
Abstract
Background
Scar formation is a normal part of the proliferative phase in wound healing where collagen is remodelled to better approximate normal skin. When collagen is not effectively redistributed, excessive scarring may occur. Recently, CO2 laser has emerged as an adjunct in improving scar quality via remodelling and redistribution of dermal collagen fibres. Due to the paucity of literature related to its use in the hands and upper extremities, we created a study to examine its effects on hypertrophic scars focused on the hands and upper extremities.
Methods
Patients treated with CO2 laser for hypertrophic scars of the hand and upper extremity were included. The Vancouver Scar Scale (VSS) and Patient and Observer Scar Assessment Scale (POSAS) were used to assess the progression of scar quality. Unpaired t-tests were performed to determine statistical difference between pre- and post-treatment scores on each scale. Pearson correlation coefficients were used to understand the relationship between number of treatments and scar quality.
Results
Of the 90 patients enrolled, 54 patients completed serial scar assessment forms. All patient and observer-reported POSAS domains showed improvement (P < 0.05) apart from Itching. All VSS domains showed improvement (P < 0.05). There was moderate correlation between overall patient-reported opinion of scar quality and Discoloration, Stiffness and Thickness, and strong correlation between overall patient opinion and Irregularity (r = 0.715). All observer-reported domains were strongly correlated (r = 7.56–8.74) with overall observer opinion of scar quality.
Conclusion
The results of this study may further substantiate CO2 laser as a treatment modality for excessive scarring in a variety of surgical subspecialties.
Lay Summary
Complex trauma and burns that impact the skin sometimes result in abnormal healing of the skin called, “hypertrophic scarring”. In our study we assessed how using focused CO2 laser therapy impacts patients and health care provider assessment of wound progression. Our results were based upon patient reported and healthcare provider observations based upon two standardized forms the Vancouver Scar Scale (VSS) and the Patient and Observer Scar Assessment Scale (POSAS). What we found is that after CO2 Laser Therapy, our 64 patients with 77 treated scars received on average almost 3 treatments and these treatments helped them with physical function and improved aesthetic appearance of their scars. The health care providers also found that the treatments improved functional and aesthetic end points. Overall, our study helps substantiate the body of evidence that using CO2 laser therapy improves aesthetics and function of hypertrophic scars in the upper extremity.
Introduction
Normal wound healing occurs in three stages: inflammation; proliferation; and maturation (remodelling). 1 After surgery, trauma or severe burns, scar formation begins in the proliferative stage as part of the natural healing process. 2 While some degree of scarring is inevitable, excessive scarring can lead to contracture and/or adhesion to surrounding tissues. In these cases, suboptimal outcomes may be attributed to a variety of complications, including the following: poor cosmesis; itching; pain; decreased tissue pliability; and limited range of motion. 2 Hypertrophic scar formation requires a tissue insult that has penetrated deep enough into the dermis to damage dermal appendages, hair follicles and sebaceous glands within the reticular layer. These structures are surrounded by and networked with the basal cells involved in keratinocyte regeneration and re-epithelialisation. 3 In the proliferative healing phase, fibroblasts initiate extracellular matrix (ECM) formation, which is largely composed of collagen. 4 After proliferation, new collagen becomes cross-linked and organised into parallel bundles. 4 Excessive scarring occurs when this remodelling process fails to adequately redistribute collagen across a closed wound. 5
Efforts to combat functional deficits caused by scarring include the following: early mobilisation; splinting; intralesional corticosteroid or anti-neoplastic injections; fat grafting; surgical contracture release; and lasering.3,6 Fractionated CO2 laser ablation entails the application of a 10,600-nm laser calibrated to the appropriate scar depth. While the exact mechanism is still being investigated, it is known that this wavelength effectively targets water molecules found extensively in dermal collagen. 2 The microperforations applied to the skin create columns of tissue vaporisation within the disorganised collagen scar. 2 This releases a substantial amount of tension and creates a controlled, localised environment for scar remodelling, effectively reducing scar density and reorganising collagen in a network that more closely approximates preinjury architecture.3,7
