
Abstract

Introduction:
Heterotopic ossification (HO) is the formation of lamellar bone within connective and other tissue where bone should not form and is a rare complication after burn injury. However, it leads to severe pain and distress, marked reduction in joint range of motion (ROM), impaired function and increased hospital length of stay. The pathophysiology, incidence and risk factors of HO remain poorly understood in burns and other traumas and the management, controversial. The aim of this comprehensive review, therefore, was to synthesise the available evidence on the development and treatment of HO after acute burn injury.
Methods:
The review was based on a systematic search of five electronic databases PubMed, EMBASE, CINAHL, LILACS and Scopus.
Results:
Synthesis and analysis of the data highlighted that, despite the passage of time, little translatable evidence is available to guide any prevention, screening, diagnostic or pharmacological or physical management protocols.
Discussion:
Causes of HO remain confounded, therefore prevention is difficult. Although spontaneous resolution is possible, surgical resection remains the recommended treatment when ROM and activities of daily living are severely affected.
Conclusion:
The findings from this review indicate that multicentre data pooling is needed to understand the optimum pathway to prevention, identification and treatment of HO in acute burn patients.
Lay Summary
Background to this subject:
Heterotopic ossification (HO) is the formation of bone within the tissue where bone should not form and is a rare complication after burn injury. However, it leads to severe pain and distress, marked reduction in joint range of motion (ROM), impaired function and increased hospital length of stay. The pathophysiology, incidence and risk factors of HO remain poorly understood in burns and other traumas and the management, controversial.
Question being asked or issue explored:
The aim of this comprehensive review was to synthesise the available evidence on the development and treatment of HO after acute burn injury.
Details of how the work was conducted:
The review was based on a systematic search of medical electronic databases to identify relevant published literature.
What we did and did not learn from this study:
Synthesis and analysis of the data highlighted that, despite the passage of time, little translatable evidence is available to guide any prevention, screening, diagnostic or pharmacological or physical management protocols. Causes of HO remain confounded, therefore prevention is difficult. Although spontaneous resolution is possible, surgical resection remains the recommended treatment when ROM and activities of daily living are severely affected. The findings from this review indicate that multicentre data pooling is needed to understand the optimum pathway to prevention, identification and treatment of HO in acute burn patients.
Keywords
Introduction
Heterotopic ossification (HO) is a relatively rare complication after burn injury. However, it remains a problematic issue for burn survivors as it causes significant long-term disorders including reduced range of movement (ROM) and function, 1 extreme pain, 2 and nerve entrapment. 3 The etymologic roots of the term HO derive from Greek origins, heteros topos, meaning different place and the Latin ossificatio, meaning bone formation. Therefore, the literal translation is ‘bone formation in another place’. 4 HO is the development of lamellar bone in non-osseous soft tissue. 4 It is reported to develop in those with genetic disorders, orthopaedic trauma, traumatic brain and spinal cord injury (SCI), electrocution and burn injuries.5,6 Therefore, it is not surprising that the incidence of HO in military patients is reported to be higher than that in civilians 7 and polytrauma. 4
Initially described in children in 1692 by Patin, 8 HO was first reported within the burns literature in 1957. 9 The prevalence of HO was reported prior to the1990s as 1.2% but is in the range of 0.2–4%1,10–12 with the incidence increasing in larger mean total body surface area (TBSA) cohorts with increasing survival. 13 However, both Orchard et al. 14 and Hunt et al. 15 highlight discrepancies in the prevalence of HO in burns, with those from a retrospective design demonstrating a lower incidence and a prospective design reporting a significantly higher incidence of HO. By far the most common sites affected are the elbows resulting in marked reduction in ROM and function, often associated with ulnar nerve compression. 10 Involvement of other joints including shoulders, hips, knees, forearms 15 and the tempromandibular joints (TMJ) 16 have been documented.
