
Abstract
Introduction:
Dynamic monitoring of coagulation is important to predict both haemorrhagic and thrombotic complications and to guide blood product administration. Reducing blood loss and tailoring blood product administration may improve patient outcome and reduce mortality associated with transfusion. The current literature lacks a systematic, critical appraisal of current best evidence on which clinical decisions may be based.
Objectives:
Establishing the role of different coagulation markers in burn patients, diagnosing coagulopathy, tailoring blood product administration and indicating prognosis.
Methods:
Literature during 2004–2017 from the Cochrane Library, PubMed, Scopus, Medline and Embase was reviewed. Eligibility criteria included randomised controlled trials, systematic reviews, multi-/single-centre study and meta-analyses. Keywords searched were ‘burns’, ‘blood coagulation disorders’, ‘rotem’, ‘blood coagulation’ and ‘thromboelastography’. The PRISMA flow system was used for stratification and the CASP framework for appraisal of the studies retrieved.
Results:
In total, 13 articles were included after inclusion/exclusion criteria had been applied to the initial 79 studies retrieved. Hypercoagulation increases in proportion to the severity of thermal injury. Whole blood testing, using thrombelastography (TEG) and rotation thromboelastometry (ROTEM), was superior to standard plasma based tests, including prothrombin time (PT) and activated partial thromboplastin time (APTT) at detecting burn-related coagulopathies.
Conclusions:
Routine laboratory markers such as PT/APTT are poor indicators of coagulation status in burns patients. Viscoelastic tests, such as TEG and ROTEM, are efficient, fast and have a potential use in the management of burn patients; however, strong evidence is lacking. This review highlights the need for more randomised controlled trials, to guide future practice.
Lay Summary
Introduction:
It is important to measure how easily or how difficult it is for blood to clot in patients who have sustained severe burn injuries. By doing this, we can predict bleeding and blood-clotting risks and it can help us determine when blood transfusions are needed. The medical literature does not currently have any articles which systematically summarise the best evidence regarding this topic.
Methods:
Databases containing medical research articles were searched in a systematic way and each article was scrutinised for its quality and how reliable the conclusions are based on how the study was performed.
Results:
Seventy-nine scientific articles were identified and narrowed down to 13 relevant ones. Patients with larger burn injuries are more likely to suffer abnormalities in their blood which leads to blood clotting more easily than normal. Blood tests called thrombelastography (TEG) and rotation thromboelastometry (ROTEM) seemed to be better than standard blood tests called prothrombin time (PT) and activated partial thromboplastin time (APTT) at detecting clotting disorders in burn patients.
Conclusions:
Standard blood clotting tests such as PT and APTT are not good at detecting blood-clotting abnormalities in burns patients. Other tests, TEG and ROTEM, are an efficient and fast way of monitoring blood clotting in burns patients. These tests have a potential use in the treatment of burns patients, but strong evidence to support this statement is lacking. This study highlights the need for more evidence, especially bigger and better research studies to guide future recommendations.
Keywords
Introduction
Thermal injury involves a complex interplay between early activation of uncontrolled coagulation and fibrinolysis, coupled with an increase in various inflammatory mediators.1–3 Bleeding remains a major challenge during early excisional surgery and is a predictor of mortality.4,5 A study investigating burn injuries > 40% total body surface area (TBSA) found that the median red blood cell (RBC) and plasma transfusion required was 19 units and 28.5 units, respectively, during an admission. 6 Coagulopathy has been repeatedly identified as a risk factor for increased morbidity and mortality in the early post-burn period as well as in later clinical course.7,8 Although the underlying pathophysiology behind this coagulopathy is not completely understood, the body of knowledge in this area has increased in recent years. Patients may require a significant amount of blood products which worsen the patient’s prognosis due to defects in the ability of fibrinogen to form firm clots, increased chance of infectious complications, organ failure and respiratory distress. 9 A combination of reducing blood loss and tailoring blood product administration could improve patient outcome and reduce mortality. Evidence in other specialties such as trauma and cardiac surgery demonstrates blood transfusions in bleeding patients can be reduced with rapid and targeted correction of coagulopathy; 10 whether this applies to burn patients is unknown.
