
Abstract
Most of the critically ill novel coronavirus 2019 pneumonia (NCP) patients progress promptly, and soon match the ARDS diagnostic criteria. When mechanical ventilation and prone position cannot reverse the fatal hypoxia—extra-corporeal-membrane-oxygenation (ECMO) will be applied as a salvage treatment if available. Here, we report a novel coronavirus 2019 pneumonia (NCP) patient, a male, 67 years old, who was treated with ECMO for 30 days. In the midst, bronchoscopy was utilized to comprehend the airway lesions and clear secretions. And computed tomography (CT) scans were performed before and after the treatment of ECMO. In the recovering phase of his disease, the patient experienced multiple times pneumothorax on both sides. Some newly developed lung bullae in the subpleural area and modest bronchiectasis were found by the CT scan. The newly developed lung bullae was the probable cause of pneumothorax. Notably, in the whole process of his illness, the serum IL-6 only had a slight elevation in the early period, there is no typical cytokine storm as that was seen in non-COVID-19 ARDS. After 3-months meticulous treatment, the patient made a full recovery and now is discharged from our hospital. Though COVID-19 may not cause typical cytokine storm, the inflammation in lung may inflict severe damage to lung. Severe NCP may cause lung bullae and bronchiectasis, making the patients hard to be weaned from mechanical ventilation or ECMO.
Keywords
Introduction
Most of the critically ill novel coronavirus 2019 pneumonia (NCP) patients progress promptly, and soon match the ARDS diagnostic criteria. 1 In NCP with moderate or severe ARDS, mechanical ventilation, prone position, and some other supportive measures are regularly needed. But severe type NCP usually doesn’t respond well to these treatments, so the mortality rate for patients so afflicted is high. A retrospective study showed that the mortality rate of acute respiratory distress syndrome (ARDS) complicated NCP was 52.4%. 2 When mechanical ventilation and prone position cannot improve oxygenation—extra-corporeal-membrane-oxygenation (ECMO) will be applied as a salvage treatment if available.3,4 But still, many patients died of multiple organs dysfunction due to their lung function didn’t recover during the ECMO treatment. Here, we report an NCP patient who was treated with ECMO for 30 days. In the midst, bronchoscopy was utilized to comprehend the airway lesions and clear secretions. And computed tomography (CT) scans were performed before and after the treatment of ECMO. Some interesting and meaningful findings were found by these measures.
Materials and methods
Ethical approval and consents for participation and publication
The treatments we performed were approved by the Administrative Panel for Medical Research on Human Subjects of The First People’s Hospital of Foshan. Patients’ family members granted consents for participation and publication in written form and can be requested at any time. Consent for publication was obtained from the patient’s family members before he made the full recovery from COVID-19. In that period he was intubated and intermittently sedated, which compromised his ability to provide the informed consent.
The aim, design, and setting of the study were not applicable, as only standard treatments were applied.
Case presentation
A 67 years old male, who has a long history of smoking and 10 years of mild COPD was admitted to our department on Feb 6th. He traveled to Vietnam from Jan 19 to 24, 2020, along with many tourists from Wuhan city. On January 26th (D1), he experienced the onset of fever, chills, dry coughs, headache, and fatigue. These symptoms were mild, the patient took it as a common cold, and was self-quarantined at home. On February 4th (D10), he started to have short of breath. After the COVID-19 virus nucleic acid was detected positive and diagnosed with NCP in the local hospital, he received the following treatments, including anti-viral (Arbidol 0.2 g tid, Lopinavir 200 mg + Ritonavir 50 mg bid), anti-bacterial (Cefoperazone sodium sulbactam sodium 3 g tid), and high flow nasal cannula (HFNC) oxygen therapy (45–60 L/min) 5 ; but his signs and symptoms were not attenuated. Hence, on February 6th (D12), the patient was transferred to our hospital and admitted to our department. Though he was treated with HFNC and noninvasive ventilation, his dyspnea was not relieved but accompanied by persistent high fever. The main treatments timeline was shown in Figure 1. On February 11th (D17), when his oxygenation index was only 126 mmHg after 8 h noninvasive ventilation, he received intubation and lung protective ventilation (LPV). In spite of lung recruitment maneuver (RM) and 16 h/day prone position, his oxygenation showed no improvement, whereas his CT imaging (D29) opacity increased dramatically, the images were exhibited in Figure 2(A). On February 28th (D34), as his oxygenation index was only 57.7 mmHg while his PEEP reached 15 cmH2O, he received veno-venous (VV) ECMO treatment (blood flow 4 L/min, gas flow 7 L/min, and Fi O2 100%). A subsequent bronchoscopy detected secretions attached superficially to the distal bronchi, mixed with a little white-hyaline mucus; also, solid particulates could be detected in the BALF after it was placed in a vessel and allowed to stand for several minutes, the pictures of BALF and sputum were presented in Figure 3. After treating with LPV and VV ECMO for 30 days, his condition had an obvious improvement and he was weaned from ECMO on Mar 28th. What’s bewildering us was that in the recovering phase of his disease (between the middle to late of March, 2020), the patient experienced multiple times pneumothorax on both sides. He was treated with thoracic close drainage, but the Mar 29th CT detected that the gas in his thoracic cavity was not completely absorbed (seen in Figure 2(B)). However, the exudation and inhomogeneity were reduced significantly when compared with the previous CT scan (performed on Feb 23th). Interestingly, some newly developed lung bullae in the subpleural area and modest bronchiectasis were found by the CT scan, the former was the probable cause of pneumothorax; while the latter may indicate that severe NCP not only damage the bronchi mucosa, but also the bronchi structure. Of note, in the entire process of his illness, the serum IL-6 only had a mild elevation in the early period. The findings in this case may suggest that serious damage to pulmonary parenchyma caused by severe NCP may induce pulmonary complications such as lung bullae and bronchiectasis. Finally, after 3-months meticulous treatment, the patient made a full recovery and now is discharged.