Due to the challenge of studying mechanistic pathways with such a low incidence problem in humans, our knowledge of the pathophysiology of HO is primarily informed by animal studies and observations of other patient populations with a relatively greater incidence (orthopaedic, traumatic brain and SCI). 17 The cellular pathways that are most implicated in the formation of pathological ectopic tissue, and the definitive mechanism driving HO deposition, have not yet been established. 18 Current understanding of the pathophysiology of HO implicates the inflammatory process and systemic responses to trauma as contributors to HO, particularly in burns. 17 Burn injury initiates the primary component identified for HO formation: the inflammatory and immune cascade. Inflammation in the affected tissue attracts myeloid cells and lymphocytes that catalyse the release of cytokines. 17 In their study of hip arthroplasty patients, Amar et al. 18 proposed that the cells responsible for triggering HO development were the mesenchymal stem cells (MSC). Bone morphogenic protein 2 (BMP2) released due to tissue trauma mediates an increase in inflammatory markers, substance P (SP) and calcitonin gene-related protein and causes MSC migration and response to unknown stimuli which in turn results in anomalous differentiation. 18 The recruitment of immune cells provokes local tissue disturbance and results in inflammatory signals that are proposed to increase osteogenic differentiation of MSCs, potentially resulting in heterotopic bone deposition. 18 The disease may include pericapsular calcification, predominantly overlying tendons and in the planes of ligaments. New bone formation may also include osteophyte formation adjacent to joints, periosteal new bone formation and intra-articular or extra-articular ankyloses. 19 Presumably due to the lack of clarity about the pathophysiology of HO in burn patients, treatment options and timing are also a controversial area.20,21 Given the impact that HO has on burn survivors, their families and health professionals, burns and rehabilitation clinicians including surgeons, intensivists nurses, allied health professionals, social workers/psychologists/psychiatrists and rehabilitation specialists need to collectively address these significant issues of HO. Furthermore, other professionals such as bio-engineers and bio-scientists, also need to collectively collaborate in an attempt to understand the pathophysiology of this condition. Therefore, the purpose of this comprehensive review was to critically appraise and synthesise the available literature on the development, treatment and impact of HO in burn survivors.
Methods
A systematic and rigorous search across the electronic health databases PubMed, EMBASE, CINAHL, LILACS and Scopus was conducted in May 2016. The databases utilised encompass a wide-ranging and multidisciplinary span of research across the healthcare domain. Boolean connectors AND, OR and NOT were used to combine search/MeSH terms and keywords including burn*, thermal injury, heterotopic ossification, HO. The reference lists of all included papers were examined to identify any potential papers not captured through the initial search strategy and full text articles were retrieved when possible.
Inclusion and exclusion criteria
The search criteria for this comprehensive review incorporated peer-reviewed primary research published in English that identified the development and treatment of HO. No parameters concerning year of publication were imposed so as to capture the depth and breadth of data. Animal studies, reviews, conference proceedings and editorials were excluded. Higher level evidence was summarised and synthesised. In the absence of higher level evidence, case studies and case series were included.
Data evaluation and extraction
A total of 415 references were downloaded into EndNote X8. After duplicates were removed, the search strategy identified 180 prospective papers (Figure 1). Authors EO and RK identified 32 potential papers through the evaluation of titles and abstracts. A further study was identified via searching the reference lists of included papers. Based on the inclusion criteria, authors RK, DV and EO independently reviewed the relevant papers. Any disparities were determined by collaborative discussion until consensus was reached. Through this systematic and rigorous process, three studies were subsequently removed. Authors DE and NF reviewed the included studies and assimilated the ‘Results’, ‘Discussion’ and ‘Conclusion’.