Traditionally, plasma-based routine coagulation tests, including activated partial thromboplastin time (APTT) and prothrombin time (PT), are used to monitor coagulopathy. These tests are adequate predictors of mortality in trauma patients; however, as APTT and PT only reflect the small amount of thrombin formed during the acute phase of coagulation, they are of limited use in the management of burns patients. Following burn injury, the patient’s coagulation status may change considerably as a response to the systemic inflammatory response over the first week, and as a result of interventions such as haemodilution and during fluid resuscitation and excisional surgery.8,11 An additional confounding variable is that APTT and PT are performed under non-physiological conditions and the delay in processing often means the patient’s condition has changed significantly before the results become available.
These limitations have led to increased interest in point of care (POC) tests that analyse whole blood to identify coagulopathies, such as thrombelastography (TEG) and rotational thromboelastometry (ROTEM). These tests have been used for over 20 years to guide blood transfusion in liver transplantation and cardiac surgery.12–14 In TEG and ROTEM analysis, a small amount of whole blood (1 mL or less) is added to a cup with a central pin. The rotating motion of the cup in the case of TEG, or the pin in the ROTEM system, detects the increase in tension as the clot forms and gives a graphic representation of the viscoelastic changes at all stages of the developing and resolving clot. A full discussion of these tests is beyond the scope of this review and is described in detail elsewhere.13,15 TEG and ROTEM allow both the severity and prognosis to be predicted, the treatment to be tailored and the effect to be evaluated. They are also easy to use by non-trained personnel and the results are available within 10–20 min, which is much quicker than APTT or PT, leading to their use as POC bedside tests.15,16 The real-time monitoring allows for rapid clinical decision-making in the emergency settings of haemorrhage, preventing delays and enabling early tailored blood product administration. In contrast to its many advantages, limitations of TEG and ROTEM include the frequent quality control and calibration of the equipment required and the inter-rater variability which has shown variable precision between operators. 17 The role of TEG or ROTEM in managing burn injury is not well characterised, although it has the potential to be of significant use and may be superior to traditional coagulation tests because of its dynamic and quick results in the acute burn injury setting.
Objectives
This study establishes the role of different coagulation markers in burn patients and assess their potential role in diagnosing coagulopathy, tailoring blood product administration and indicating prognosis.
Methods
Aim construct
The terms of reference in Patient Intervention Comparator and Outcome (PICO) format are reported in the supplementary data (S1), conforming to pre-validated criteria. 18
Literature search
A comprehensive literature search was conducted between March and April 2017 in line with the Cochrane Handbook for Systematic Reviews of Interventions. 19 The Cochrane Library, PubMed, Scopus, Medline (OVID) and Embase (Ovid) databases were searched for articles with regards to burns, coagulation disorders and TEG and ROTEM. Primary studies of randomised controlled trials (RCTs), systematic reviews, multi-/single-centre studies, meta-analyses, case series in English and human participants over the last 13 years were included with the following Boolean and Medical Subject Headings (MeSH) ‘Burns’[MeSH] ((‘Blood coagulation disorders’[MeSH] OR rotem[TiAb]) OR ‘Blood coagulation’[MeSH]) OR ‘thromboelastography’[MeSH] (see Figure 1). Other criteria for inclusion were studies that included TEG, ROTEM, coagulation tests, and anticoagulant factors or disseminated intravascular coagulation (DIC) in burn patients. Case studies and articles only considering non-burn trauma were excluded. Finally, all results were independently screened and assessed by two researchers to identify any relevant studies for inclusion and the final set was agreed upon by serial discussion/assessment rounds for any discrepancy in selection. Cohen’s kappa coefficient was calculated at each stage of title, abstract and full text review to ascertain inter-rater variability between the two reviewers.
