
Abstract
Needle procedures are one of the most common reasons for children to visit hospitals. If unaddressed, negative needle experiences can worsen over time and lead to needle noncompliance, needle fears, and healthcare avoidance. This mixed methods pilot study tested the effect of combined music therapy and standard pharmacological care compared to standard care alone on fear and discomfort in children in connection to a scheduled needle procedure. Children and their parents were also interviewed on their general experience of music therapy and how they regulated fear and discomfort during needle procedures while participating in music therapy. Thirty children aged 0 to 15 and their parents were recruited at the pediatric outpatient unit at The Central Hospital in Karlstad, Sweden. The participants were randomized to an intervention group with music therapy and to a control group that received standard care alone. The children rated their fear and discomfort before, during and after a needle procedure on a child-friendly visual analogue scale. The children and parents who were randomized to the music therapy condition were interviewed about their experiences of music therapy as procedural support. No significant differences between the intervention group and the group with standard care alone were found, indicating that the two groups were equivalent with regard to experienced fear and discomfort. The content analysis of the interviews indicated that the children and their parents considered that the music therapy intervention promoted the participants’ emotion regulation, promoted adaptive coping strategies for both children and the parents, and favorably but also ambivalently affected the context and interactions in the procedural room.
Keywords
Introduction
Routine needle procedures are one of the most frequently used medical procedures for children and are perceived as fearful by the majority of this population. Research has estimated that as many as 70% of school-aged children fear vaccinations and other needle procedures because of needle fear and injection pain (Constantin et al., 2023; Taddio et al., 2022). The level of fear is of great importance for how children experience pain (Hedén et al., 2020). Negative memories of distressing and painful needle procedures heighten the risk for increased pain and fear in similar situations in the future (Noel et al., 2012; Noel et al., 2017). Long term, this increases the risk for developing needle fear and phobia, healthcare avoidance, immunization non-compliance, as well as chronic pain (Pavlova et al., 2022). In pediatric care, fear and pain management has long been under-prioritized, which may increase the risk for these undesirable consequences across one's lifespan (Taddio et al., 2022).
In addition to fear of needles, the hospital environment itself can cause discomfort in children. In healthcare settings, children might feel abandoned, not listened to, disrespected, vulnerable, and not given the opportunity to influence their own care (Forsner et al., 2009). Some children strongly believe that the healthcare professionals will cause them harm when they have their blood samples taken (Forsner et al., 2009). There is a risk of developing maladaptive behaviors, separation anxiety, and anger outbursts, both in connection to, and long after, a negative healthcare experience (Millet & Gooding, 2017). Previous studies have shown that topical lidocaine-prilocaine emulsion cream (EMLA®) reduces vaccination-related pain (Taddio et al., 1994). There are, however, side effects with sedatives and other pharmacological treatments. In Swedish pediatric care, it is recommended that pharmacological interventions are only used in conjunction with non-pharmacological options during painful procedures with infants and children (Swedish Medical Products Agency, 2014). Multiple combined psychological interventions are preferred, with cognitive and behavioral strategies that take biopsychosocial factors into account (Leroy et al., 2016). These non-pharmacological options are non-invasive, without known side effects, and they enable children to develop their own adaptive coping strategies (Birnie et al., 2015; Birnie et al., 2018).
Emotion regulation is defined as the process through which individuals influence the experience and expressions of emotions (Gross, 2002). It is imperative for our psychological and physical health as well as for social interactions to be able to adapt our emotive responses (Kim and Hamann, 2007). A child needs help with emotion regulation and prompting by caregivers and other adults to engage in regulative adaptive behaviors that will reinforce the child's own ability to cope with experiences such as venepuncture (Constantin et al., 2022). However, some parents experience increased stress and anxiety themselves in connection to their child's needle procedure and may therefore have problems with regulating and supporting the child. When the child cries and shows anxiety, fear, and discomfort, some parents often use unhelpful reassuring verbalizations, which instead increases the child's distress in a non-regulatory feedback loop (Constantin et al., 2022, 2023; Loewy, 2019; Swedberg Yinger, 2016). Parents’ and staff's acceptance of the child's needs of anxiety release, and of a sense of inclusion and control in the situation, is encouraged and supported in music therapy (Loewy, 2019). When children are given the opportunity to develop adaptive coping strategies, they can increase their confidence in their own abilities, strengthen their sense of control, and gain confidence in their capacity to complete tasks – also described as self-efficacy (Bandura, 1997).