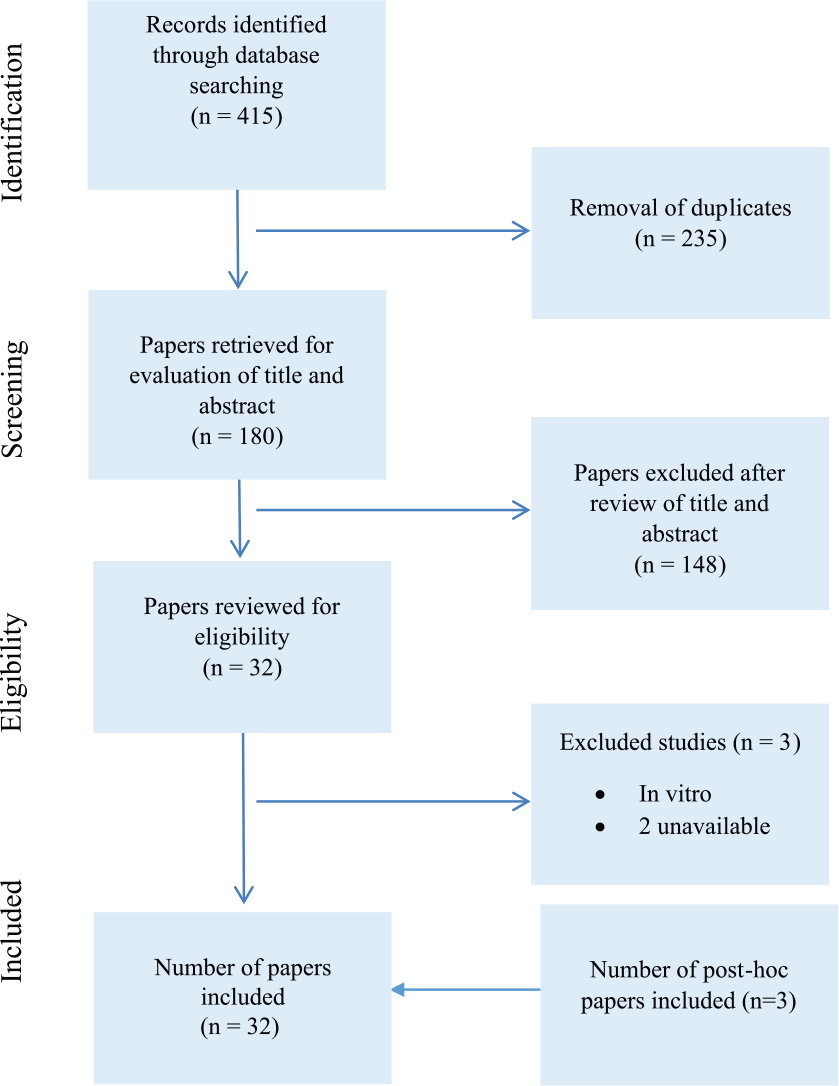
Decision trail of included studies.
A total of 32 papers were systematically summarised and synthesised. Findings from the studies were analysed and developed into key domains as to enable the recognition of recurring relationships across data. Data extracted included author(s), year of publication, country of origin, design, purpose of study, sample and study population, data collection and analysis and significant findings/outcomes (Table 1), and case series and reports were tabled separately (Table 2).
Summary of included studies.

Available case reports and case series of HO in burns trauma.

Results and discussion
Study report and pooled sample characteristics
The clinical sample amassed in this comprehensive review included 545 burns patients diagnosed with HO of which the majority were men. Of the 32 studies, 14 were retrospective cohort, 14 were case series or case reports, two case control studies, one prospective study and one registry-based study were included in the review. This comprehensive review did not identify any meta-analyses or randomised control trials. Thus, the evidence available regarding HO in burns was low (level III–IV) with only one study, comparing HO excision surgery outcomes, identified at level II.
Studies captured spanned four decades from 1972 to 2015, with nine studies and five case reports documented in the last 16 years and nine studies and nine case reports prior to the year 2000 emphasising the dearth of literature in the domain of HO and humans with burn trauma. Excluding the case reports, the pooled study sample of 412 patients (82% men) had a mean age of 37 years (age range, 8–62) and mean TBSA of 48% (range, 8–95%) (Table 3). The studies had a range of 7–98 participants. Studies mainly emanated from the USA; however, other study reports arose from Israel, Canada, South Africa, Australia, New Zealand, France, Germany, Spain, India, and China and Taiwan (Table 1). The included studies did not consistently report all required data, including mean values and standard deviations, gender of subjects and the size of the sample population, limiting the ability to pool data.
Summary of descriptive studies.