The main treatments timeline. The main treatment course included antiviral, and respiratory supportive measures such as high flow nasal catheter oxygen therapy (HFNC), noninvasive ventilation (NIV), lung protective ventilation (LPV), and veno-venous extracorporeal membrane oxygenation (VV ECMO). CoVID-19’s RNA was tested by RT-PCR, and the positive results were marked with a plus sign “+.”
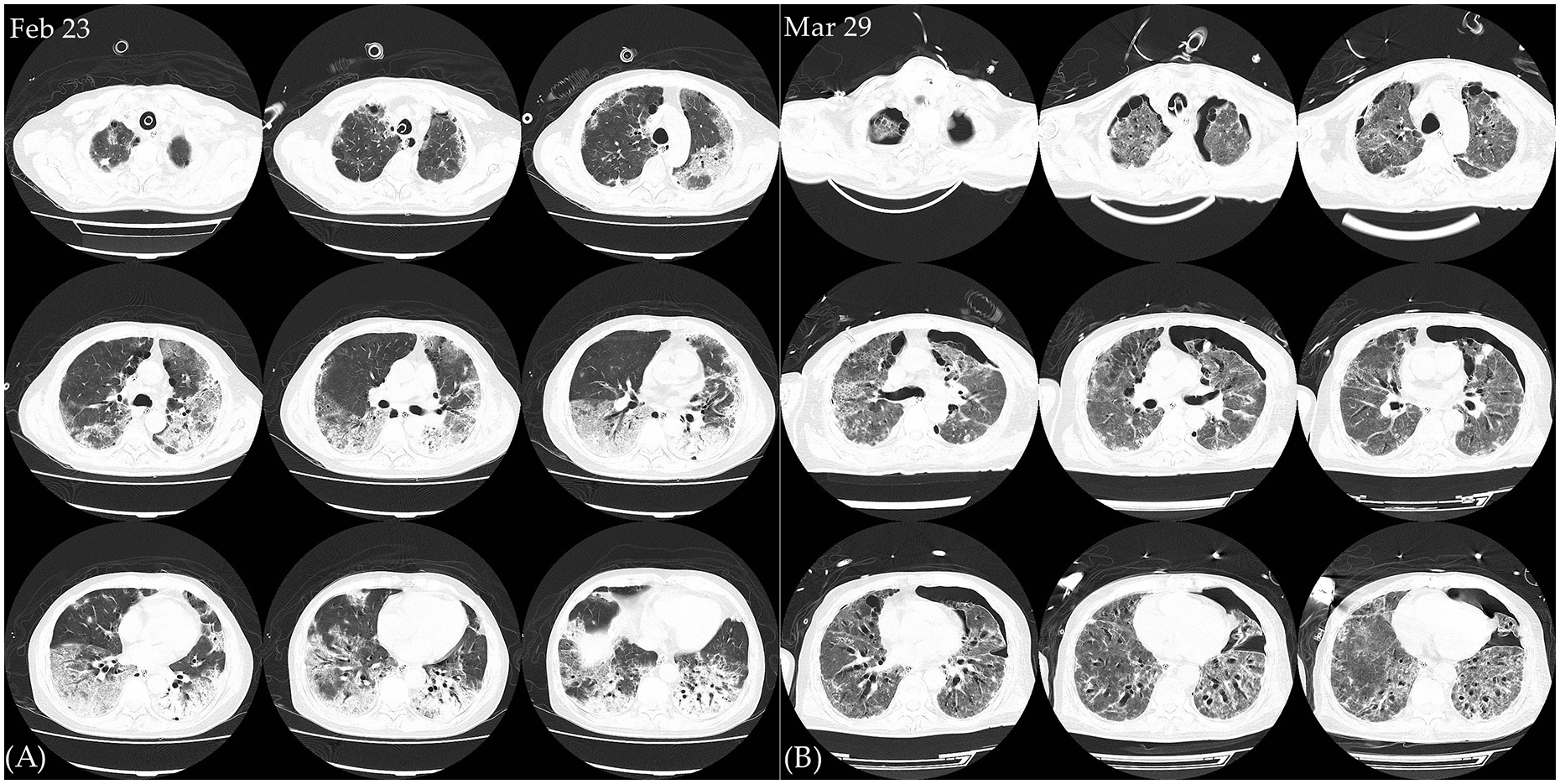
The CT scans of the patient. Two CT scans were performed, on February 23 (before the initiation of ECMO) and March 29 (after the wean of the ECMO) respectively. By CT scans, the exudation and inhomogeneity in lung were found to be reduced significantly after his recovery, but some newly developed lung bullae in the subpleural area and modest bronchiectasis were detected.