Live interactive music therapy administered by trained music therapists for procedural support is an example of evidence-based non-pharmacological emotional support used in healthcare settings (Bradt, 2013). Music therapy as procedural support is defined as the use of music and aspects of the therapeutic relationship to promote healthy coping and decrease distress in individuals undergoing medical procedures (Ghetti, 2012). The music therapist works within a systematic therapeutic process through personally tailored music experiences for symptom management in a biopsychosocial framework (Bradt et al., 2015). The music is used interactively, entrained to the patient's affective, emotional, and/or physical state, thus offering integration instead of distraction (Loewy, 2019). Relationship-focused methods are a typical feature of music therapy, situating music-therapy within the family-centered care framework. Family-centered care (FCC) is an approach to health care that is respectful of and responsive to individual families’ needs, culture, and values (Davidson et al., 2017). FCC ensures that care is planned around the whole family, not just the individual child, and that all the family members are recognized as care recipients. FCC also comprises, for example, a culturally competent and respectfully supportive parent-professional collaboration and continuous information sharing (Institute for Patient and Family-Centred Care, 2010). Within this framework, the music therapist works in a collaborative and culturally sensitive way, building relationship between the child, the parent, and the therapist, based on equality and participation so that the family's knowledge and skills are fostered. Music therapy plays a unique role in humanizing the experience of hospital care for the child and the parents and helps to acknowledge each person's individuality and dignity (Ghetti, 2013). In Swedish pediatric care, comprehensive inclusion of and collaboration with parents is considered best practice.
In previous research, music therapy interventions are associated with several positive outcomes, for example contributing to regulation of respiratory rate, saturation, heart rate, cortisol levels, and blood pressure (Stegemann et al., 2019; Uggla et al., 2018). In addition, music interventions decrease pain perception, fear, anxiety, and build resilience in both children and their parents in connection to medical procedures (Caprilli et al., 2007; Cousin et al., 2022; Dileo, 1997; Ghetti, 2012; Klassen et al., 2008; Malone, 1996; Pfaff et al., 1989; Sanfi, 2012; Swedberg Yinger, 2016; Swedberg Yinger & Gooding, 2015; Turry, 1997). Music therapy as a procedural support is well documented since the 1990s in a small but growing number of pediatric medical contexts in the developed world. A number of studies have investigated the effects on emotions and perceptions of music therapy as procedural support for children (Beer & Lee, 2017; Dileo, 1997; Edwards & Kennelly, 2016; Loewy 1999; Loewy, 2022; Noguchi, 2006; Turry, 1997). Lately, there is also an increasing interest in music therapy as procedural support for infants and their parents (Ullsten et al., 2018; Ullsten, 2019). To date, there is no available study investigating effects on emotions and perceptions of music therapy as procedural support for children in a Swedish pediatric outpatient setting. This mixed methods study examines the effect of music therapy combined with standard pharmacological care compared to standard care (pharmacological care combined with routinely offered non-pharmacological interventions) on fear and discomfort for children and adolescents undergoing a needle procedure. This study also investigates how children and adolescents regulate their emotions during needle procedures while participating in music therapy, and examines children's, adolescent's, and parents’ general experience of music therapy in this context.
Methods
Overview of the Study
This study is a randomized controlled pilot study with a mixed methods design. In music therapy research, mixed methods designs are recommended because of the possibility of elucidating the studied phenomena from multiple perspectives to achieve a holistic understanding and better-informed clinical practice (Bradt et al., 2013).
Informed consent to participate in the study was obtained from the parents of each child. Both the parents and the children received information about the study prior to the hospital visit. Children over the age of 15 also gave verbal assent to participate. The study was approved by the Swedish Ethical Review Authority (Dnr 2021-07020-01) and was a research collaboration between Örebro University and Region Värmland, Sweden.
Interventionists
All authors (AU, AKS, EL, SE) were involved in designing the study. Two psychology master students (AKS, EL) had the primary responsibility for carrying out the data collection and performing the analysis. They were supervised throughout the whole process (by AU and SE). The music therapy intervention was designed and performed by the music therapist (AU), who served as interventionist for all participants in the intervention group.
Recruitment and Randomization
Recruitment lasted from mid-February to the end of March 2022. Children and parents who visited the Pediatric outpatient unit at The Central Hospital in Karlstad, Sweden, for a scheduled needle procedure during the data collection period, were recruited. This pediatric outpatient hospital unit treats children with diverse medical conditions: children with cancer, heart disease, and diabetes. The unit also performs diagnostic procedures and prepares children for radiology or other examinations and treatments. The children who participated in the study, visited the pediatric outpatient unit for blood tests, injections such as COVID-19 vaccine, for various imaging examinations (kidneys, small intestine, eye, and brain), and for infusion therapy. Exclusion criteria were children older than 18 years old and/or arriving to the clinic without a guardian. No children were excluded based on the exclusion criteria.
Participants were randomized to either a control group with standard care comprising pharmacological and non-pharmacological standard treatments, or to a music therapy group that received a single music therapy intervention in addition to pharmacological standard care. To assure the groups were similar regarding age distribution, the children were first ascribed to a specific age group (age 0–4, 5–10, 11–15, or 16–18) and then randomized in blocks of two. An experienced researcher who was blinded to the purpose and design of the study was responsible for the randomization. Group affiliation was then assigned to each child in the order that their appointments were scheduled. Affiliation was communicated to the participants on arrival in the treatment room. Due to the nature of the intervention, the nursing staff, interventionists, and participants could not be blinded to group allocation during data collection.
