
Abstract
Background:
Keloid disease (KD) is common and often refractory to treatment. Definition of the genetic mechanisms of KD can lead to a better understanding of the disease and suggest more effective treatment strategies.
Objectives:
To quantitatively estimate the association between KD susceptibility and the -509C/T polymorphism in the TGF-β1 gene.
Methods:
PubMed, Embase and CNKI databases were searched using a combination of the Medical Subject Headings (MeSH) and relevant words in titles. Analyses were performed with STATA 12.0.
Results:
Five case-control studies encompassing a total of 564 keloid cases and 620 healthy controls were pooled in the final meta-analysis. Among the five studies, no significant association was detected between the TGF-β1 -509C/T polymorphism and KD under all of the five genetic models (allele comparison, heterozygote comparison, homozygote comparison, dominant model and recessive model) for the overall analyses and for the subgroup analyses based on DNA extraction method, participant ethnicity and group size. When stratified by study quality, three high-quality studies showed significant association under allele comparison and homozygote model (C versus T: OR = 0.80, 95% confidence interval [CI] = 0.65–0.98, P = 0.03; I2 = 0%, P = 0.64; CC versus TT: OR = 0.62, 95% CI = 0.41–0.94, P = 0.02; I2 = 0%, P = 0.79); while two moderate-quality studies showed significant association under allele comparison, homozygote model and recessive model (C versus T: OR = 1.52, 95% CI = 1.15–2.01, P = 0.004; I2 = 39%, P = 0.20; CC versus TT: OR = 2.14, 95% CI = 1.24–3.70, P = 0.02; I2 = 19%, P = 0.27; CC versus CT+TT: OR = 2.04, 95% CI = 1.29–3.24, P = 0.002; I2 = 0%, P = 0.35).
Conclusions:
The current meta-analysis suggests that the TGF-β1 -509C/T polymorphism is not associated with KD susceptibility. High-quality and large-scale studies are needed to validate our findings.
Lay summary
Keloid scars are thick and lumpy scars that behave almost like tumours. They grow, are unsightly and itchy, and difficult to treat as they can get worse after attempts at treating them. This article reviews the scientific evidence for a link between a certain gene variation, specifically `509C/T polymorphism in the TGF-β1 gene’. After an extensive scientific database search, five studies were found, and no significant association was detected between the TGF-β1 -509C/T polymorphism and Keloid scarring. High quality and large-scale studies are needed to validate our findings.
Keywords
Introduction
Keloid disease (KD) is an aggressively raised dermal lesion resulting from abnormal wound healing processes following skin trauma, surgery, burn injury, vaccination and even acne. Unlike hypertrophic scars, in which the raised dermal lesion stay within the confines of the initial wound, keloid scars grow beyond the margin of the original wound. 1 The exact aetiology of KD is still unknown. In the general population, the incidence of KD was reported to be 4–6%, while in different ethnically defined patient populations it reached up to 20%. 2 Familial inheritance, parallelism in twins and mutation in certain genes or chromosomal regions such as p53, TGF-β, SMAD, HLA, 2q23, 18q21.1 and 19q13.1 are suggested to be risk factors to the development of KD. 3
Pathological findings of KD include over proliferation of fibroblasts, excessive deposition of collagen, elastin and proteoglycans in the extracellular matrix (ECM). Fibroblast dysfunction has been commonly thought to contribute to the pathogenesis of KD. 4 Transforming growth factor-beta (TGF-β) family members play an important role in cell proliferation, apoptosis and differentiation. In particular, TGF-β1, a cytokine encoded by the TGF-β1 gene located on chromosome 19q13.1, is one of the most frequently studied among many cytokines which may be responsible for KD formation.5,6 Studies have shown that keloid-derived fibroblasts demonstrated over-production of TGF-β1 compared with fibroblasts isolated from normal wound tissue.7,8
TGF-β1 plays such a key role in the biological function of fibroblasts that any irregularity of this cytokine caused by gene polymorphism or mutation at gene level may lead to the development of KD. There are several polymorphisms in the TGF-β1 gene like -988C/A, -800G/A and -509C/T in the promoter region, Arg25Pro and Leu10Pro in exon 1 and Thr263Ile in exon 5.9,10 Among them, -509C/T of TGF-β1, which is also designated as rs1800469, has been confirmed to influence the transitional activity of TGF-β1. Currently, many studies have been conducted to investigate the association between the -509C/T polymorphism in the TGF-β1 gene and susceptibility to KD, but the results remain inconsistent. The object of the present study is to combine those relevant studies published to date and assess the relationship between KD susceptibility and the -509C/T polymorphism in the TGF-β1 gene.
