL per point separated by 1–1.5cm). The laser was applied in two separate sessions (every 3–4 weeks) and patient’s follow-up was completed six months after the final laser session. Assessment was done by two blinded dermatologists based on digital photographs; additionally patients filled out a questionnaire to grade their improvement. The overall improvement of the right side based on the Qualitative Global Grading System was better than on the left side (P < 0.001). The resolution of erythema following the laser was faster on the PRP-treated side (P = 0.0052) and post-inflammatory pigmentation did not occur on the treated side; the occurrence of acneiform eruption was also significantly lower on the treated side. In addition, patient satisfaction was also higher on the PRP-treated side (P < 0.001).
Chawla 24 performed a study to investigate the efficacy of PRP versus vitamin C as adjuncts to microneedling for the treatment of atrophic post-acne scars as part of a split-face prospective study. Four sessions separated by a four-week interval were offered to 30 patients (Goodman and Baron grades II–IV), 23 of which completed the study. A double-spin method was used for the PRP and 1.5-mm needling rollers were used. At the end of the four treatments, photographic assessment was undertaken by the patient and treating physician and improvement was graded on a scale from poor to excellent. Results suggest that PRP compared favourably as contributing to an excellent outcome by the physician (18.5% vs. 7%) and also to those who had a poor response (37% vs. 22.2%); additionally, patient scores indicated that patients were more satisfied with the PRP adjunct (P = 0.01).
Zhu et al. 25 examined the combination of topical PRP with erbium fractional laser for the treatment of 22 patients (Fitzpatrick type III or IV) with facial atrophic acne scars. The settings for the laser treatment were: pulse duration 300–600 ms; pulse energy 600–1200 mJ; microbeam diameter 2–7 mm; and penetration depth 18–24 μm. At 1–3 month follow up, digital photography assessed by two blinded dermatologists showed difference of 2.77 ± 0.39 corresponding to moderate improvement; additionally, self-evaluation using a quartile grading scale was shown to have improved by 3.3 ± 0.36 and 91% of the patients were ‘very satisfied’.
Nita et al. 26 treated 64 patients suffering from 43 atrophic and 21 ‘contractile’ scars involving different body parts with combination of ablative fractional CO2 laser, PRP and autologous fat grafting. Standard fat harvesting and the Coleman technique were employed for the lipofilling technique and fractional CO2 laser settings (power 9–12 W, time 4 ms, medium density) were matched to skin type. The PRP was obtained after two centrifugations (GLOFIN, Salo, Finland kit) and injected in the mid to deep dermis. At six-month follow-up, the overall patient satisfaction rate was > 50% (55.81% for atrophic and 52.38% for contractile scars). The authors proposed that the combination of the three modalities seems to be an effective approach for scars. Table 1 summarises the salient literature reports relating to the use of PRP and atrophic acne scars.