Initially, 44 children and their parents were considered eligible for the study and were asked to participate, and six families declined (Figure 1). In total, 38 parents and children agreed to take part, but on the day of the data collection, five families declined participation or cancelled their appointment. Three children were hospitalized before data collection started. In the end, 30 children and parents completed the data collection: 16 in the music therapy intervention group and 14 in the standard care control group.

Flowchart of procedure and attrition.
Setting
In addition to pharmacological treatments and as part of standard care, the healthcare professionals at the pediatric outpatient unit offer a range of non-pharmacological, cognitive, and behavioral strategies as adjuvant pain management. These are distracting techniques, such as playing with toys, watching movies, playing mobile games, and blowing bubbles; non-pharmacological options such as skin-to-skin contact or comfort positioning with parents holding the child on their lap; and psychological strategies, such as picture/photo storybook for the venepuncture or verbal encouragement from staff. The clinic also has a psychosocial team with psychologists, counsellors, and child life specialists. However, the team has many families on the list waiting for treatment for fear of needles. The pediatric outpatient unit is a family-centered clinic. It is here considered best practice and part of the clinic's routines to always have a parent accompanying the child or adolescent to the procedure.
Procedure
The researchers met the families in the waiting room. Consent forms were collected, or opportunity was given to fill in the form on site. After this, the children and their parents were invited into the procedure room where one researcher (AKS or EL) was present. For the music therapy intervention group, the music therapist (AU) was also present. The nurses then performed the medical procedure according to standard care. As part of standard care, all children received pharmacological treatments, e.g., topical anesthetic, and selections of non-pharmacological interventions. The participants in the intervention group received live interactive music therapy administered by a trained music therapist in conjunction with pharmacological standard care.
Depending on the type of needle procedure and the child's fear levels, the procedure time ranged from 5 to 20 min. The procedures were video recorded with a camera on a tripod, which recorded the child as well as the parent and, in the intervention group, also the music therapist. After the procedure, all participants in the music therapy intervention group went to another room for an interview. Two researchers (AKS, EL) were present during the interviews; one conducted the interview and the other recorded the interview with QuickTime Player on a computer. The interview time ranged from 5 to 12 min.
The Music Therapy Intervention
The children who were randomized to the music therapy group, met the music therapist (AU) in the procedure room. The music therapist brought a trolley containing songbooks and various musical instruments including piano, drums, and numerous hand percussion instruments. While the nurses started to prepare for the needle procedure, the music therapist assessed the participants’ individual needs and music preferences. The therapist then invited the child and parent to participate in musical interplay, which continued during the procedure and for a short time after, to promote recovery and closure. The interaction was adapted to the child's need for either relaxation or activation and tailored to the child's musical interest and culture. Before, during, and after the needle procedure, the music therapist, the child, and the parent created music together by singing pre-composed songs, improvising on instruments, or composing new songs, integrating music therapeutic strategies based on previous research (Bradt, 2013; Dileo, 1997; Ghetti, 2012; Loewy, 1999; Sanfi, 2012; Swedberg Yinger, 2016; Turry, 1997). The total time given by the music therapist for the treatment group ranged from 10 to up to 30 min. The music therapy intervention included an approximately 5 min long verbal pre-procedural assessment aiming at meeting the individual needs of the participants, as well as a musical closing providing recovery for the child and parent.
The music therapy intervention in this study was informed by attachment theory and transdisciplinary biopsychosocial pain theories and models for pain management and procedural support, including the neuromatrix theory of pain (Melzack, 1999), the biopsychosocial model (Engel, 1977), the social communication model of pain (Craig, 2015), procedural comfort care (Leroy et al., 2016), working model of music therapy as procedural support (Ghetti, 2012), and the integrative model of procedural music therapy (Loewy, 2019). Since age-appropriate pre-procedural preparation is crucial for mitigating pain, the healthcare staff and music therapist constantly monitored and coordinated the comfort process and procedural process, and only proceeded when comfort was optimal (Leroy et al., 2016). Ongoing assessment was a vital component of the music therapy support in this study (Ghetti, 2012; Loewy, 1999; Loewy, 2019; Turry, 1997).
Quantitative Measures and Analysis
Power Calculation
Power calculations, based on previous studies using the Visual Analogue Scale (VAS) (Birnie et al., 2019), showed that a total of 26 children (13 in each group) needed to be included to ensure statistical power (80% and 0.05 level of significance). To compensate for potential dropouts, it was decided to include 30 participants in the study.
Demographic Information
Questions regarding age, gender, and type of needle procedure were asked.
Child Friendly Visual Analogue Scale (VAS)
An assessment scale used with children from diverse backgrounds should be simple to score and interpret and it should be easy to apply in younger children with limited cognitive abilities and linguistic skills (Setty et al., 2019). Previous studies in health care settings suggest combining the numeric rating scale with emojis as a way to represent mood (He et al., 2022; Pourmand et al., 2020; Setty et al., 2019). The children in this study were asked to self-report the intensity of their fear and discomfort related to the needle procedure on a modified child-friendly visual analogue scale (VAS). VAS is easy and quick to handle and can be used for children over the age of three (Birnie et al., 2018). The VAS used in this study, was an open-source version inspired by validated faces scales modified to only assess fear and discomfort and not pain. VAS ranged from 0 (no fear/discomfort) to 10 (worst possible fear/discomfort) on a 100 mm line. The space between each number was 10 mm. The faces or emojis included in the scale, ranged from a happy and relaxed emoji, to a sad, crying emoji (a visual example of this VAS scale with emojis is found in He et al., 2022).