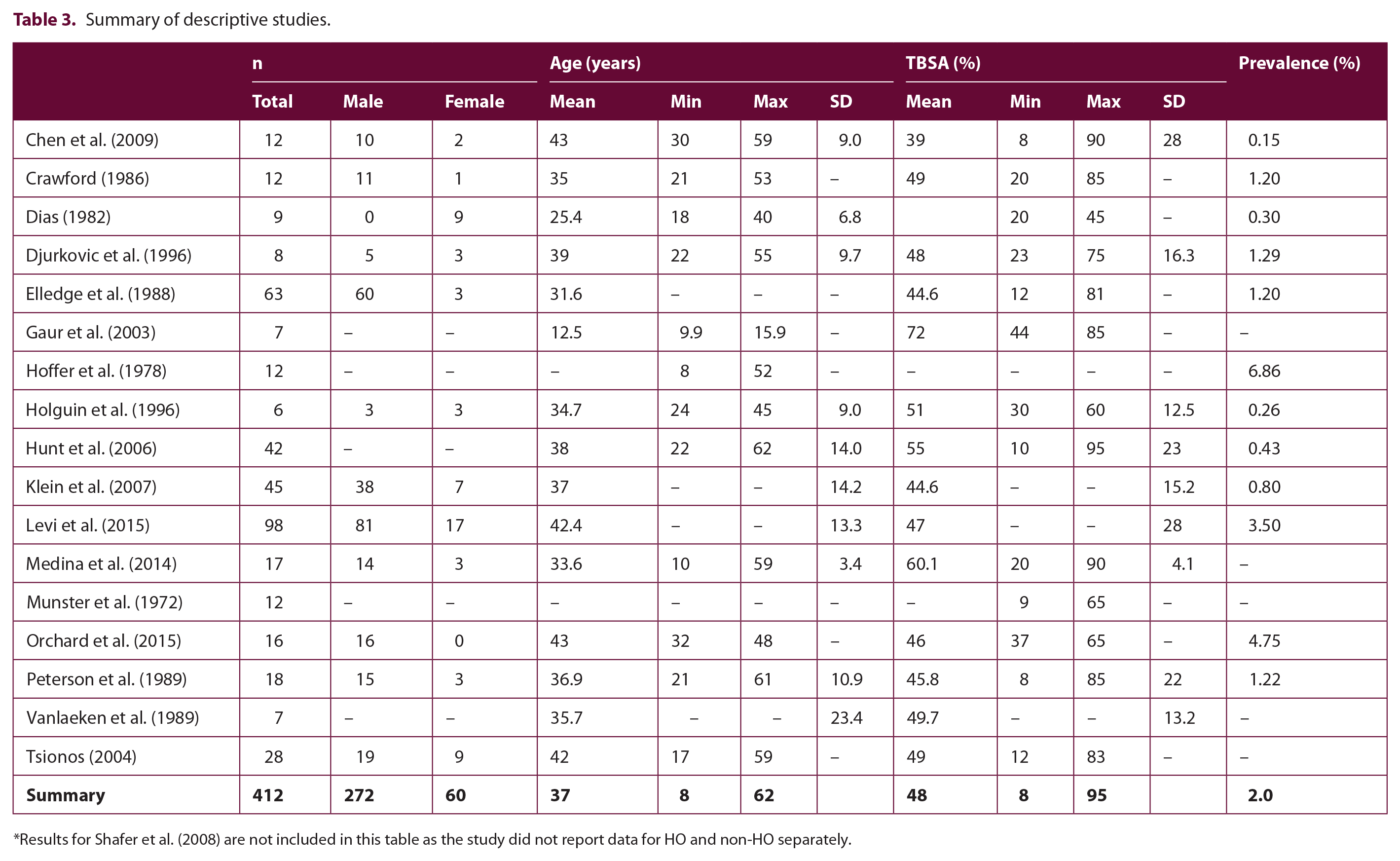
Results for Shafer et al. (2008) are not included in this table as the study did not report data for HO and non-HO separately.
While the case series and reports described in more detail the burn patient with HO, 18 studies investigated several domains including pathogenesis of HO, incidence and risk factors in the formation of HO, diagnosis, therapeutic management, surgical outcomes and function post removal of HO and delayed wound closure and HO formation.