A summary of the different studies investigating the role of PRP in the management of atrophic acne scars.

Keloid scars
Level 4
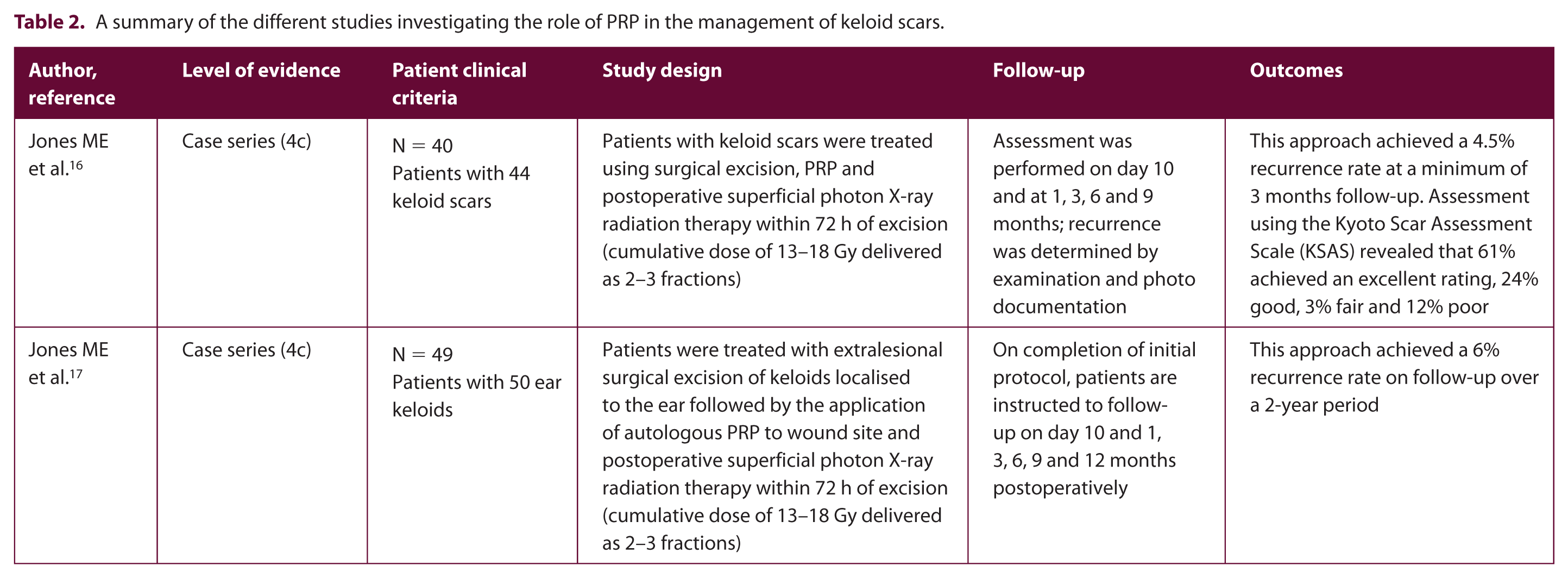
Keloids represent a particularly challenging subset of scars for which a variety of therapeutic approaches have been described including surgical excision and radiotherapy, intralesional steroid injection and cryotherapy. 27 Jones et al. 28 recruited 40 patients (with 44 keloid scars) and treated them using a combination of:
Extralesional surgical excision;
PRP (2–3 mL) applied to the excision wound bed and incision site; and
Postoperative superficial photon X-ray radiation therapy within 72 h of excision (cumulative dose of 13–18 Gy delivered as 2–3 fractions).
All patients were advised to use a corticosteroid-based cream (0.5% hydrocortisone) twice daily for the first three months; additionally, triamcinolone injections were administered to four patients who were scored ‘poor’ on the Kyoto Scar Assessment Scale (KSAS); the latter was employed to assess scar outcomes in the study. This novel protocol approach achieved a recurrence rate of 4.5% (defined as induration, hypertrophy or extraordinary erythema beyond the site of excision) at a minimum three-month follow-up (range = 3–11 months). Assessment using the KSAS revealed that 61% achieved an excellent rating, 24% good, 3% fair and 12% poor. Radiation-induced hyperpigmentation was noted in all patients in the study. Limitations of the study included the short follow-up period, the non-standardised radiation protocol used as well as the variable use of triamcinolone; these factors make it very challenging to identify the exact contribution of PRP in the final recurrence rate. The same author 29 reported results of a retrospective study on 49 patients with 50 ear keloids treated with the same combination therapy as described above and achieved a 6% recurrence rate with a two-year follow-up period.
Currently, there is an ongoing randomised controlled trial (RCT) to assess the efficacy of autologous PRP administered immediately after complete surgical excision and then subsequently within the first month postoperatively on three occasions. 30 Given the limitations of the reported studies so far, results are eagerly awaited to assess the role of PRP in keloid scar management. Table 2 summarises the salient literature reports relating to the use of PRP and keloid scars.
A summary of the different studies investigating the role of PRP in the management of keloid scars.
Surgical scars
Surgical or postoperative scars have received special attention in the literature in the last few years and a limited number of studies have investigated the role of PRP in optimising final scar quality.