The children in the study self-reported the intensity of their fear and discomfort by pointing to the emoji or verbally expressing a number that best corresponded to her/his emotional state in the moment. If the child was younger than four years, the question was directed towards the parent who rated their perception of the child's emotional state.
Statistical Analyses
Pearson's chi-squared test was used to ascertain differences in the demographic data (age, gender and type of procedure) between intervention group and control. This test was used because the variables compared were categorical and not numerical, which speaks in favor of non-parametric alternatives. The normal distribution in age for both groups was examined using the Shapiro–Wilk normality test as it suited the sample size. The same test was also conducted to assess the distribution of feelings of fear and discomfort (VAS), at the three time points in both groups. The three time points were before, during, and after venepuncture.
To analyze the differences between the two groups on fear and discomfort, a 2 × 3 mixed ANOVA was conducted as this analysis allows comparisons of differences between and within groups at all time points. ANOVA also provides the opportunity to measure the combined effect, known as the interaction effect. Follow-up post-hoc tests using Bonferroni adjustments were conducted to further examine significance. This method was used as it was believed suitable for analyzing differences over time between groups in randomized controlled trials (Comer & Kendall, 2013). Three outliers (measuring points) were found and adjusted from extreme values to values that were more representative for the collected data. Statistical analyses were performed using IBM® SPSS® 27.0 statistics software for Mac.
Qualitative Measures and Analysis
Interviews
The children and parents in the music therapy group were interviewed after the venepuncture using a semi-structured interview design. Focus for the interviews was to investigate the child's and the parent's shared experiences of the music therapy intervention and its potential to regulate the dyad's emotions. Hence, our qualitative research questions only aimed to investigate the overall experience of music therapy. The child and her/his parent were interviewed collectively despite the risk that both parties could influence each other's responses. The study design also complied with the family-centered policies on the pediatric outpatient unit, never separating the child from the parent during their healthcare visit, not to exacerbate any procedural trauma.
The two researchers used an interview guide (Appendix 1) with open-ended questions related to experiences of the medical procedure, including how the family experienced the visit, what kind of strategies the family usually uses to regulate their emotions, how the parents coped with their child's distress during the venepuncture and whether the music therapy intervention promoted the child's emotion regulation capacities. The interview questions were developed in consultation with an experienced child psychologist employed by Örebro University, to ensure that the questions were adapted to the children's age and developmental stage.
Qualitative Content Analysis
The interviews were analyzed with Graneheim and Lundman's qualitative content analysis (2004). This method focuses on the interpretation of a text, for example people's description of experiences (Graneheim & Lundman, 2004). An inductive approach was applied, which meant searching for patterns without predetermined premises and thus moving from data to a theoretical understanding (Graneheim et al., 2017). Table 1 shows an example of the qualitative content analysis process in this study.
Example of the qualitative content analysis process.

Initially, the researchers (AKS, EL) individually listened to all interviews and transcribed the recorded interviews separately. AKS and EL read through each other's transcripts several times and color-coded the children's answers as well as the parents’. To avoid influencing each other's readings, the researchers separately de-contextualized the content in the respondents’ answers. The de-contextualization process generated two separate analyses. De-contextualization was done by dividing the respondents’ answers into meaning units, i.e., sentences, utterances from individual interviews, or paragraphs that relate to each other through content and context, and that also related to the research questions. After that, the meaning units were condensed and shortened to core sentences to find similarities and differences in the material. AKS and EL then met together to discuss the data and the two sets of meaning units to find units represented in both analyses. The meaning units from the transcribed interviews generated codes that were grouped into categories, so-called abstraction, which is part of the re-contextualization process. No subcategories were identified as the data sample was estimated to be too small. AKS and EL re-contextualized the categories, which all authors of this article met to discuss and reconstruct together into themes. In the interpretation phase, which is also part of the re-contextualizing process, the analysis was moving from descriptions of the manifest content to interpretations of the latent content. The manifest content in the categories was filtered through the study's theoretical framework, the biopsychosocial perspective (Engel, 1977), guiding the articulation of the latent content – the themes in this study. The biopsychosocial perspective (Engel, 1977) was chosen as a relevant theory and framework for the analysis since health and sickness, pain, stress, and fear involve biological, psychological, and social factors, which are addressed in music therapy treatment. The researchers used the biopsychosocial perspective to guide them in their content analysis, identifying meaning units, codes, categories, and themes.
Results
Thirty children and parents completed the data collection: 16 in the music therapy intervention group and 14 in the standard care control group. Pearson's chi-squared test showed no significant differences between the groups. The Shapiro–Wilk normality test showed normally distributed data in the intervention group but not in the control group. Furthermore, normality testing of the VAS-variable showed that the scores at all time points for both groups were evenly distributed, except for the second VAS-scores reported by the intervention group; these were positively skewed and had a leptokurtosis curve. Since the ANOVA is known for its robustness regarding non-normality (Blanca et al., 2017), it was decided to proceed with the chosen analysis. For an overview of the participants’ demographics see Table 2.