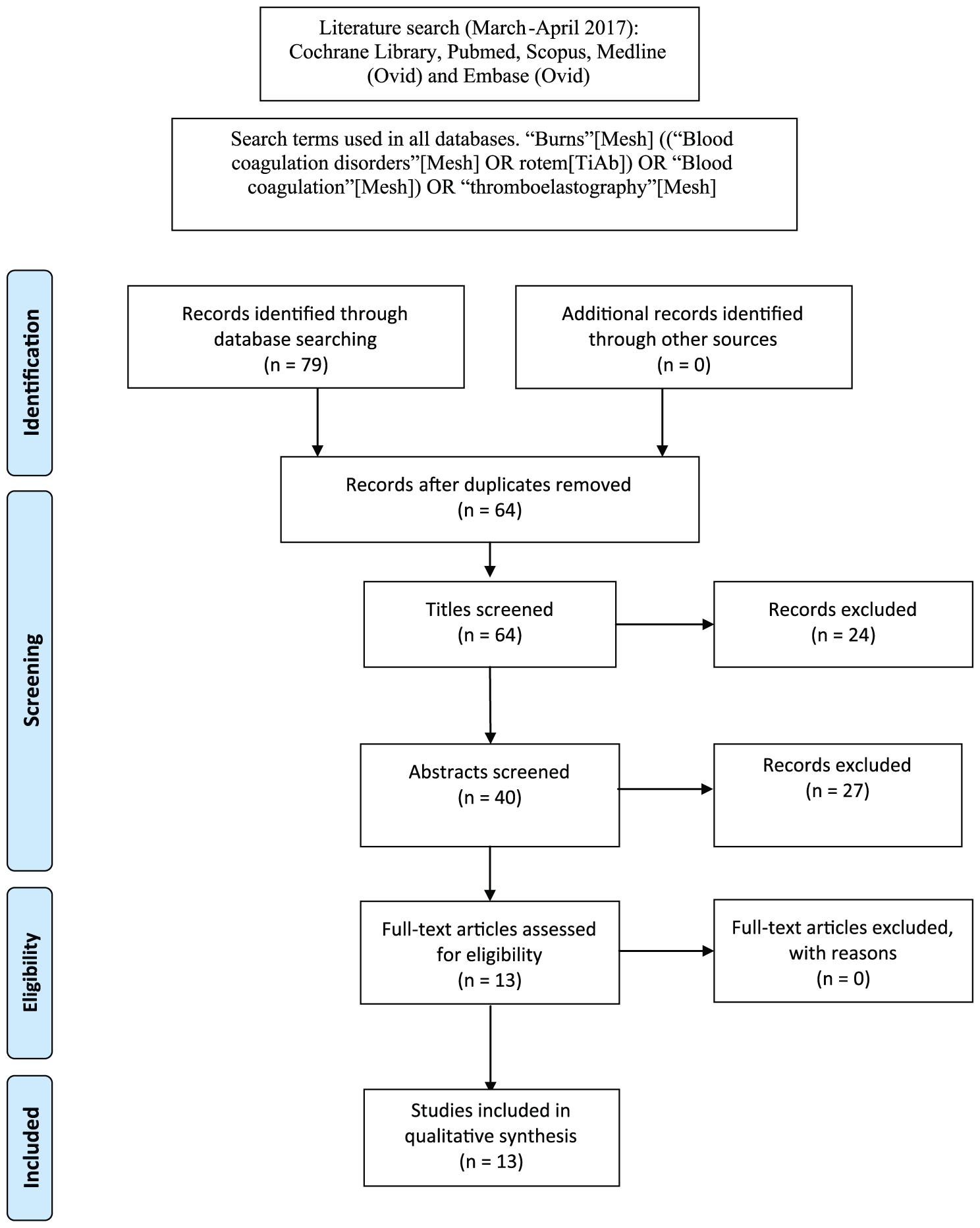
Flow chart of literature retrieval.