Case series and reports
Case series/reports allow the identification of rare clinical conditions and provide a thorough review on important topics. 22 Of the 14 case series and reports included in this review (Table 2), ten were single-participant case reports and four were case series with two to four participants. Patients represented in the case series/reports were predominately men with only one woman identified. In contrast to the group-wise data, the case reports included a child of 12 months and an older adult of 68 years. As a cohort, the case report patients remained within the same TBSA range (30–86%) and depth of burn as in the pooled sample. The case reports identified the elbow as the most commonly involved joint but also described diagnosed HO in shoulders, knees, hips, hands, temporomandibular joint and more obscure areas such as the chin and vocal cords. Pre-surgical complications included significantly limited ROM, pain and one case of ulnar nerve entrapment. ICU admission was stated in six reports with three involving ventilation and three reporting sepsis. However, despite the depth and the size of the burn, ICU was not stated in several reports which may indicate omissions in reporting. Serum alkaline phosphate was reported within normal limits in some reports and elevated in others. Confirmed diagnosis of HO, in 1–4.5 months, was established by X-ray, bone scan and CT. Surgical intervention was described in seven of the reports with physiotherapy active and passive movement and static splinting the most common postoperative regime. Time to follow-up was in the range of 4 months–4 years in the cases where this was reported. Studies reported post-intervention ROM ranged from no improvement to the return of full ROM.
Risk factors for the development of HO
The studies identified an HO incidence in the range of 0.15–4.7% but repeatedly noted as 1.2% before 200023–26 and ≥ 3.5% in later years.6,17 The overall prevalence from the pooled sample was 2.0% (Table 3). The reviewed literature consistently identified severity of injury as a risk factor with the most strongly implicated markers being: TBSA (13% increase risk per % surface area); full thickness or deep dermal burn; ICU stay and/or mechanical ventilation; and inhalation injury. In more recent studies with enhanced statistical analysis methods, greater risk of HO was associated with: increased time to wound closure (8% increased risk per day); delayed grafting; and number of surgical episodes. These factors interact with delayed time to commencing physiotherapy and active ROM, immobilisation timeframes and contracture which have also been implicated in recent studies. There were exceptions to these high-risk categories. For instance, HO was reported in non-burned elbows. 28 Schneider et al., 17 using data from the same database as the Levi et al. 12 study, established a validated risk-scoring system for HO. Location of grafts and percentage of TBSA were found to impact HO risk while other variables were not found to increase the risk of HO. 17 The percentage of TBSA had the greatest impact on HO risk in this study with an increase of 10% in TBSA providing an increase of 1 point in their risk scale. Furthermore, graft location at the arm, head/neck or trunk providing 1 point in the risk scale, although other graft and burn areas in general were not associated with an increased risk. 17 Site of burns, grafts and HO are not consistently reported in the surveyed case-control studies and hence do not allow pooled data to be generated for these important measures. Burn aetiology, age and gender were not found to be predictors of HO risk in their analysis.
Anti-contracture positioning and splinting is commenced immediately in most burn services. Prolonged pressure on high HO risk areas during immobilisation has been implicated as a potential predictive factor in the development of the complication. 27 In addition, the intubated patient is unable to communicate to health professionals, so there may be unrecognised, excessive pressure on the posterior aspect of the elbow joint. 19 Munster et al. 28 described the most common occurrence of HO as just posterior to the distal end of the humeral shaft, in the olecranon fossa, and anterior to the insertion of the triceps muscle. They further note that calcification often then spreads to the medial epicondyle of the humerus and occasionally in the lateral structures as well. Levi 12 noted that certain anatomical aspects of the elbow joint, including the superficial ulnar nerve may increase risk of HO through a pathway of neurogenic inflammation. Further supporting mechanical compression as a contributor to risk is the frequent use of the elbow for leverage and the constant pressure on the elbow in immobilised patients which is commonly positioned with the arm in extension and forearm supinated. 27 Lastly, anatomically, the elbow joint is an articulation of two joints in one capsule permitting 2° of freedom for the upper limb. 23 In contrast to most other joints, even in sedentary individuals, the elbow is accustomed to frequent, large arc movements. 23
Given that the pathophysiology of HO is linked to an imbalance of factors leading to abnormal calcium phosphate deposition in tissues, some have tried to isolate whether serum calcium, phosphorus and alkaline phosphate levels can be interpreted to reliably diagnose HO or identify those at risk. 12 To date, the studies have been conflicting in their outcome.6,11,12 The primary issue is that these values are often abnormal in burn patients due to co-morbid factors such as hypermetabolism, electrolyte imbalance or sepsis. Thus, at present, there is a lack of valid screening or laboratory tests for HO.