Overview participant demographics.

Quantitative Results
There were no significant differences between the intervention group with music therapy and the control group that received standard care alone regarding fear and discomfort, F(1, 28) = 0.52, p = .48, n2 = .02. In addition, no significant interaction effect between time and group was found, F(2, 56) = .27, p = .77, n2 = .01, indicating no significant differences between the groups regarding fear and discomfort before, during, or after the needle procedure. Also, there were no significant differences in perceived fear and discomfort over time for the two groups (Table 3).
Means and standard deviations for the VAS-scale.
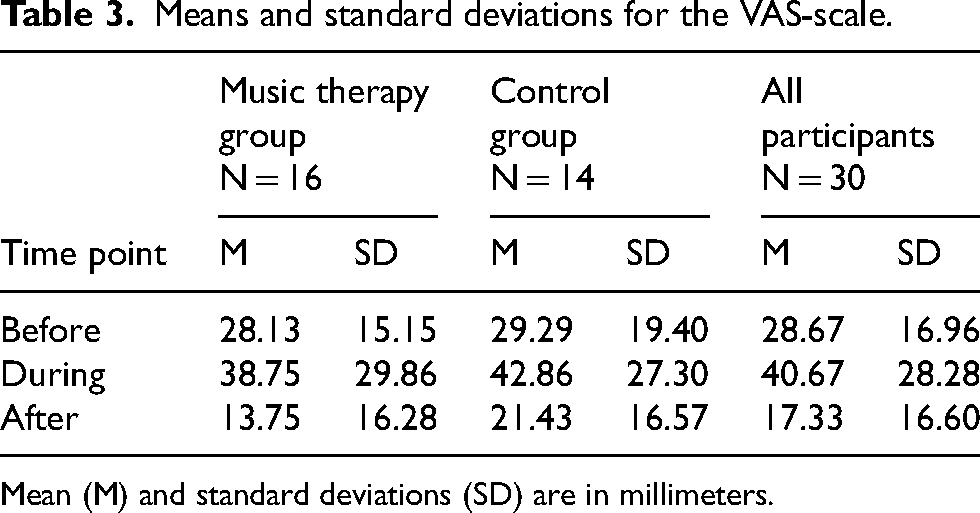
Mean (M) and standard deviations (SD) are in millimeters.
However, when ratings of fear and discomfort at the three time points were compared for the whole group, a significant main effect was found, F(2, 56) = 13.63, p < .001, n2 = .33. All children, independent of group, experienced significantly less fear and discomfort after the procedure than before the procedure, t(59) = 2.98, p = .02, 95% CI [1.62–20.61], and during the needle procedure, t(59) = 4.37, p = .00, 95% CI [9.70–36.73]. There was also a significant difference between before procedure and during procedure, t(59) = 2.91, p = .02, 95% CI [1.53–22.67], with the highest levels of fear and discomfort occurring during the needle procedure. The results show that all children in this sample had a similar pattern of experienced fear and discomfort during the needle procedures. The highest levels of fear and discomfort occurred during the needle procedure and the lowest levels after.
Qualitative Results
Qualitative content analysis (Graneheim & Lundman, 2004) was performed exploring how children and adolescents regulate their emotions during needle procedures while participating in a single music therapy intervention, and how the children, adolescents, and parents perceived the music therapy intervention in this context.
Three themes were identified through the study's qualitative content analysis; i) The music therapy intervention promotes participants’ emotion regulation, ii) The music therapy intervention promotes adaptive coping strategies, and iii) The music therapy intervention affects context and participation. Figure 2 shows an overview of the themes, categories, and codes in the interview study. All three themes relate to the biopsychosocial perspective (Engel, 1977), as they touch upon physiological, psychological, and social mechanisms that influence the children's and parents’ experiences of the music therapy intervention as a whole. The participants’ quotes from the interviews illustrate the different themes. To maintain anonymity, the children's quotes (C1–C8) and parents’ quotes (P1–P15) were anonymized. The quotes have been translated from Swedish to English.

Overview of the themes, categories, and codes in the interview study.