Methods
Literature search
A relevant literature search was performed according to the PRISMA (Preferred Reporting Items for Systematic reviews and Meta-analysis) guidelines. 11 The PubMed, Embase and CNKI databases were searched using a combination of the Medical Subject Headings (MeSH) and relevant words in the title. The MeSH used were ‘Keloid’ and ‘Transforming growth factor beta1’ and ‘Polymorphism, Single Nucleotide’. The relevant words in the title included ‘keloid’, ‘keloids’, ‘transforming growth factor’, ‘TGF-beta1’, ‘TGF-β1’, ‘polymorphism’, ‘association’ and ‘genetic’. Additional studies were acquired through a hand search of the reference lists of related articles and existing reviews. The search was performed in February 2017 and no limit was applied to the study language. All retrieved records were added to an EndNote (Version X5, Thomson Reuters, New York, NY, USA) library.
Study selection
Studies were included in our meta-analysis if they met the following criteria: (1) original research study, i.e. not a review or a comment; (2) case-control study including KD cases and healthy controls; (3) studies that assessed the relationship between KD susceptibility and the 509C/T polymorphism in the TGF-β1 gene; (4) healthy controls were in Hard–Weinberg equilibrium (HWE); and (5) data of allele frequency and genotype frequency were sufficient for meta-analysis. Studies were excluded if they were: (1) reviews, letters, case reports, editorials, comments, studies on animals or cells; (2) studies without healthy controls; (3) healthy controls were not in HWE; and (4) studies without sufficient allele and genotype data for extraction.
Data extraction
The following information was extracted: first author, year of publication, study design, number of cases and controls, DNA extraction method, allele frequency, genotype frequency, HWE for healthy controls. Two reviewers independently proceeded the data extraction and inconsistency was resolved following a discussion.
Quality assessment
The quality assessment of the finally included studies was assessed by two reviewers independently based on the Newcastle–Ottawa scale (NOS) quality scoring system. This quality score system includes three broad perspectives: ‘Selection’, ‘Comparability’ and ‘Exposure’. The overall scores are in the range of 0–9 and studies with scores of 0–3, 4–6 and 7–9 are identified as being of a low, moderate and high quality, respectively. Any inconsistency of quality assessment was resolved by discussion and consultation with a third reviewer.
Data analysis
Odds ratio (OR) and 95% confidence interval (CI) were calculated to evaluate the association between KD susceptibility and the -509C/T polymorphism in the TGF-β1 gene. The Chi-squared test was used for quantification of statistical inconsistency between studies and I2 values showed the degree of heterogeneity. Data with significant heterogeneity (P ⩽ 0.1 and I2 ⩾ 50%) were combined using a random effects model, while data without significant heterogeneity (P > 0.1 and I2 < 50%) were combined using a fixed effects model. The differences between subgroups were further tested, and a value of P < 0.05 was considered statistically significant. The following five genetic models were applied for meta-analysis of the TGF-β1 -509C/T polymorphism: allele comparison (C versus T); heterozygote comparison (CT versus TT); homozygote comparison (CC versus TT); the dominant model (CC+CT versus TT); and the recessive model (CC versus CT+TT). The Chi-squared test was used to evaluate the HWE for healthy controls. Subgroup analyses were conducted based on DNA extraction method, participant race, NOS score and study size. Egger’s linear regression test were used to assess the publication bias. Analyses were performed with STATA 12.0.
Results
Literature search
A total of 19 studies were originally retrieved through database search and two studies were acquired through cross-reference search. Eighteen studies remained after the removal of duplicates. Twelve studies, including non-genetic studies, experimental studies on cells and studies not about the TGF-β1 -509C/T polymorphism, were excluded. Full texts of the remaining six studies were then reviewed for eligibility. One study was further excluded because of imprecise definition of KD in the study. As a result, five studies were pooled in the overall analysis. The process of study selection and the reasons for exclusion are shown in Figure 1.