Level 1
Tehranian, et al. 31 conducted a RCT involving 140 patients undergoing elective Caesarean delivery. They were randomly allocated into two groups; the intervention group received PRP applied to the subcutaneous tissues of the wound before closure, whereas the control group received the usual care (i.e irrigation of the wound with saline before closure). Patients were examined by blinded physicians on days 1 and 5 as well as eight weeks after the procedure using a visual analogue scale for postoperative pain (VAS) and the Redness, Oedema, Ecchymosis, Discharge, Approximation (REEDA) scale to assess wound-healing progress; the Vancouver Scar Scale (VSS) was additionally used to grade the quality of scar formation. The authors identified that patients who were treated with topical PRP had a significant reduction in the REEDA score (85.5% for PRP vs. 72% for control group, P < 0.0001) implying better healing progress. Regarding the VSS, treatment with PRP had a significant effect on reducing the score beginning on the fifth day and continuing with a stable trend at the end of the eight weeks (54% vs. 18% reduction, P < 0.001). Furthermore, based on the VAS score for pain, PRP contributed to statistically significant reduction of pain experienced at the end of the follow-up period (93% vs. 79%, P < 0.001). Limitations of this study include the very short follow-up, which did not extent into the remodelling phase of scar maturation.
Level 4
Azzena et al. 32 reported a case of a painful adherent postoperative scar following a shoulder replacement surgery in which they injected a gel mixture of autologous adipose tissue combined with PRP into a subcutaneous pocket using a novel in vivo adipocyte delivery system. The patient reported complete remission of pain and ultrasonography performed six months and one year after treatment showed enhanced fat survival and resolution of the adhesion with the underlying fascia. Table 3 summarises the salient literature reports relating to the use of PRP and surgical scars.
A summary of the different studies investigating the role of PRP in the management of surgical scars.

Traumatic scars
Scarring following trauma can lead to both aesthetic and functional sequelae for patients; 33 a small number of studies have investigated the role of PRP in this subset of scars.
Level 1
Cervelli et al. 33 recruited 60 patients (Fitzpatrick skin types II–IV) affected by traumatic scars of varying aetiology in different bodily parts. They were randomly allocated to one of three groups (20 patients each): group A was treated with fat grafts mixed with PRP at one and three months; group B underwent four sessions of 1540-nm non-ablative laser alone (settings: 20–40 J/cm2 using a 10-mm fractional handpiece); and group C was treated with a combination of both procedures (laser at one and three months delivered seven days after the graft/PRP). The PRP was extracted with a single-spin preparation and was added to the fat (harvested using the Coleman technique) before injection at volumes in the range of 5–50 mL depending on the defect. The combined modality group showed greater overall clinical improvement in comparison to the other groups as assessed using the Manchester Scar Scale (MSS). The most effective scar treatment was the combination of the fat graft-PRP and non-ablative laser resurfacing in group C, which had increases in wound healing of 22% and 11% compared with groups A and B, with significant improvement in texture, colour and scar contours on MSS. The authors concluded that the addition of PRP to a combination of fat grafting and non-ablative 1540-nm laser increases the efficacy of the combined scar management strategy.
Level 2
Gentile et al. 34 conducted a comparative study on 20 patients with burn and traumatic scars using either stromal vascular fraction (SVF)-enhanced autologous fat grafts or 1 mL of Coleman-based fat grafting mixed with 0.5 mL of PRP; in this study a control group of 10 patients were treated with centrifuged fat without PRP addition. The fat re-implantation was performed following scar subcision with 1.5-mm diameter cannulas. In both groups (study and control), one operation was required in six cases and two in four cases. Evaluation was performed using photographic team evaluation and radiological assessment as well as patient self-evaluation. In patients treated with PRP-enriched fat, 69% maintenance of contour and three-dimensional volume after one year was observed in comparison to the control group. Magnetic resonance imaging (MRI) additionally showed that patients treated with PRP as well as SVF-enriched fat showed lower fat absorption. The authors concluded that use of PRP during fat grafting improves adipose tissue maintenance and survival.