Theme Number One
The Music Therapy Intervention Promotes Participants’ Emotion Regulation
The first theme covers children's and parents’ experiences of the music therapy intervention. During the procedures, the participants perceived that the music therapy intervention strengthened them to deal with their fear and discomfort. Some children and parents experienced that the music therapy intervention could promote adaptive emotion regulation strategies during venepuncture. The music therapy intervention promoted the participants’ ability to express themselves both verbally and non-verbally, and also participate actively in the intervention, which may contribute to the development of self-efficacy. Children and parents described that the music therapy intervention enabled relaxation and increased feelings of calm. I think most people should have this option. The best thing about music therapy is that it's fun, that's good, and it calms you down. Most people might not think about music this way. (C1) Yes, the music absolutely has an effect. Everything becomes like… there's tension released immediately. It's a bit like that when you come to a hospital - it's a very serious place. (P1) Mom usually has to hold down the shoulder, hold my arm. This time she did not need to do that. The music makes it easier. (C2) I could just sit over there… and still feel that my child could handle the situation on her own… And that was enjoyable and very relaxing. (P2) I felt as if you did not even need me there; but more like: ‘Now I’ll play my instruments’. (P3) This was the first time my child participated in music therapy during venepuncture and he was not as upset as he usually is during needle procedures. (P4) I started laughing and then it was just great. (C3) I dare say, if I won’t have any more examinations from now on, I would think that this was probably the most enjoyable visit I’ve ever had in all my hospital visits. This was really the best. (C4)
Theme Number Two
The Music Therapy Intervention Promotes Adaptive Coping Strategies
The second theme illuminates children's thought patterns and associations, ability to be present in the moment and use selective attention. These coping strategies address children's and parents’ need for psychological and social safety and create positive memories for future visits. Children and parents described experiencing the music therapy sessions as evoking a feeling of safety through associations and pleasant emotions. The music signified safety. My child recognised the music from nursery, which calmed him down and brought about a feeling of being safe. (P5) Although this is a new environment and situation, the music is still familiar and safe. (P6) I think it will affect my future visits; I will still remember that I had a fun time here. (C5) The music therapy intervention was a good investment. Not just for this visit but also for future visits, kind of: ‘last time it was great fun’. (P7) Dad knows the drill now. Mom administers the venepuncture and dad manages the music. (P8) When he gets completely stressed out, it's like nothing breaks through, but the music therapy intervention might have been able to reach him. (P9) She did not get completely blocked or closed, she still wanted to interact and play the instruments. (P10) Well, I felt the prick, but it did not bother me, I wanted to continue playing the instruments. (C6) The music therapy changes how I perceive the prick, I mean I feel the prick and it feels like it usually does but I was more focused on what I was playing. I did not worry about the prick because I cared more about what I was engaged in. (C7)
Theme Number Three
The Music Therapy Intervention Affects Context and Participation
The third and last theme includes the descriptions of and perspectives on how the music therapist and music therapy positively transformed the atmosphere in the examination room and improved the healthcare examination as a whole, as well as the social and psychological relationships between the individuals present in the examination room. In this theme, the participants also expressed how the music therapy and feelings of control over musical actions promoted a sense of agency, enabling interaction and participation for the whole family. In addition, the relationship between the music therapist and the children was perceived as contributing to a more light-hearted mood. It affected the atmosphere in the room from the very first second and it immediately felt cheerful. (P11) During venepuncture, she looked at me with an expression like ‘should I be happy or sad?’. So, I’m convinced that the music therapy intervention was influential (P12) It was pleasant to be involved and take part in it, and to dance to the music. (P13) When the music therapist laughed, I also started laughing. (C8) During the venepuncture, you might need to talk about what is going to happen in order to prepare yourselves and the child, and the music might interfere with this, turning the examination into a ballyhoo, even though we know it's not. (P14) The intervention confused me; I ended up being a mix of both an entertainer and a parent. (P15)
Discussion
This mixed methods study tested the effect of combined music therapy and standard pharmacological care compared to standard care alone on fear and discomfort in children in connection to a scheduled needle procedure. Children and their parents were also interviewed on their general experience of music therapy and how they regulated fear and discomfort during needle procedures while participating in music therapy. There were no statistical differences measured with the VAS between the music therapy intervention group and the control group, indicating that the two alternatives were equivalent with regard to experienced fear and discomfort. The content analysis of the interviews indicated that the children and their parents considered that the music therapy intervention promoted the participants’ emotion regulation, promoted adaptive coping strategies for both children and the parents, and favorably but also ambivalently affected the context and interactions in the procedural room.
The Visual Analogue Scale Assessment
In this study, children were recruited regardless of their level of needle fear. Based on previous research estimating that a majority of children fear needle procedures (Constantin et al., 2023; Taddio et al., 2022), we expected high VAS-ratings of fear and discomfort among the participants in our study. Unexpectedly, in our sample, the children included did not report high levels of fear prior to the procedure. This raises the question whether the VAS was a reliable measure in this context. This question is also relevant to ask when the VAS- ratings are compared to the qualitative findings in the interviews and to observations of the children in the videos. The children showed strong emotional reactions during the needle procedures even though they scored relatively low on the VAS-measurement. The parents also described that their children experienced intense emotions in the situation. Taken together, the results are therefore somewhat contradictory.
The generally low VAS-scores could also reflect the pediatric setting's quality of standard care, which aside from the pharmacological treatments already includes a repertoire of effective non-pharmacological supportive options. Still, music therapy proved to be as effective as these supportive options. This might raise the question why music therapy is needed when other effective non-pharmacological options are already available. However, one solution does not fit all children, and combining multiple biopsychosocial fear-reducing strategies has the best effect (Birnie et al., 2018). This means that including music therapy in needle procedures that produce fear and pain expands the repertoire of effective strategies for emotion regulation for children in these situations.