Process of study selection and the reasons for exclusion.
Study characteristics
A total of 564 keloid cases and 620 healthy controls were included in the five case-control studies.10,12–15 The publishing years ranged from 2003 to 2015. Two of the five studies were conducted in Chinese populations and the remaining three studies were conducted in Caucasian, Malay and Polish populations, respectively. All studies involved case groups and control groups. All control groups of the five studies fulfilled the HWE. Polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) was used in all five studies to identify the -509C/T polymorphism of TGF-β1. The scores of NOS were in the range of 5–8. Three studies were identified as being of a high quality and two studies were identified as being of a moderate quality. The characteristics and methodological quality of the five included studies are shown in Table 1. The risk allele and genotype frequency are shown in Table 2.
Characteristics and methodological quality.

CC, community control; HC, hospital control; PCR-RFLP, polymerase chain reaction-restriction fragment length polymorphism SNP, single nucleotide polymorphism.
Allele and genotype frequency.

HWE, Hardy–Weinberg equilibrium.
Overall and subgroup meta-analyses
The results of overall and subgroup meta-analyses were summarised in Table 3. For the overall analysis, no significant association was detected between the TGF-β1 -509C/T polymorphism and KD under all five genetic models. Significant heterogeneity was found under three genetic models (allele comparison: C versus T; homozygote model: CC versus TT; recessive model: CC versus CT+TT), while homogeneity was found under two genetic models (heterozygote model: CT versus TT; dominant model: CC+CT versus TT).
Overall and subgroup meta-analyses.
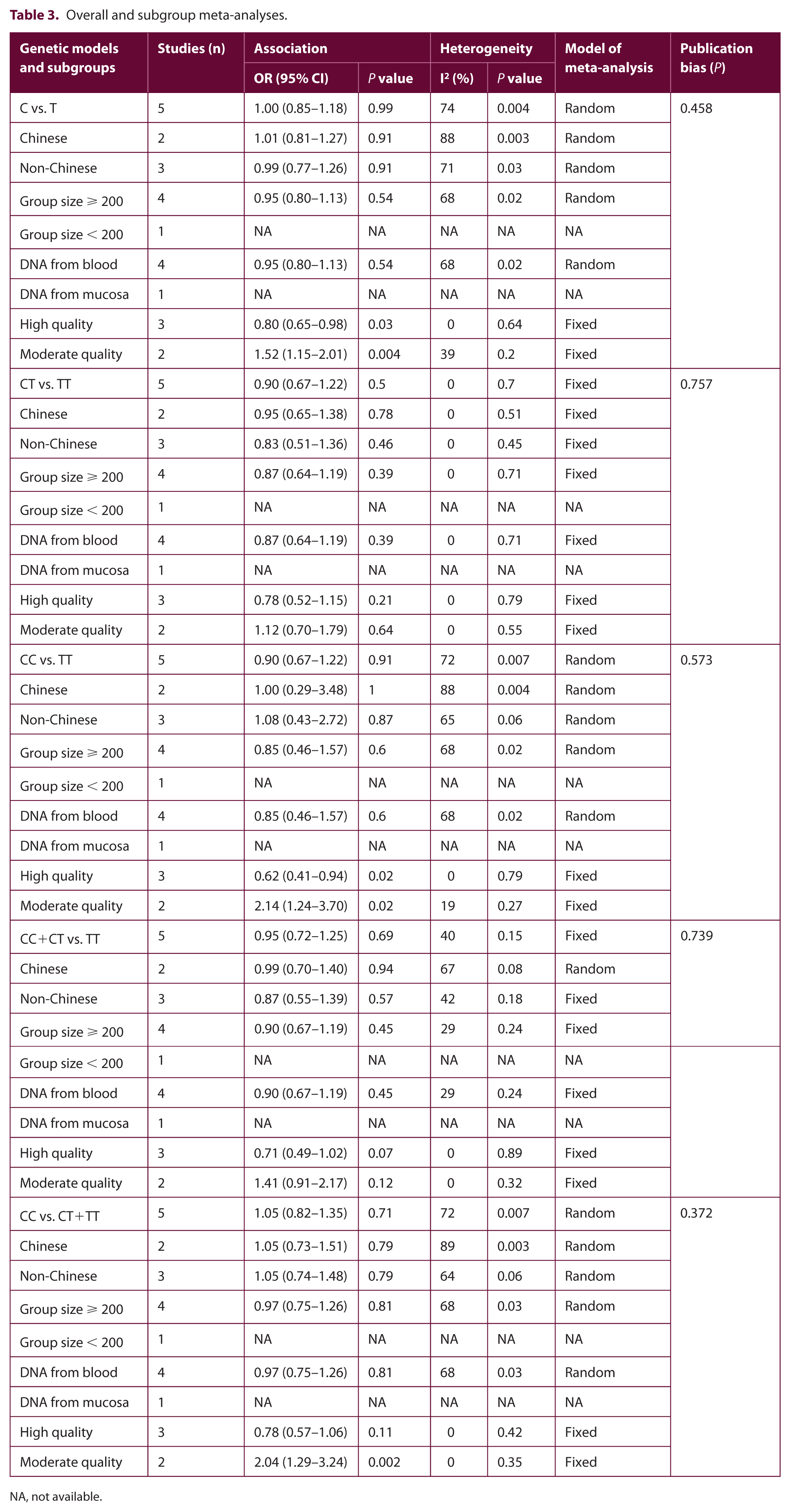
NA, not available.