Hypertrophic, burn, keloid, pigmented and acne scars have all shown improvement when treated with CO2 laser.8–11 McGoldrick et al. published a two-part review article detailing over 20 years of experience treating a wide variety of scar types using lasers in conjunction with a variety of other treatments.8,9 While they reported subjective improvement in these scars and high rates of patient satisfaction, there was no standardised measure of this subjective improvement.8,9 Objective assessments provide valuable clinical data, but fail to account for patient perceptions which ultimately influence final satisfaction. 12 As treatment modalities evolved, subjective scar assessment tools have been developed to allow a more holistic evaluation of scar quality. Given the known effects of excessive scarring on quality of life and the variability of patient factors influencing perception of outcomes, valid patient and observer-reported outcome measures are needed to address the full spectrum of scar quality. 13
The Vancouver Scar Scale (VSS) was first described by Sullivan in 1990 and includes four variables: vascularity; height/thickness; pliability; and pigmentation. 14 While observer scores correlated well with objective measures such as tonometry, the VSS lacked a patient-reported component. More recently, the Patient and Observer Scar Assessment Scale (POSAS) was developed to include both patient and observer rankings of various dimensions of scar qualities. 12 Other scales have been created to simplify the VSS (e.g. Visual Analog Scale with scar ranking), broaden the scope of assessable scars (e.g. Manchester Scar Scale) or focus the scale to address particular injury patterns (e.g. Stony Brook Scar Evaluation Scale) (Table 1). 12 However, the VSS and POSAS remain the gold standard scales for subjective scar evaluation.15–18
Comparison of scar assessment scales.*

*None of the scar scales measure the following: the amount of total body surface area that is scarred; the functional disability caused by scar; and the effects of pain and pruritus in terms of activities of daily living.
VAS, visual analogue scale; VSS, Vancouver Scar Scale.
The current literature evaluating CO2 laser therapy is largely focused on the use of these treatments for burn scars. Although hands are involved in as many as 90% of all burns, the literature lacks studies focused on CO2 laser therapy for burn and traumatic scars of the hand and upper extremity.3,6 To fill this gap in the literature, we designed a study to evaluate the efficacy of this treatment in a hand surgery practice at a single academic hospital using the VSS and POSAS to track scar quality progression.
Methods
Patients treated with CO2 laser for traumatic and/or burn scars of the hand and upper extremity were included. The Lumenis® Ultrapulse laser was used with the following settings in our cohort: 120–130 mJ micropulse energy; 250 Hz pulse rate; 800–1500 ms duration; 3% density; random pattern; and 1.3 mm spot size. Spot shape varied depending on the shape of the scar. The VSS and POSAS were used to assess the progression of scar quality before and after laser treatments. Patients and observers were blinded to previous scores. Patient charts were reviewed for additional subjective data not captured on the VSS or POSAS.
Unpaired t-tests were performed to determine statistical difference between pre- and post-CO2 laser treatment scores on each scar assessment scale. Pearson correlation coefficients were calculated to assess the relationship between number of treatments and improvements in scar quality as well as how individual POSAS variables may have influenced the overall opinion of both the patient and observer.
Results
In our cohort, 64 participants with 77 scars completed pre-laser Patient POSAS forms, and 54 completed multiple, serial scar assessment forms with a mean of 2.8 treatments and an average follow-up of 23.3 months from initial treatment. In total, 44 patients had pre-laser Observer POSAS and 41 had post-laser Observer POSAS, while 42 patients had pre-laser VSS forms and 40 had post-laser VSS forms.
The average patient age was 28.4 years (age range = 2–81 years) and 54.7% of patients were male. The most common cause of scarring was thermal burn (45.5%) followed by traumatic laceration or avulsion (20.8%). Mean scar surface area was 333.4 cm2, and median surface area was 130.6 cm2 (range = 2.2–4047.8 cm2). Mean time from initial injury to first CO2 laser treatment was 12.6 months (range = 2.9–49.8 months). Mean time from laser treatment to completion of assessment forms was 3.2 months (range = 1.1–9.7 months) (Table 2 and Figure 1).

Mechanisms of hypertrophic scar formation.
Demographics.

All POSAS patient-reported domains had significant improvement (P < 0.05) with the exception of Itching (P = 0.242), which still showed mean improvement (Table 2). All POSAS observer-reported domains showed significant improvement (P < 0.05). All VSS domains showed significant improvement (P< 0.05) (Table 3).
Unpaired t-tests.