Biopsychosocial Indications
The biopsychosocial perspective (Engel, 1977) was chosen as a relevant theory and framework for the qualitative analysis. Music therapists work within a biopsychosocial framework (Bradt et al., 2015), engaging human beings in reciprocal communication, sharing and partaking through singing, musicking, and improvising. The results from the analysis of the interviews suggested that music therapy as procedural support primarily promoted and facilitated biopsychosocial responses such as relaxation, emotion regulation, coping skills, and positive social interactions in the participating families in connection to the needle procedures. Based on previous research, the goal of the music therapy intervention in the study was to minimize distress while maximizing coping skills (Turry, 1997). In music therapy the therapist can create music which will support the child's unique coping style (Turry, 1997), as well as creating a safe, containing atmosphere (Loewy, 1999). Consistent with previous research (Cousin et al., 2022; Swedberg Yinger, 2016), the parents in this study expressed how the music therapy intervention relieved stress, and increased the children's ability to relax and even have fun during the procedure. Including parents in improvisational music making can alleviate stress and promote positive and enjoyable interactions in the procedure room (Turry, 1997). How children remember their hospital visits can have a lasting impact on their future health behaviors, development of fears (e.g., needle phobias), and avoidance of medical care into adulthood (Noel et al., 2017).
However, the qualitative results from the interview study also disclosed that some parents reported an ambivalence regarding the music therapy intervention being present during the needle procedure describing music therapy as different, confusing, or disturbing. Music therapy was something that these families had never experienced before within a healthcare context. In this pediatric outpatient unit, children, adolescents, and their parents are not separated. The parents’ presence during procedures is considered best practice and part of the clinic's routines. Parents play an important role in facilitating their child's adaptive coping of fear, pain, and discomfort. Still, during needle procedures, certain parents use behaviors that are less attuned with their child's needs, which may be contingent on the parents’ own emotion regulation capacity (Constantin et al., 2022). A careful pre-procedural assessment is crucial for the outcome of the music therapy intervention. Age, gender, diagnosis, culture, past experiences of procedures, and past traumas, as well as the benefits or disadvantages of including parents during the procedure, are among the critical factors in pain assessment (Loewy, 2019). Some parents in this study could have benefitted from detailed information on how music therapy can contribute to supportive strategies for both the parent and the child. Offering psychoeducation and coping strategies separately in advance for some parents might ease these parents’ own stress and enhance the parents’ own emotion regulation capacities in connection to their child's needle procedure. With a short preparatory interview, the music therapist could have tracked the families’ own operative coping strategies when implementing the intervention.
The participants in this study mentioned that the music altered the child's perception of time and place (cf. Sanfi, 2012). In the interviews, the participants expressed that the music therapy intervention helped the children focus on the musical interactions, possibly strengthening the children's ability for selective attention. When the child loses her/himself in the music, the fear and the discomfort related to a painful experience may be reduced and the child remains in a communicative state open to comply and learn coping strategies (Cousin et al., 2022). However, as we saw in the study, some children are helped by observing and engaging in the needle procedure to feel in control (Loewy, 2019). Several parents reported that their children recovered faster and that they were more approachable after the procedure compared to similar previous procedures. This experience is not statistically confirmed in the quantitative data. There was however, a non-significant trend of lower levels of fear and discomfort for the music therapy group after the needle procedure compared to the control group. This could indicate a faster recovery for this group.
Limitations and Strengths
Several limitations of this study warrant further discussion, one being the power calculation. The power calculation was based on previous studies recruiting only children with high levels of needle fear. For feasibility reasons, this study chose to recruit all children who had a needle procedure planned during the period of data collection. This may have affected the possibility of identifying statistically significant differences in our sample.
Another limitation is related to parents’ ability to rate level of emotions in their children accurately. For the younger children (age 0–4) in this study, parents rated their child's levels of fear and discomfort on the VAS. This might have influenced the scoring for these children, making the results less reliable.
In this study, the children and their parents were interviewed together, which meant that the parents heard the children's answers and vice versa, and both parties could influence each other's responses. This might have affected the trustworthiness and authenticity of the answers, depending on how attuned the parents were to their child's opinions and emotions. However, this was a considered choice as the focus for the interviews was to investigate the child's and the parent's shared experiences of the music therapy intervention and its potential to regulate the dyad's emotions. The study design also took into consideration the risk for exacerbating a potential procedural trauma by separating the child from its parent directly after the procedure for the interviews. In addition, the interview design complied with the family-centered policies and routines in the pediatric outpatient unit where parents or another next of kin always are present with the child during the procedures. The key strength of the interview study was that the older children reported their own feelings and actively participated in the interviews, making the findings a valid contributor of children's own opinions and experiences of music therapy as procedural support to future research.
It can be considered a weakness that the interviews were relatively short and thus perhaps not exploratory enough. However, many families had limited time after the needle procedure before their next healthcare examination, and too long interviews would have limited their ability to participate. The length of the interviews was adapted to the children's age and attention span, which can also be considered a strength.