Onset and differential symptomology
The principle signs and symptoms of HO include: decreased ROM with associated joint stiffness; localised swelling; a painful joint; and possible nerve palsy. 25 At the elbow in particular, ulnar nerve palsy with intrinsic muscle weakness is a relatively common presentation. A consistent early sign of developing HO is a loss of active ROM, or the need for assistance to achieve a ROM that had previously been reached by active motion alone. 28 The ‘locking sign’ can aid differentiation of HO from elbow scar contracture. 11 HO pain was described as ‘sharp’ and ‘stabbing’, a symptom that was distinguishable from the pain experience of burn injury alone. 2 Early clinical signs of HO have been reported at means of 37–43 days post burn injury14,28 though diagnosis is reported as early as 12 days post injury. 15 This preceded radiological confirmation by a mean of at least five days to several weeks.14,25 The unique time frame and specificity of the symptoms paints a picture that will differentiate HO from restrictions related to early scar contracture, which typically develops at four to eight weeks after injury. 29 The symptoms of acute ulnar nerve entrapment are present in ~12% of cohorts with HO. 23 The symptoms of neuropathic pain and marked motor and sensory deficits of the ulnar nerve are diagnostic for HO though are often not the initial signs complained of by patients.
Detection and diagnosis
Widely used diagnostic techniques have low sensitivity or specificity to incremental progression of mineralisation at early time points in HO development. 30 Yeh et al. 31 reported that ectopic bone formation generally does not show on plain film until four to eight weeks after the initial symptoms. Without accurate and reliable early diagnosis, there is little chance of early intervention, and late detection fails to limit unabated progression of HO which often results in joint contractures, nerve entrapment and marked pain. Expensive and time-consuming radiographic techniques, including CT and MRI, provide high-resolution visualisation of late stage HO and 3D CT reconstruction can show the exact anatomic location of HO and is thus helpful for preoperative evaluation. 11 Three-phase bone scintigraphy (SPECT) has been proposed as a method for early detection and may serve as an index for following up on HO maturity. 31 However, the presence of inflammation in burn wound healing may generate false positives when HO is not present. 30
As proposed by Chen et al., 11 a solution to provide early differential diagnosis of HO was documented in a stroke patient. 31 The case report indicated that serial ultrasonography (US) provided earlier and more specific diagnosis of a hip muscle HO lesion than did X-ray or MRI, the latter indicated necrotising fasciitis initially. 31 Ultrasonography depicted clear disease progression, with calcification visible on day 15 after onset of first symptoms. 31 Similarly, in the orthopaedic patients, US has high sensitivity and specificity for early HO diagnosis one week after total hip arthroplasty. 18 Further, evidence of HO on US was detected up to 10–14 days prior to when radiographic evidence appeared. 18 In contrast, Perovsky et al. 30 stated that although US can detect HO sooner than conventional radiography, it cannot distinguish new bone formation from less mineralised mature bone. All told, due to accessibility, low relative cost and lack of radiation, US is a feasible and safe screening tool for early diagnosis of HO in the burn population.11,31
Lastly, it is worth noting emergent technology, suggested in a study of non-invasive near infra-red (NIR) imaging to diagnose and monitor the progression of HO in vivo in a mouse model. 30 NIR detected HO from the first assessment on day 5 and revealed a temporal response in HO formation and heterotopic bone turnover when using NIR contrast agents. Thus, NIR may provide a sensitive and reliable approach for following up dynamic disease processes in the future.