Level 4
Majani et al. 35 evaluated the results of lipografting in 28 patients with different types of scars (including burn cicatricial, traumatic and postoperative scars). Eleven patients (group 1) received lipografting only and 11 (group 2) were treated with PRP 7–10 days before the surgery; six patients (group 3), who had symmetrical scars, were treated on the left side only with lipografting and on the right side with a combination therapy of PRP and lipografting. The PRP was obtained using a single-spin technique and infiltrated into the scars in volumes in the range of 1–8 mL and fat was injected in volumes in the range of 8–37 mL. Patients were photographed at 30, 90 and 180 days postoperatively. Thirty days following lipografting, all patients showed better scar elasticity and the treated area showed evidence of aesthetic improvement. Ninety days after surgery, in three patients from group 1 and one patient from group 2, there was absorption of the injected fat. In patients from group 3, the increase was most evident on the right side. The authors concluded that a suitable preparation of the treated areas with the combination therapy of PRP and lipografting resulted in more durable corrections, particularly in situations where vascularization is more impaired. Table 4 summarises the salient literature reports relating to the use of PRP and traumatic scars.
A summary of the different studies investigating the role of PRP in the management of traumatic scars.

Discussion
Based on the studies available in the field of atrophic acne scarring, there is level 1 evidence that PRP in conjunction with ablative fractional CO2 laser treatment may improve the overall clinical response/quality of scars attained and decrease the duration of laser related side effects including erythema and duration of oedema.19,20 Additionally, there appears to be no statistically significant difference between the intradermal and topical application of PRP after fractional CO2 laser treatment in terms of efficacy. 20 Level 2 studies suggest that PRP can decrease erythema and oedema following 1.5-mm microneedling in a statistically significant manner. 21 Another study in this category of evidence failed to show statistical superiority of PRP and skin microneedling compared with TCA CROSS and isolated intradermal PRP administration on the basis of QGSGS ratings. 8 Furthermore, two other level 2 studies provided contradictory results around the role of PRP in ameliorating post-fractional CO2 side effects including erythema resolution.22,23 Some of the main limitations of the studies available in this arena include the small cohort sizes as well as their short follow-up period (range = 2–6 months); this is very limited given that the timescale of scar remodelling is considered to span over at least 12 months. Furthermore, the heterogeneity of treatment parameters (volume/concentration of PRP, laser settings, Fitzpatrick skin types) may render generalised conclusions challenging.
There is weak evidence (level 4) for the inclusion of PRP in the management of keloid scars employing surgery and radiotherapy. The non-comparative design of the two available studies, the selective use of steroids to a significant percentage of patients as well as the short follow-up period in one report (deviating significantly from the widely accepted minimum two-year period to assess long-term efficacy reliably) make valid conclusions challenging to draw.27,28 The results of the currently conducted RCT are eagerly awaited to appraise the value of PRP in keloid scar management.
Regarding surgical scars, there is level 1 evidence that autologous platelet preparations may improve wound healing and scar quality at eight weeks as well as mediate a reduction in postoperative pain following a Caesarean section; nevertheless, the short follow-up in the study does not provide an indication of the possible contribution of PRP towards better long term scar quality. 31
Reviewing studies in resurfacing of traumatic scars, the addition of PRP in fat-grafting procedures combined with non-ablative, fractional 1540-nm laser appears to contribute to better wound healing compared to isolated modalities (PRP-enriched fat grafting and laser alone). Furthermore, MSS scores indicated a significant improvement in texture, colour and scar contours at six-month follow-up. 33 Another level 2 study showed that PRP enrichment of autologous fat grafts can improve adipose tissue survival and maintenance during fat grafting at 12-month follow-up. 34
Concluding remarks
This work appraised the literature concerning the use of PRP in scar management. The use of autologous plasma derived adjuncts has a number of potential advantages by virtue of the ability to deliver a high concentration of growth factors to target tissues and potentially improve wound healing and scarring parameters. The majority of studies currently available focus on the adjunctive use of PRP in the management of atrophic acne scars; nevertheless, there are significant shortcomings in this arena including the small cohort sizes appraised, the short follow-up periods as well as the heterogeneity of treatment parameters employed, which render generalised conclusions challenging. Further high-quality studies are eagerly awaited in order to further delineate to role of autologous platelet-derived adjuncts in scar management protocols.
Footnotes
Acknowledgements
We would like to acknowledge Ewelina Rogozinska (research consultant in evidence synthesis) for her assistance with the categorisation of the included studies into levels of evidence and Alistair Turner, BTI Biotechnology Institute, UK for providing the image included in the manuscript.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.