When stratified by DNA extraction method, participant ethnicity and group size, no significant association was detected between the TGF-β1 -509C/T polymorphism and KD under all five genetic models in any one of the subgroups. When stratified by study quality based on NOS scores, in studies being identified as high quality, significant association was found under allele comparison and homozygote model (C versus T: OR = 0.80, 95% CI = 0.65–0.98, P = 0.03; I2 = 0%, P = 0.64; CC versus TT: OR = 0.62, 95% CI = 0.41–0.94, P = 0.02; I2 = 0%, P = 0.79) (Figures 2 and 3); while in studies being identified as moderate quality, significant association was found under allele comparison, homozygote model and recessive model (C versus T: OR = 1.52, 95% CI = 1.15–2.01, P = 0.004; I2 = 39%, P = 0.20; CC versus TT: OR = 2.14, 95% CI = 1.24–3.70, P = 0.02; I2 = 19%, P = 0.27; CC versus CT+TT: OR = 2.04, 95% CI = 1.29–3.24, P = 0.002; I2 = 0%, P = 0.35) (Figures 2–4).
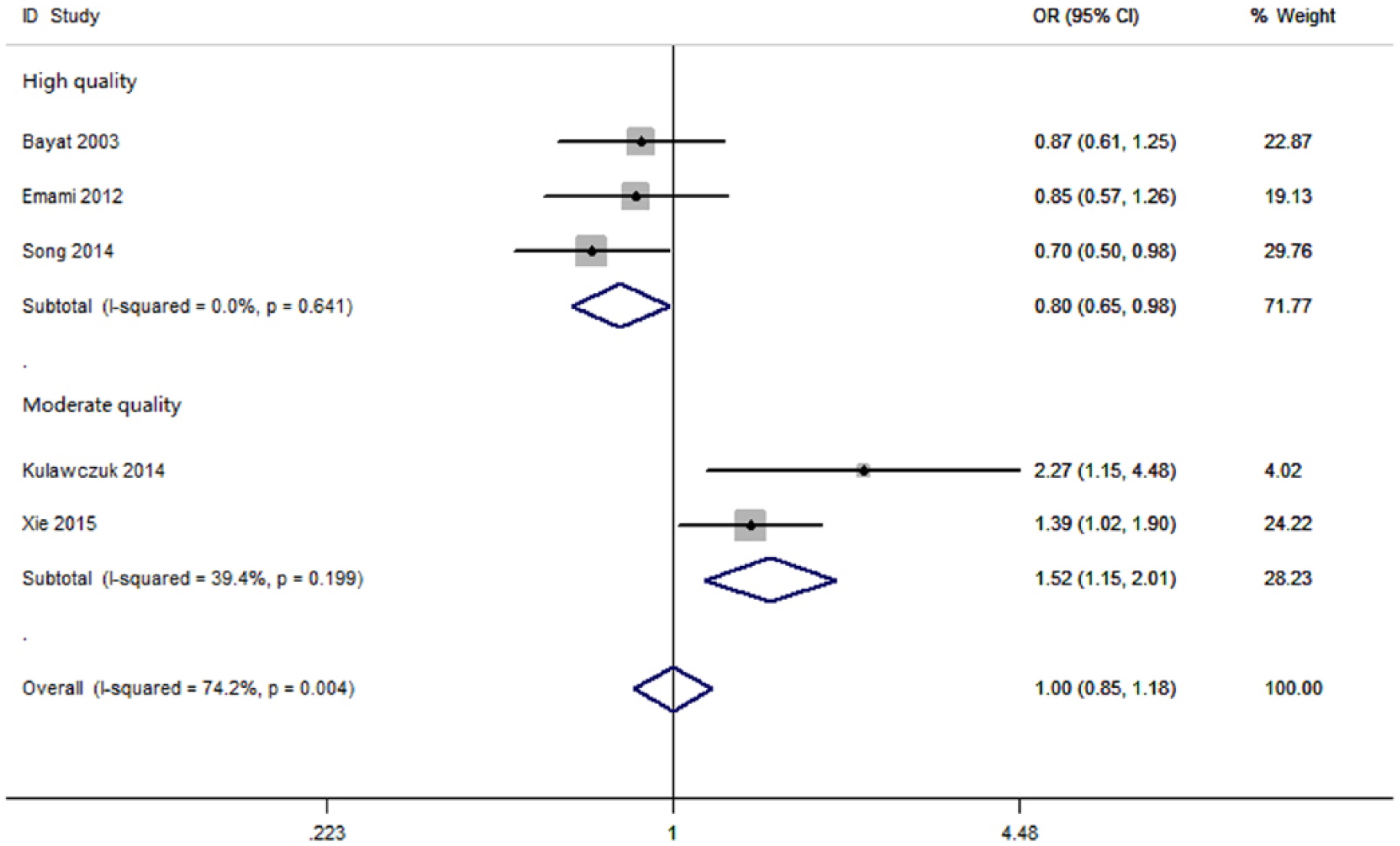
Subgroup analyses based on study quality under allele comparison (C vs. T).

Subgroup analyses based on study quality under homozygote model (CC vs. TT).

Subgroup analyses based on study quality under recessive model (CC vs. CT+TT).
Meta-regression
As shown in Table 4, results from meta-regression indicated that study quality based on NOS was considered as the source of heterogeneity under allele comparison, homozygote model and recessive model (C versus T: P = 0.037; CC versus TT: P = 0.039; CC versus CT+TT: P = 0.042).
Meta-regression analyses (P value).

Publication bias
Publication bias was evaluated using Egger’s linear regression. No significant publication bias was detected under all five genetic models, as shown in Table 3.
Discussion