Treatment
Mobilisation and activity
Controversy continues to surround the role of exercise therapy and stretching exercises in the diagnosis and treatment of HO. 13 Active and passive range of motion exercise and minimisation of immobilisation are widely applied principles to mitigate burn contracture. 32 Shafer et al. 3 proposed that the combination of immobilisation, an active inflammatory state (burn wound healing and surgery) and local trauma from early aggressive exercise therapy was implicated in the development of HO. The review results showed that specific prescription of movement therapies and effect on joint trauma and HO progression remains unclear. 12 Little evidence exists to confirm whether stretching should be limited to the arc of tolerable pain and resistance free ROM, or if aggressive range maintenance and stretching techniques can be advocated to optimise post-HO functional outcomes. In addition, it is unclear if, or how exercise therapies should change with clinical suspicion prior to confirmed diagnosis of HO.
The results of this review indicate that patients who have prolonged immobilisation, as well as patients who receive aggressive physical therapy, are both at greater risk for the development of HO.11,23,33 Case reports and animal studies suggest that forceful passive manipulation beyond pain-free ROM during re-establishment of joint range after immobilisation, the density and volume of calcification increases.34–36
In a prospective study conducted in the SCI population, Stover et al. 37 compared aggressive passive ROM (stretching) and active ROM therapy groups and the rate of development of HO. No significant or clinical difference was evident. In patients with established HO, aggressive stretch therapy into pain and resistance, increased independence and ROM, negating the need for surgery in one case. 13 Little scientific evidence exists to aid the prescription of the physical therapy program when HO is confirmed or when it is suspected. 38 This may suggest that immobilisation should be minimised and both active and passive ROM exercises should be continued despite developing or evident HO. The optimal force applied, and acceptable levels of pain, during movement therapies remain unknown. Caution is warranted as potential risks of skin and graft failure, nerve injury and bony fracture increase with the aggressiveness of therapy.
Pharmacotherapy
Indication for drug therapy varies with the stage of the disease and studies have included prophylactic measures to prevent the formation of ectopic bone.34,39 Etidronate disodium (EHDP), a bisphosphonate, has been shown to inhibit hydroxyapatite crystal formation, osteoclast function and bone formation, and therefore theoretically may diminish the incidence or severity of HO. 3 In spinal cord and head injury and orthopaedic surgery populations, EDHP was purported to prevent the development and progression of HO. 40 Yet, other studies suggest that EHDP is ineffective or that its inhibitory effect is transitionary and clinical manifestations and radiographic evidence eventually return with discontinuation of the drug.41–43 In burns, Shafer et al. 3 showed EHDP did not demonstrate clinical efficacy in treatment of HO and further, when used prophylactically, HO incidence increased (46.4% with EHDP 600 mg/day versus 13.8% without). Garland et al. 44 found that low dose EHDP (10 mg/kg/d) did not prevent progression of HO.
Non-steroidal anti-inflammatory drugs (NSAIDs) are believed to prevent the formation of HO by inhibiting cyclooxygenase (COX).11,15 After orthopaedic hip surgery in patients, non-selective (COX-1) and selective (COX-2) NSAIDs significantly prevented HO formation more than placebo. 45 Further, their review concluded that COX-1 NSAIDs were significantly more likely to cause more gastrointestinal side effects and be discontinued than COX-2 NSAIDs or placebo. 45 In a randomised, prospective, double-blind, placebo-controlled clinical trial conducted in the SCI population, Rofecoxib (COX-2 NSAID) prevented HO. 46 While promising, the review did not discover any trials exploring COX-1 or COX-2 inhibitors in prevention or treatment of HO in burn patients. It would appear prudent to conclude that COX-1 NSAIDs are not recommended in burns due to their side effect profile, including major bleeding and negative influence on wound healing and graft take. 11 Further research is warranted as to the use of COX-2 NSAIDs in the prevention and treatment of HO in burn patients.