Reporting of the systematic review and evidence-based process
PRISMA guidelines were applied to report the systematic review and evidence-based process. The retrieval process reported only two RCTs due to the novel nature of the topic, requiring these guidelines to be adapted. Systematic review of studies other than RCTs is not new, 20 and so case series, reviews (best balance of sensitivity and specificity) and cohort studies at multi/single centres were also included. To ensure comparability, rigorous critical appraisal was applied to determine the quality of the studies retrieved and ensure inclusion of comparable, valid and relevant evidence. 21 All literature was appraised using the approved Critical Appraisal Skills Programme (CASP) framework, which assesses articles for validity, results, uncertainty and applicability to the considered population. 22
A table (Table 1) was formulated and used to extract the data from each study, including the type of study, outcome of interest, participant information, results summary, conclusion and level of evidence. The strengths and limitations of each study were discussed therein.
Summary of article findings.

ABIC: acute burn-induced coagulopathy; APC: activated protein C; APTT: activated partial thromboplastin; AT: antithrombin; ATC: acute traumatic coagulopathy; AXa: antifactor Xa; Dd: D-dimer; DIC: disseminated intravascular coagulation; DVT: deep vein thrombosis; FVIIa: factor VIIa; FVIII: factor VIII; MOFS: multi-organ failure syndrome; PAI1: plasminogen activator inhibitor 1; PC: protein C; PS: protein S; PT: prothrombin time; ROTEM: rotation thromboelastometry; TAT: thrombin/antithrombin complex; TBSA: total body surface area; TEG: thrombelastography; TPA: tissue plasminogen activator; VTE: venous thromboembolism.
Types of studies
All meta-analyses and RCTs were included. In anticipation of insufficient numbers of trials (n < 3) due to the novel nature of this topic, case series, reviews (best balance of sensitivity and specificity) and cohort studies at multi/single centres were also included.
Outcome data
Outcomes of interest were: the potential role of anticoagulant factors; coagulation markers in burn injury and any association with DIC; coagulation tests that had the potential to diagnose burn-associated coagulopathy, tailor blood product administration and provide an indication of prognosis.
Results
Search results
A total of 79 publications relating to burns and coagulation, with specific reference to the latter, were identified. Irrelevant and duplicate studies and those not fulfilling the inclusion and exclusion criteria were identified using manual checking and eliminated through serial assessment rounds by establishing inter-rater agreement (Figure 1). Thirteen full-text publications contributed to this systematic review (Table 1). Agreement between reviewers was high with Cohen’s kappa coefficient calculated as 0.74, 0.89 and 1 for the title, abstract and full-text review stages, respectively.
Participants and settings
Population
Our review included 3821 patients across 11 studies. The critical appraisal process reported two level 5,23,24 one level 4 (five patients), 25 five level 2b (205 patients),3,14,26–28 three level 3b (3550 patients)29–31 and two level 1b (61 patients)2,32 evidence studies. The RCTs were conducted in Greece 2 and Austria, 32 the cohort studies were conducted in Greece, 3 USA,14,26,28,30 UK/Spain, 29 Australia 31 and Austria, 27 the literature reviews were conducted in The Netherlands 23 and USA 24 and the case series was conducted in the USA. 25 Although there is a wide geographical variance, the coagulation markers used appear to be similar across all units.
All studies matched the participants to the criteria being evaluated. Only the two RCTs2,32 had equal representation of participant characteristics, including age, sex and severity of burns injury. The remaining eight cohort studies3,14,26–31 and one case series 25 had a higher ratio of male participants, which can reduce the generalisability of the evidence. All studies involved the adult population, except Barret et al., 29 who also included children. Van Haren et al. 28 included three patients with electrical burn injuries as part of their study population in addition to their 21 patients with thermal injuries. Park et al.14,26 used the same group of participants across two cohort studies; however, different outcomes, haemostatic status using coagulation tests 14 and coagulation and inflammatory factors, 26 were measured; therefore, both studies were included. The literature reviews included 53 24 and 92 23 journal articles, respectively, with publication dates of 1968–2015. All studies reported explicit eligibility criteria and outcomes, which would minimise confounding variables and increase applicability. However, the case series reported that patients had co-existing morbidities including hypertension and HIV; therefore, this may have confounded the results. 25
The severity of burn injury included in the studies varied between 3% 25 and 66–100% 30 TBSA. All studies consistently reported that the level of coagulopathy was proportional to the percentage of TBSA burned, although no studies specifically looked at the degree of coagulopathy in relation to burn size, which would be more useful. Park et al.14,26 failed to report the extent of burn injuries, therefore affecting the applicability of results.