There is much speculation regarding a genetic basis of KD. Autosomal recessive expression was reported by Omo-Dare, 16 while in the studies of Bloom, Marneros et al., Chen et al. and Clark et al., autosomal dominant expression was suggested.17–20 Studies have shown that a positive family history of KD may contribute to the development of multiple-site keloids or more severe forms of keloids. 21 Mutations or polymorphisms of genes or chromosomal regions that may be associated with the susceptibility to KD have been widely investigated.22–26 However, several limitations existed in those genetic studies. First, many of those studies were case reports, letters or correspondence. Small group sizes or lack of healthy controls made the data of allele and genotype insufficient for pooled analysis. The occurrence of KD is often associated with other genetic disorders and no standard criteria were applied for the inclusion of individuals with KD in those genetic studies. Moreover, those genes selected for mutation or polymorphism study were so scattered and not systemised that it was difficult to draw conclusions about the genetics of KD.
Pathologically, different kinds of scars can be formed after dermal injuries, such as scarless fetal wound healing, linear scars, stretched scars, scar contractures, atrophic scars, hypertrophic scars and keloids. 27 A normal wound-healing process is composed of three distinct yet overlapping phases: inflammatory phase; proliferative phase; and scar maturation phase. 28 Keloids form as a result of an abnormal wound-healing process and grow beyond the boundaries of the original wound. 29 Studies have shown that excessive deposition of ECM components during the scar maturation phase is a key feature of KD. 4 Identifying the genetic predisposition that closely correlated to abnormalities of ECM components would help to elucidate the mechanisms underlying the development of KD.