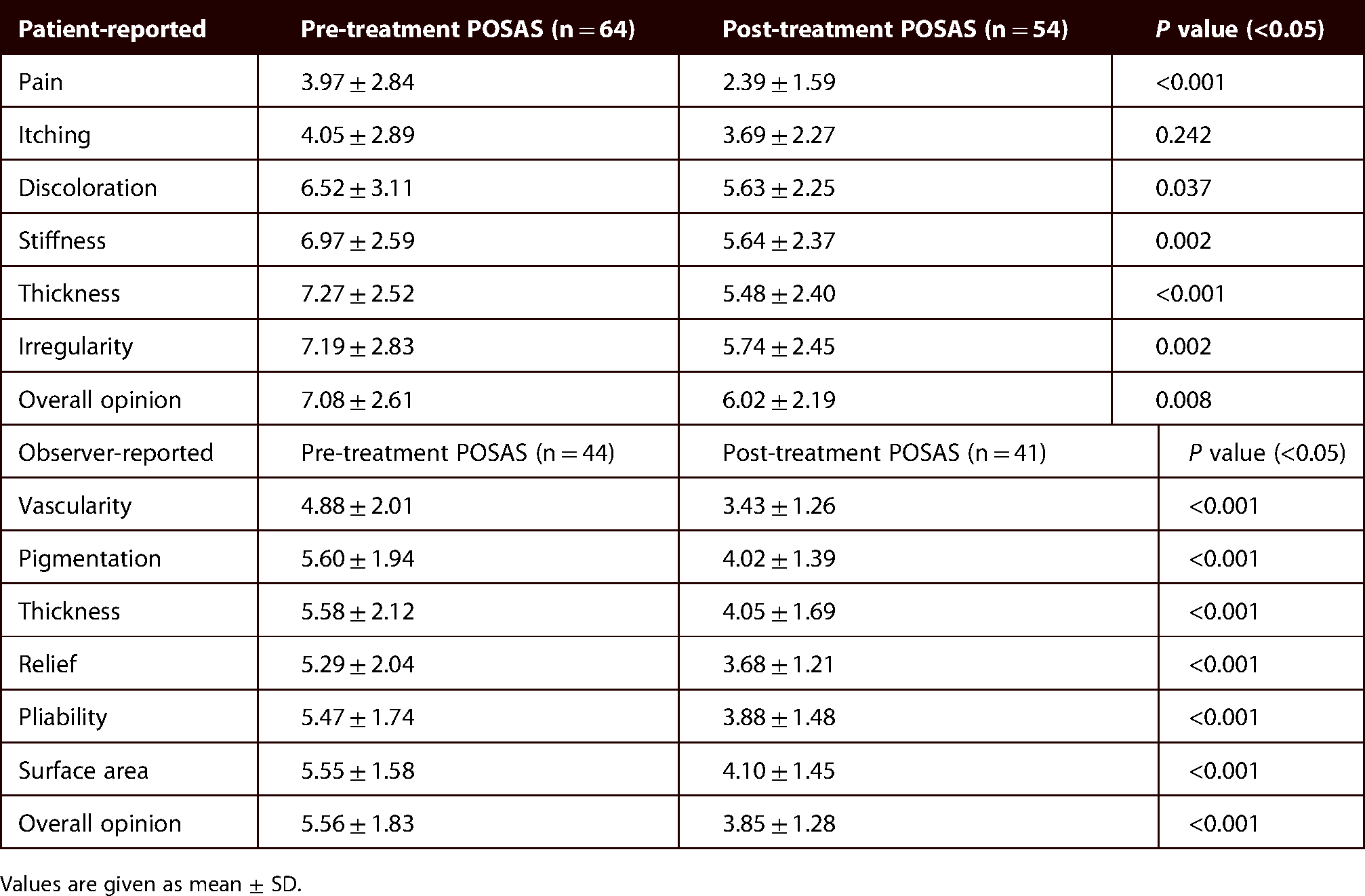
Values are given as mean ± SD.
Pearson correlation coefficients indicated moderate correlation between overall patient-reported opinion of scar quality and patient-reported Discoloration, Stiffness, Thickness and Irregularity. All observer-reported domains were strongly correlated with final overall observer opinion of scar quality (Table 5). Improvements in patient-reported POSAS Discoloration, Stiffness, Thickness and Overall Opinion were weakly correlated (r = 3.52–4.39) with improvements in observer-reported POSAS counterparts (Pigmentation, Pliability, Thickness and Overall Opinion). Number of treatments was not significantly correlated with overall patient rating of scars (r = 0.012).