Outcomes
All studies posed a clear research question and identified relevant outcomes. These included testing useful markers for the coagulation status of patients and determining the effect of these markers and their role in DIC. In addition, the haemostatic status of patients using routine laboratory tests and newer viscoelastic techniques were explored. Van Haren et al. 28 concomitantly measured both TEG and standard PT and PTT in their study population. There were no studies comparing ROTEM against standard PT and APTT tests. Furthermore, cost comparisons did not appear to be considered in any of the studies.
Randomisation and blinding
One RCT involved a treatment group, receiving antithrombin, and a non-treated control group. 2 The other RCT involved randomisation into either a case group whereby blood product use was based on a treatment algorithm using ROTEM, or into a control group with blood products being given at the discretion of the clinician. 32 Neither study described the process of randomisation, increasing the possibility of selection bias and neither study was blinded which may lead to observer bias and the possibility of a placebo effect.
Due to the nature of case series 25 and cohort studies,3,14,26–31 especially in this small, specialised group of patients, randomisation was not possible. Therefore, participants may not accurately represent the population, which reduces its validity. Participants were largely self-selected during defined dates of admission to the intensive care unit. Although difficult to blind, the case/cohort studies employed standardised methods by hospitals and clear outcomes were stated; therefore, bias was unlikely to have been introduced. It is appreciated that caution should be taken when interpreting results from case series; however, due to the limited literature, this case series 25 facilitated the publication of new observations and collectively can influence further, higher order research.
Limitations, statistical significance and quality of body of evidence
Power was not stated for any of the studies, and apart from Barret et al., 29 all studies were of small sample sizes; therefore, it is difficult to draw any definitive conclusions from their results. However, the clearly stated eligibility criteria, demographics and clinical details across all studies add strength to their conclusions and recommendations.
The reported statistically significant results included: an increase in fibrinogen 48 h following burn injury, P = 0.002; 27 reduction in blood product requirements in burn patients managed using a ROTEM-based treatment algorithm for transfusion compared to clinicians discretion (P < 0.002); 32 the improved ability to predict mortality using coagulation (maximal amplitude on TEG) and inflammatory (TNF alpha levels) parameters (P < 0.001); 26 elevated PT and APTT in burn patients when compared to controls (both P < 0.05); 14 repeat TEG samples show hypercoagulability in burn patients taken one week after admission which was more sensitive than PT and APTT measurements (P < 0.05); 28 biochemical coagulopathy on admission is an independent risk factor for 28-day mortality (P < 0.05); 31 the incidence of acute traumatic coagulopathy in burn patients on admission is significantly less than in trauma patients (P < 0.0001); 30 reduction in TPA (tissue plasminogen activator) and TAT (thrombin anti-thrombin) on day 1 compared to day 4 in patients treated with antithrombin, compared to non-treated controls, and an increase in D-dimer on day 1 compared to day 4 of injury (both P < 0.05). 2
The two literature reviews both highlighted the lack of high quality studies to base recommendations on and recommended further investigations in the area of prophylactic venous thromboembolism (VTE) treatment and hypercoagulability in burn patients 24 and coagulopathy of severe burns and its management. 23
A meta-analysis was not considered due to the variations in methodology and outcomes across all included studies which prevented direct comparison of coagulation measurements between studies to prove superiority of either.