Surgery
Surgical resection of HO is indicated in patients with limited ROM after non-surgical treatment. A delay of 12–24 months, to ensure bone maturation and reduce the risk of HO recurrence, is recommended. 47 However, such delay in release surgery has been associated with up to 30% of patients with permanent loss of ROM (>25% of normal range),48,49 and up to 25% postoperative iatrogenic or persistent ulnar nerve lesions. 50 Long-standing dysfunction of the elbow is compounded by secondary scar and soft-tissue contracture, joint arthrosis from ligament and joint capsule fibrosis; muscle atrophy and articular cartilage degeneration.47,51 Further, in a qualitative study, HO and loss of ROM was associated with poorer functional outcomes and negative impact on participation and return to normal social roles. 2 In a neurological trauma population, delayed surgery did not correlate with clinical necessity of resection. 52
Thus, earlier excision of HO has been explored. Chen et al. 47 suggested early excision simplified the operative procedure and reduced the risk of damage to structures that are important for elbow stability. These authors retrospectively reviewed 164 HO patients to compare recurrence and elbow function between early (mean, 6.1 months) and late excision. 47 No significant difference was found in terms of HO recurrence between the groups with a low recurrence rate and the establishment of a functional ROM for both. Similarly, Medina et al. 6 performed early excision of HO (mean 5.35 ± 1.46 months post diagnosis). These authors concluded that the approach reduced long-term and postoperative complications and re-established adequate ROM, which was improved significantly when com-bined with physiotherapy within pain-free range. However, a local HO recurrence rate of 30% was reported, necessitating a second surgical episode. 6
Radiation therapy
It must be noted that surgical resection is often associated with complications and a high risk of recurrence. 53 Radiologically, the recurrence rate of HO is 82–100% and 17–58% clinically. 53 As such, preventing the recurrence of HO is crucial in this high-risk population. However, the literature in the burn population is limited and remains controversial with many clinicians expressing concern about the long-term side effects of local radiation such as the development of secondary malignancies.6,54 In the SCI population, Sautter-Bihl et al. 55 concluded that irradiation is an effective neoadjuvant and adjuvant treatment option. The results of this study demonstrated progressive bone formation was prevented in 50 out of 70 hips. 55 Further, a meta-analysis of randomised trials demonstrated that prophylactic irradiation is slightly more effective than NSAIDs in preventing clinically significant HO after major hip procedures. 56 In the burns population, Maender et al. 54 recommend the use of perioperative radiation therapy routinely in conjunction with surgery to reduce recurrence rates. However, this case series is limited by the retrospective nature of the study, small cohort and lack of long-term follow-up. Therefore, multicentre trials with larger cohorts are required to establish the role of prophylactic radiation therapy in the burn population.
Limitations
While it is undeniable that surgical excision of HO remains an integral treatment to restore function, research is required to confirm the optimal timing of resection to balance the competing challenges of inflammatory ankyloses of soft tissues, nerve compromise, risk of recurrence and patient habitual and mental health responses and burden due to reduced ROM.
This review did not include studies published in languages other than English. Thus, studies with larger numbers and better research design may have been missed. The majority of studies found were retrospective with small sample sizes, or were case series or reports. The study types and level of evidence affordable to such research is almost certainly due to the low incidence of major burn injury, the confounding factors presented by acute burns and the even smaller numbers who suffer HO after burn.
Conclusion
There remains little translatable evidence to drive clinical change in the prevention or treatment of HO in burn patients, despite this review spanning 45 years of research. Given the dearth of high level evidence, burn clinicians urgently need more purposeful multicentre data pooling for detailed exploration of the specific risk factors of HO and the development of cost-effective screening and early physical and pharmacological interventions to prevent and/or ameliorate this devastating complication which adds insult after burn injury. While selective NSAIDs hold promise for prevention and treatment, surgery continues to be the best and recommended treatment for established HO when ROM and activities of daily living are significantly affected. While clinicians may uncover treatment options which exacerbate, or prevent HO, bio-scientists need to identify the mechanism and engineers need to focus on the biomechanics of this phenomenon. HO will only be solved by collaboration between disciplines and, therefore, it is essential that disciplines from all fields need to collaborate to improve both the understanding and treatment of HO.
Footnotes
Acknowledgements
Thank you to the Katie Piper Foundation for supporting the open access publication fees for this paper.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding body in the public, commercial, or non-profit sector.