Pre- and post-treatment VSS results.

Values are given as mean ± SD.
VSS, Vancouver Scar Scale.
Pearson correlation coefficients (r) for each scar assessment domain in relation to overall scar opinion score.

At routine follow-up visits, many patients were asked to report the percent improvement from pre-laser conditions, whether they would repeat the treatment if they could go back to pre-treatment conditions, and if they would recommend this treatment to others in a similar situation. Of the 34 patients with these subjective responses, 33 (97.1%) stated they would repeat the treatment and/or recommend CO2 laser to others. Mean patient-reported improvement was 53.7% (range = 0%–99%). The strongest correlation between POSAS dimensions and patient-reported percent improvement was Discoloration (r = 0.318). Photographs of pre- and post-laser scars can be found in Figures 2–4.

(A) Traumatic scar before initial laser treatment. (B) Six weeks after second administration of CO2 laser.

(A) Burn scar before initial CO2 laser treatment. (B) Scar after two laser treatments (five months after initial laser treatment, one month after second treatment). (C) Scar after three laser treatments (10 months after initial laser treatment, two months after third treatment).

(A) Reverse radial forearm flap harvest scar before laser treatment. (B) Harvest site scar after two laser treatments (four months after initial laser treatment, two months after second treatment).
Discussion
Hand surgeons are positioned at the crossroads of multiple specialties, including general, plastic and orthopaedic surgery. Given the broad spectrum of injuries seen in practice, it is necessary for hand surgeons to incorporate emerging treatment modalities such as CO2 laser therapy that are commonly used in other subspecialties. The efficacy of CO2 laser is well documented in the burn literature. 16 As previously mentioned, the hands are involved in the vast majority of all burn injuries; however, there are few reports specific to hand and upper-extremity scars.3,19 Given its ease of use, CO2 laser is an accessible option for all subspecialties treating patients with excessive scarring and should be included in scar management algorithms.
The literature indicates that VSS provides reliable subjective assessments and has historically been considered the gold standard due to its high inter-observer reliability. 10 While burns and traumas are not the only scars treatable by ablative CO2 laser, they comprise the bulk of cases that may benefit from this treatment. One study of 11 patients with burn scars of the face, neck and upper extremities followed patients who had received 10 treatments over an average period of five weeks. At six months, there was a significant improvement in VSS scores compared to baseline measures. Skin biopsies taken before and after treatment from four patients showed newly formed dermal papilla in the upper dermis, corroborating clinical findings of improved in surface smoothness and tension. 20 A recent randomised controlled trial also demonstrated improvements in burn scars after CO2 laser in both VSS and histological parameters. 21 A large database study including 295 patients assessed the impact of burn scar severity (measured by the VSS) on increases in time to healing (TTH). 17 Investigators found that a VSS score increase of 0.11 points (P ≤ 0.001) was associated with an additional day of TTH, irrespective of differences in total burn surface area or surgical intervention. These findings suggest that VSS scores are a valid indicator of burn scar severity. 17
While the VSS has demonstrated clinical utility, it lacks a patient-reported component, and the POSAS has recently gained popularity by addressing this shortcoming. 15 In practice, functional outcomes such as range of motion and return of sensation are often the primary concern of surgeons managing excessive scarring. Unfortunately, the impact of scars reaches beyond functional deficits and is known to affect patients’ social and psychological wellbeing.22,23 Given these additional considerations, patient perceptions are now considered an essential component of any scar assessment algorithm. 24 While some reports have shown only low correlation between subjective assessment using POSAS and objective assessment using spectrophotometer and ultrasonography, 10 patient perception may be given priority in assessing parameters that do not cause functional impairment. Patient opinions of cosmesis can determine, to some degree, the psychosocial impact of scars.23,24 Ultimately, the goal of any scar treatment is to improve patients’ quality of life.