Discussion
Coagulopathy after burn injury is influenced by a complex interplay of multiple factors and it is not always possible to predict the outcome as coagulopathy can be disproportionate to the burn injury sustained.25,30,31 Current evidence suggests that burn injury involves an uncontrolled increase in the coagulation system, in proportion to the TBSA burned.8,33 Additionally, factors contributing to a coagulopathic state include the depth of burns, inhalation injury and haemodilution in the resuscitative phase.8,31 In the early post-burn period, routine coagulation tests, PT and APTT, are not sensitive enough to detect the subtle changes in coagulation abnormalities, often only becoming abnormal once severe coagulopathies are established. 29 Several studies have found that in the majority of severe burns, PT and APTT are normal at presentation.8,30,33 However, marked changes in specific coagulation and fibrinolytic markers have been reported in the early post-burn period,3,11,12 and in one study, in the presence of normal PT and APTT. 33 The levels of coagulation-associated markers which signify a hypercoagulable state in the early post-burn period include increased fibrinogen, TAT complex, activated factor VII and decreased levels of the natural anticoagulants antithrombin III, protein C and protein S and the associated increases in markers of the fibrinolytic system include the fibrin degradation product D-dimer, TPA and TPA type 1.3,12,25,27,33 All studies reported a time course-related change in these markers, with results normalising between five and seven days unless complications developed. However, one study reported that repeat TEG measurement one week after admission showed a transition to a hypercoagulable state despite VTE thromboprophylaxis. 28
Management of severe bleeding caused by surgical debridement of wounds is known to be a clinical challenge and management can have a profound effect on patient outcome. It has been suggested that traditional plasma based coagulation tests such as PT and APTT are of limited use in managing bleeding during surgical wound debridement of burn injury.14,25,27 Instead, whole blood tests such as TEG® or ROTEM® are superior and allow for targeted therapy of blood transfusions, which has been supported by a recent RCT in burn patients. 32 Schaden et al. 32 reported a significant reduction in allogenic blood product requirements during burn excision in patients managed with an algorithm based on trauma induced coagulopathy using POC ROTEM®, compared to those managed according to clinicians discretion. Most of the available literature describe TEG®/ROTEM®’s ability to monitor and guide blood product replacement, with very little literature on its ability to detect hypercoagulable states, such as those seen in burns. Park et al. 14 reported TEG® to be more sensitive than plasma-based clotting assays (PT and APTT) in detecting hypercoagulable states in burned patients, and suggest TEG® as an additional method of assessing the efficacy of deep vein thrombosis prophylaxis in these high-risk patients. Furthermore, Van Haren et al. 28 detected a hypercoagulable state in all their patients one week after admission as measured by TEG sampling. Targeted therapy based on TEG®/ROTEM® results could improve patient outcome and allow for better allocation of healthcare resources; however, strong evidence is lacking and further research is needed to support this before clinical guidelines can be developed and implemented.
Despite several studies investigating the effect of burns on coagulation, the exact time course of these haemostatic changes remains unknown as it is effected not only by the pathophysiology of the burn, but also in response to therapeutic interventions such as fluid resuscitation, excisional surgery and transfusion. Hypothermia is a preventable problem in the early post-burn period, as a result of a combination of skin loss, hospital transfers often via air ambulance and impairment of thermoregulation with anaesthesia. Mitra et al. 8 demonstrated that hypothermia on presentation (35.5°C) was associated with early onset coagulopathy in a study of 163 patients with > 20% TBSA burns. Although hypothermia was not an in independent predictor of coagulopathy in this study, hypothermia is well known to exacerbate coagulopathy and is a cause of morbidity during burn excision surgery. 34 In a recent in vitro study of a new viscoelastic technique for clot microstructure, hypothermia was significantly associated with increased clotting times and the formation of weaker, more porous clots, prone to fibrinolysis. 35 Similar studies using this new technique have also demonstrated a significant effect of fluid haemodilution using both crystalloid and colloid fluids on coagulation in vitro. Clot strength and clot microstructure (fractal dimension) both decreased with progressive haemodilution, which became significant at dilutions as low as 20%.36,37 Higher volumes of fluid administration have been shown to be an independent predictor of early onset coagulopathy in burns (odds ratio [OR] 1.59; 95% confidence interval [CI] 1.02–9.3; P = 0.02), suggesting judicious fluid resuscitation regimes may help prevent coagulopathies in these patients. 8