It is well-known that the TGF-β family plays an important role in the process of wound healing via its multi-directional regulation of ECM synthesis. 5 Many genetic studies have been conducted to investigate the mutations or polymorphisms in the TGF-β1 gene that may be responsible for the development of KD. Bayat et al. conducted a case-control study to investigate the association of five known single nucleotide polymorphisms (SNP) of TGF-β1 (codons 10, 25, 263 and -800G/A, -509C/T) and susceptibility to KD. No statistical significance for both alleles and genotypes of those TGF-β1 SNP were found in their study. 10 Emami et al. also found no statistically significant difference in both allele and genotype frequency distributions between KD patients and healthy controls for c.29T/C and -509C/T of TGF-β1 in a Malay population. 12 However, Kulawczuk et al. found in their study that the presence of allele T (i.e. CT or TT genotype) of TGF-β1 -509C/T was related to a significantly lower risk of KD in a Polish population (OR = 0.321, 95% CI = 0.119–0.870, P = 0.03). 13 There were two studies on the relationship between the TGF-β1 -509C/T polymorphism and susceptibility to KD in a Chinese population. Song et al. found that Chinese individuals with allele C (i.e. CT or CC genotype) of TGF-β1 -509C/T had a significantly higher risk of developing KD (OR = 1.421, 95% CI = 1.109–1.983, P < 0.05). 14 Slightly different from that, Xie et al. suggested that CC genotype of TGF-β1 -509C/T significantly increased the risk for the development of KD in Chinese population (OR = 1.818, 95% CI = 1.077–3.070, P < 0.05). 15 As above, the results of these genetic studies of the TGF-β1 -509C/T polymorphism in KD remain inconsistent.
Our current meta-analysis of five studies showed that the TGF-β1 -509C/T polymorphism was not associated with the susceptibility to KD. Meta-regression was used to explore the source of heterogeneity under three of the five genetic models (allele comparison: C versus T; homozygote model: CC versus TT; recessive model: CC versus CT+TT) and it was found that the study quality might be the effect modifiers for heterogeneity under the three genetic models. Stratified analyses based on study quality lowered the heterogeneity. Among the three studies being identified as high quality, significant association was found under allele comparison and homozygote model (C versus T: OR = 0.80, 95% CI = 0.65–0.98, P = 0.03; I2 = 0%, P = 0.64; CC versus TT: OR = 0.62, 95% CI = 0.41–0.94, P = 0.02; I2 = 0%, P = 0.79) between individuals with KD and healthy controls. Among the two studies being identified as moderate quality, we found that in the study by Kulawczuk et al., patients enrolled in their case group and control group both suffered from cardiac diseases and consequently underwent cardiac surgery. 13 Likewise, in the study by Xie et al., the individuals in their control group were those patients with healthy scars after surgery. 14 The potential selection biases for cases or controls in the two studies lowered the final scores of NOS. Although significant association was found under allele comparison, homozygote model and recessive model (C versus T: OR = 1.52, 95% CI = 1.15–2.01, P = 0.004; I2 = 39%, P = 0.20; CC versus TT: OR = 2.27, 95% CI = 1.12–4.58, P = 0.02; I2 = 19%, P = 0.27; CC versus CT+TT: OR = 2.04, 95% CI = 1.29–3.24, P = 0.002; I2 = 0%, P = 0.35) in the two studies without significant heterogeneity, showing an OR opposite to that of high-quality studies, we assumed it to be practically meaningless due to unknown geographic differences or co-morbidity-related genetic background differences that could not be evaluated in the meta-analyses.
The current meta-analysis, however, has some limitations. For instance, only five studies were finally included for the pooled analysis. Two studies were conducted in Chinese populations and the three other studies were conducted in Caucasian, Malay and Polish populations, respectively. It was quite insufficient for the subgroup analysis based on ethnicity. Although publication bias was not observed among the five studies, limited numbers of enrolled studies weakened the strength of statistical evidence. Moreover, opposite results of OR were observed among high-quality studies and moderate-quality studies. Apparently, it could not be merely explained by the selection biases for cases and controls in moderate-quality studies.
In conclusion, the current meta-analysis suggests that the TGF-β1 -509C/T polymorphism is not associated with KD susceptibility. High-quality and large-scale studies are needed to validate our findings.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.