One study tracked the progress of 10 patients with hypertrophic burn scars treated by CO2 laser over the course of six months after treatment. 16 VSS and POSAS scores showed significant improvement, as did the quality of life rating measured by the Dermatology Life Quality Index (DLQI). 16 A separate study followed 47 burn patients with at least one laser treatment cycle. 18 Patients were then evaluated using the POSAS, VSS and Burn Specific Health Scale Brief (BSHS-B) to measure quality of life after burn injury and lasering. Ultrasound measurements were used to objectively measure scar thickness. After an average of 55 days after treatment, average scar thickness decreased from 2.4 to 1.9 mm (P < 0.001). Mean VSS dropped from 7 to 6 (P < 0.001) and mean overall patient-reported POSAS score improved from 9 to 5 (P < 0.001). Quality of life scores also improved significantly (median 120 to 135; P < 0.001), and improvements following treatment were equally significant across all levels of scar maturation. 18 These studies show that improvements in POSAS and VSS scores after treatment with CO2 laser are indicative of improved quality of life.
Results from our cohort support the existing body of literature demonstrating the efficacy of CO2 laser therapy as shown by significant improvements in all but one POSAS domain. Of note, our data suggests that patients’ overall opinion of their scar is influenced more by functional and aesthetic variables than sensory and pain variables (Table 4). The weak correlation between improvements in patient versus observer-reported POSAS domains suggests that patient opinions are distinct from observer opinions of scars.
The present study is limited by the heterogeneity of scar types and severity, making it difficult to discern which scars may benefit most from laser therapy. Specifically, time to first laser therapy was variable among patients who had severe thermal burns compared with patients who had reactive scar formation from a recent procedure. The latter patients received CO2 laser therapy earlier in their clinical course compared with the burn patients. This phenomenon is consistent with the literature where surgical scars may receive intervention in as soon as three weeks compared with burns where first treatment after a burn occurs at approximately 18 months.11,25 Another challenge posed to researchers and clinicians treating hypertrophic scars is generating objective photographic imaging to track progression of scars from visit to visit. Two dimensional photographs are the most common assessment tool to evaluate scar progression, but plain photographs alone may introduce bias due to logistical constraints and provides inconsistent objective analysis compared to other means of assessments (i.e. VSS).26–28 Three-dimensional stereophotogrammetry does offer some advantages over two-dimensional imaging in objective scar assessment because of features such as volume measurements and inter-operator reliability.29,30 However, scar location on a curved surface creates challenges to generate a consistent and reproducible volume measurement and may be challenging for ubiquitous use due to the expertise necessary for consistent re-calibration as well as angular measurements. 30 This imaging technique is also limited by scar size, wherein individual photos of scars must be summed causing possible inaccurate measurements and inconsistent data over the life of a scar that is larger than the visual field that the camera requires. 29
The final and most relevant challenge posed to any researcher studying hypertrophic scarring is distinguishing between successful therapeutic intervention and natural progression of hypertrophic scarring. As previously mentioned, early intervention with laser therapy has demonstrated better outcomes in specific populations. However, the question remains as to whether the natural regression of hypertrophic scars is the primary mechanism by which the outcome was achieved given the most common outcome in hypertrophic scars is resolution within one year of the initial scar formation.11,31–33 Given the potential for spontaneous improvement, the present study is limited as we did not compare laser treatment to outcomes of similar scars that did not receive CO2 laser.
Future studies should include a broad range of scar injury mechanism with sufficient sample sizes and a control group to adequately compare laser treatment to non-laser treatment. Time to first laser treatment should also be evaluated for potential impact on outcomes. The literature suggests that CO2 laser therapy benefits are equivocal independent of scar age in burn patients but patients undergoing surgical scar laser therapy within three weeks of the procedure demonstrated superior results compared with delayed intervention.11,18 Another important consideration for future clinical studies evaluating hypertrophic scar outcomes should also include a non-intervention arm given the fact that the natural course of hypertrophic scars is complete regression within one year.11,31–33 Quality of life scales were not used to assess the psychosocial impact of scar improvements. Psychosocial measures, coupled with the VSS and POSAS, may provide a more complete picture of scar outcomes.
Our study provides valuable data assessing the utility of CO2 laser therapy in treating scars of the hand and upper extremity. Results of this study may further substantiate CO2 laser as a treatment modality for excessive scarring, particularly in subspecialties where it is not already common practice.
Footnotes
Acknowledgements
The authors acknowledge Cheryl Edwards, Erica Carter and Nancy Swinford for their contributions to data collection for this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
How to cite this article
Cox C, Bettiol P, Le A, MacKay BJ, Griswold J and McKee D. CO2 laser resurfacing for burn and traumatic scars of the hand and upper extremity. Scars, Burns & Healing, Volume 7, 2021. DOI: 10.1177/20595131211047694.