Although randomization minimizes the selection bias, blinding of the nursing staff, interventionists, and participants to group allocation during data collection was not possible due to the nature of the intervention. However, the interventionists ensured that the two allocation groups were, apart from the music therapy intervention, treated as equally as possible to prevent differential treatment of the groups. To prevent biased assessment of outcomes, only the two psychology master students performed the primary analysis.
To ascertain differences in the demographic data between intervention group and control, Pearson's chi-squared test was used. However, the choice of Pearson's chi-squared test is problematic when the sample size is small, as in this study (McHugh, 2013). This might have contributed to pre intervention differences between the control group and the intervention group not being detected.
The data collection took place during the COVID-19 pandemic, which meant that nurses, the music therapist, and researchers had to wear both face masks and visors. The children might have had difficulties in perceiving facial expressions behind the visors and masks, consequently increasing the risk for hampering the interpersonal and the musical interactions with the children and their parents.
Implications for Clinical Practice
As a real-life clinical research project, this study has ecological validity with results that can be generalized to and safely implemented in pediatric outpatient settings in Swedish health care. The music therapy intervention was flexible and aimed at meeting the individual needs of the participants, which enabled inclusion of all children, including children with various health difficulties, functional diversities, and diagnoses.
This study only focused on the period of time immediately before, during, and after the procedure. When providing procedural support, it is important for music therapists to be mindful of the families’ time constraints, particularly for those receiving care in outpatient settings. However, a thorough procedural preparation and assessment, along with information on the rationales for including music therapy strategies in this context, which some parents in the study requested, is essential for the outcome of the music therapy intervention (Loewy, 2019). The core principle in procedural comfort care is for the child and parent to be well regulated before the needle procedure (c.f. Leroy et al., 2016). The music therapist should therefore prioritize procedural preparation and procedural assessment prior to the procedure and then tailor the music therapy intervention accordingly.
Implications for Further Research
Research must continue to address the under-prioritization of fear and pain management in pediatric healthcare settings since the majority of children are still afraid of needles (Taddio et al., 2022). This area of research is difficult to investigate. To assess, measure, and systematically capture multisensory, biopsychosocial, and ambiguous phenomena as fear, pain, music, and music therapeutic interactions, there is a need of more comprehensive research tools. Mixed methods designs are recommended in music therapy research because of the possibility of elucidating the studied phenomena from multiple perspectives (Bradt et al., 2013). To acquire a more exhaustive knowledge of music therapy as a non-pharmacological treatment during needle procedures, and the biopsychosocial impact of music therapy interventions, future research might consider measuring the child's and the parent's heart rate variability as a psychophysical marker of emotion regulation (Constantin et al., 2022), as well as using skin conductance monitoring to discern changes in electrical (ionic) activity resulting from changes in sweat gland activity in response to sensory stimuli (Savino et al., 2013).
Given the essential role of parents in children's experience of needle-related fear and pain, and the parents’ presence during these procedures in the Swedish pediatric context, a participatory music therapy research project in collaboration with pediatric staff and child life specialists, parents, and children, would be of interest. Potentially, music therapeutic psychoeducation could contribute with long-lasting procedural coping strategies for the whole family.
Conclusion
This is the first study in a Swedish pediatric outpatient setting to investigate the effects on fear and discomfort of music therapy as procedural support for children and their parents. The study also explored children's and parents’ perceived emotion regulation during needle procedures while participating in music therapy and their experiences of a single music therapy intervention.
There were no statistical differences measured with the VAS between the music therapy intervention group and the control group, indicating that the two alternatives were equivalent with regard to experienced fear and discomfort. Children and their parents expressed that the music therapy intervention promoted the participants’ emotion regulation, promoted adaptive coping strategies for both children and the parents, and that the music therapy intervention favorably but also ambivalently affected the context and interactions in the procedural room. In conclusion, for most families in this study, the music therapy intervention promoted integration, creating a safe and trusting atmosphere during the needle procedure through interactive participation. Combining multiple biopsychosocial fear-reducing strategies has the best effect. Therefore, it is important to expand knowledge about music therapy as an evidence-based family-centered non-pharmacological supportive option.
Footnotes
Acknowledgments
Our warmest thanks to all the study participants and health professionals at the Paediatric outpatient unit at the Central Hospital in Karlstad, Region Värmland, Sweden. Thank you Centre for Clinical Research and Education, Region Värmland, Sweden for financial support.
Action Editor
Orii McDermott, University of Nottingham, Institute of Mental Health, School of Medicine.
Peer Review
One anonymous reviewer.
Jane Edwards, University of New England, Faculty of Humanities, Arts, Social Sciences and Education.
Contributorship
AKS, EL, and AU researched literature, conceived the study, and administrated participant recruitment. AKS, EL, AU, and SE were involved in study design, gaining ethical approval, and data analysis. AU wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Swedish Ethical Review Authority (Dnr 2021–07020-01) and was a research collaboration between Örebro University and Region Värmland, Sweden.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Paediatric Clinic at the Central Hospital in Karlstad, Region Värmland, Sweden, Centre for Clinical Research and Education, Region Värmland, Karlstad, Sweden.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.