Although all studies describe an increase in coagulation markers in proportion to TBSA, no papers report on the specific changes seen at different severities of burn size, which would of course be of great interest to the burns physician. One study reported a TBSA threshold whereby burns over 6% TBSA result in a hypercoagulable state; however, this was a very small study of just five patients and therefore no firm conclusion can be taken from this. 25 Both Kowal Vern et al. 11 and Garcia-Avello et al. 12 demonstrated a significant difference in coagulation markers between extensive (> 40% TBSA) and less extensive burns (< 40%TBSA) on day 1 post injury. The reason for this is most likely down to a number of factors, including a greater inflammatory reaction stimulating a more marked response by the coagulation cascade. Also, larger volumes of fluid resuscitation with larger burns will lead to a dilutional component to the alteration in coagulation markers. 11 On the other hand, Van Haren et al. 28 reported no significant difference in TEG measurements between burn patients < 50% TBSA and burns > 50% TBSA in their study. Despite the fact that both surface area and depth of burn is proportional to the severity, none of the above studies specified the depth of burn injury. This is another relevant factor to consider as ‘the volume’ of a burn can be considered.
The clinical relevance of this burns-related coagulopathy remains unknown and needs assessing via large prospective studies to assess whether this indeed has any effect on outcome in terms of wound healing and overall prognosis. Early onset coagulopathy has been shown to be associated with higher volumes of blood product replacement, prolonged mechanical ventilation and extended ICU stays; 26 however, no association with wound healing or surgical complications have been reported in any previous studies. Early onset coagulopathy has been shown to be independently predictive with increased mortality in a study by Sherren et al. 31 and the presence of overt DIC at presentation has been shown to be significantly related to organ failure and mortality (P < 0.001; OR 10; 95% CI 3.23–32.26) in two studies by Lavrentieva et al.2,3 The use of coagulation markers as a prognostic tool was suggested by Park et al. 26 who reported a scoring system to predict the probability of mortality in traumatic and burn injuries. This is currently being used at an Army Medical Centre for research purposes, but there did not appear to be any follow-up results or recommendations. Strong evidence for the role of coagulation tests as markers for prognosis and outcome are still lacking and require further research.
Strengths of this review include consistent searches of available literature across five main databases, the transparent reporting of the search strategy, articles found, and inclusion and exclusion criteria. The entire body of evidence was evaluated and graded using the well-established CASP framework 22 and Oxford Centre for Evidence-Based Medicine, 38 respectively.
Limitations of the study included the retrieval of only two RCTs requiring adaptation of our systematic review to include case series, reviews and cohort studies. The small body of evidence, sample sizes and disparate outcome measures which prevented direct comparisons proved to be a challenge in this study, which make it difficult to draw definitive conclusions.
Future work with regards to RCTs comparing burn and blood transfusion outcomes where management is based on TEG®/ROTEM® results vs. PT/APTT for comparison is advised to ascertain the usefulness of these POC tests in the burns setting.
Conclusion
This study has identified limited level 1b evidence that newer viscoelastic POC tests such as TEG and ROTEM appear to be sensitive at detecting early coagulation abnormalities. These tests could prove to be beneficial in making immediate clinical decisions regarding treatment and prognosis in burn injuries and in predicting thromboembolic events; however, even when recognised there are no current guidelines for the management of burn-related coagulopathies. Further research in the form of a well-designed large multicentre RCT investigating the accuracy of routine laboratory and newer viscoelastic tests in diagnosing post-burn coagulation disorders is required before definitive recommendations can be produced.
Footnotes
Acknowledgements
We would like to thank Morriston Hospital Library Services for their help in the initial literature search and retrieval of full-text articles.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.