The bronchoscopic and BALF macroscopic pictures of the patient. The bronchoscopic checks were performed on February 23, March 4 and March 14 respectively. With the recovery of the patient, the BALF became less bloody gradually.
Discussions and conclusions
During this crisis, a total of 98 NCP patients were diagnosed in Foshan, where there were 12 severely ill and 2 critically ill patients. The patient we reported here was one of the critically ill patients. The patient has a long history of smoking and 10 years of mild COPD, which are predictors of refractory severe NCP. 6 He developed ARDS and received ECMO treatment because his condition was not reversed by regular treatments such as LPV and prone position.
The case herein has several characteristics: (1) The viral pneumonia developed fast, and respiratory failure came swiftly, which was belong to the critical and refractory type viral pneumonia. (2) Since the grade 0–4 bronchi usually didn’t possess much secretion, it easily gave doctors the illusion of only rather limited secretion in the airways. (3) The bronchoalveolar lavage fluid was bloody in the severe phase, suggesting NCP can severely damage the bronchi mucosa. (4) Some newly developed bullae were found in the subpleural area, that’s the probable cause of pneumothorax. (5) Based on the newly developed bronchiectasis and lung bullae, we suspect that severe NCP may not only damage the bronchi mucosa, but also the bronchi structure and pulmonary parenchyma.
Low tidal volume ventilation and prone positioning in moderate to severe ARDS, both of which have been shown to reduce mortality, now are the mainstay of ARDS management. In this case, low VT ventilation and prone position were administered before the initiation of ECMO. ARDS is known to be a heterogeneous syndrome with different sub-phenotypes depending on different clinical features, inflammatory cytokine profiles and differential response to interventions. COVID-19 induced ARDS also fits this rule, thus individualized and time-evolving treatment is important. In the early course of his illness, prednisone was given to the patient after ARDS was diagnosed. Later the RECOVERY trial that proved early low-dose dexamethasone improves survival in patients with COVID-19, especially among those on mechanical ventilation, supported our clinical judgement. But when flow cytometry showed that his total T lymphocytes counts were reduced significantly, corticosteroids were stopped to prevent fatal secondary infection in the context of potential immuno-suppression. To date, there are no other proven medications for COVID-19 except remdesivir and dexamethasone. 7 However, mesenchymal stem cells which was investigated extensively in recent years might be an eligible candidate.8–11 In the entire course of his illness, the serum IL-6 (62 pg/mL), ferritin (1.21 g/L), and LDH (780 U/L) only had a slight elevation in the early period, there is no typical cytokine storm as that was seen in non-COVID-19 ARDS. The COVID-19 associated thrombosis has been noticed by many clinicians,12,13 heparin was regularly used to prevent thrombosis even after the patient was weaned from ECMO. In extremely severe cases, COVID-19 inflicted lung damage may cause lung complication such as lung bullae and pneumopericardium,14–16 under the circumstance of which the necessity of lung recruitment maneuver should be carefully assessed.
Conclusion
Though COVID-19 may not cause typical cytokine storm, the inflammation of severe NCP may cause lung bullae and bronchiectasis, which consequently may make the patients hard to be weaned from mechanical ventilation or ECMO. Therefore, the prevention of pneumothorax and bronchiectasis should be considered.
Footnotes
Author contributions
WFY and FB contributed equally to this work, they conceived the idea and analyzed the medical file together. The manuscript was translated in English by WFY. CGQ made supportive contributions to this work. ZLX was involved in drafting the manuscript and revising it critically for important intellectual content. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by key medical specialty cultivation project of Foshan.
Ethical approval and consent to participate
The treatments we performed were approved by the Administrative Panel for Medical Research on Human Subjects of The First People’s Hospital of Foshan. Patients’ family members granted consents for participation and publication in written form and can be requested at any time.
Informed consent
Consent for publication was obtained from the patient's family members before he made the full recovery from COVID-19. In that period he was intubated and intermittently sedated, which compromised his ability to provide the informed consent.
Consent for publication
Consent for publication was obtained from the patient's family members before he made the full recovery from COVID-19. In that period he was intubated and intermittently sedated, which compromised his ability to provide the informed consent.
Availability of data and material
The datasets used and/or analyzed in this study are available from the corresponding author on reasonable request.