
Abstract
Early clinical stability has been proven to be vital for the treatment of community-acquired pneumonia (CAP). This research retrospectively analyzed the predictive implication of neutrophil–lymphocyte ratio (NLR) and confusion, urea >7 mmol/L, respiratory rate ⩾30 breaths/min, low blood pressure, and age ⩾65 years (CURB-65) score to predict early clinical stability of the adult CAP. Clinical data, CURB-65 scores, pneumonia severity index (PSI) scores, NLR on admission (within 24 h) of 230 patients between January 2012 and June 2015 were obtained from the Affiliated Hospital of Chengdu University. Instable patients had significantly higher CURB-65, PSI, white blood cell (WBC), neutrophil, and NLR than the stable patients (P < 0.05); NLR was positively correlated with CURB-65 (r = 0.270, P < 0.001) and PSI (r = 0.316, P < 0.001). NLR and CURB-65 were screened as risk factors through the discriminant analysis. The area under the curve (AUC) was 0.662 (95% confidence interval (CI): (0.569, 0.756), P = 0.002) for NLR, 0.670 (95% CI (0.569, 0.772) P = 0.001) for CURB-65. The enhanced predictive power was observed for combining NLR-CURB-65 with the AUC of 0.704 (95% CI (0.606, 0.802), P < 0.001). The risk of early clinical instability rose significantly in patients with NLR (odds ratio (OR) = 3.440, 95% CI (1.741, 6.798) with the cut-off value of NLR = 6.161) and higher CURB-65 (OR = 3.797, 95% CI (1.801, 8.005), with the CURB-65 cut-off value of 1.5). Both NLR and CURB-65 are qualitatively accurate for predicting early clinical stability of CAP, an accuracy-enhanced predicting power was observed in the NLR-CURB-65 combined test, further large-sample studies are required to validate the conclusion.
Introduction
Community-acquired pneumonia (CAP), a common pneumonia disease caused by bacteria, viruses, and other organisms, is becoming a global healthcare concern. 1 CAP is the eighth leading cause of death in the United States, with more than 1.5 million adult patients hospitalized annually, and nearly 100,000 deaths were caused during hospitalization. 2 In China, the control situation of CAP is not optimistic because of the high proportion of hospitalized patients in recent years. 3 There are many factors affecting the outcome and prognosis of CAP, of which early clinical stability is proven to be vital for the disease control. 4 In recent years, the significance of clinical easy-to-use index to the disease diagnosis, treatment, and prognosis has aroused attention. Several international guidelines in clinical practice have recommended confusion, urea >7 mmol/L, respiratory rate ⩾30 breaths/min, low blood pressure and age ⩾65 years score (CURB-65) and pneumonia severity index (PSI), the two most-respected clinician-administered scales for estimating CAP in patients. 5 Since systemic inflammation of CAP happens during the peripheral blood changes, for example, changes in neutrophils and lymphocytes, peripheral blood examination is also considered as a common indicator for assessing the condition of CAP patients on admission and for covering pathogens. To guide antibiotic regimen, both the neutrophils and lymphocytes constituting neutrophil–lymphocyte ratio (NLR) are easy-to-use and easy-to-measure indices with economic efficiency and fastness, which can be easily applied in all levels of medical institutions, including the primary care hospitals. 6 These two are probably capable of measuring inflammatory response in acute infection which are the likely candidates related to early clinical stability. However, there is limited evidence of the relation between admission NLR, CURB-65 score, and early stability of CAP. The aims of this study were to investigate whether there is a correlation between the level of CURB-65, NLR, and early clinical stability and to find or define the best cut-off point for CRUB-65 and NLR, enabling the absence of early stability after 72 h of admission to be identified.
Materials and methods
General data
This study is a retrospective study of adult CAP patients admitted to the department of respiratory and critical care medicine at Affiliated Hospital of Chengdu University. Data of patients diagnosed with CAP were collected by the electronic medical record (EMR) system between January 2012 and June 2015. The information including demographic information, clinical symptoms, treatments, CURB-65 scores, PSI scores, laboratory tests, and NLR (on admission, within 24 h) was collected. The study was approved by ethic community of the Affiliated Hospital of Chengdu University (ID: PJ2018-011-02).
Inclusion and exclusion criteria
Inclusion criteria
The Guidelines for the diagnosis and treatment of CAP by the Chinese Thoracic Society in 2006 served as the standard basis: 7 (1) recent onset of cough or expectoration or aggravation of existing symptoms of respiratory tract diseases, with or without purulent sputum, chest pain, dyspnea, or hemoptysis; (2) fever; (3) signs of pulmonary consolidation and/or moist rales; (4) peripheral white blood cell (WBC) count >10 × 109/L or <4 × 109/L, with or without a left shift; and (5) chest radiograph showing new patchy infiltrates, lobar or segmental consolidation, ground-glass opacities, or interstitial changes, with or without pleural effusion. The presence of at least one of criteria 1–4 plus 5, except for tuberculosis, lung cancer, non-infectious pulmonary interstitial disease, pulmonary edema, atelectasis, pulmonary embolism, pulmonary eosinophil infiltration, pulmonary vasculitis, etc.
Exclusion criteria
(1) age <18 years; (2) presence of other respiratory diseases, for example, tuberculosis and lung cancer; (3) hospital-acquired pneumonia; (4) immunosuppressive therapy, chemotherapy and radiotherapy within 2 months, and acquired immune deficiency syndrome; (5) duration of 14 days or more, hospital stay less than 3 days; (6) pregnant and lactating women; (7) psychiatric disorder or mental retardation affecting mental status examination; and (8) antibiotic therapy prior to the present admission. 7
Definition of early clinical stability
The early clinical stability of patients at 72 h after initial therapy was performed in line with the criteria of the Infectious Diseases Society of America/American Thoracic Society Consensus Guidelines on the Management of Community-Acquired Pneumonia in Adults (2007) by the American Thoracic Society/Infectious Diseases Society of America (ATS/IDSA): 2 (1) temperature ⩽37.8°C; (2) heart rate ⩽100 bpm; (3) respiratory rate ⩽24 bpm; (4) systolic blood pressure ⩾90 mmHg; (5) SaO2 ⩾90% or PaO2 ⩾60 mmHg on room air; (6) ability to maintain oral intake; and (7) normal mental status. Besides, patients satisfying any one of the criteria were considered clinically stable. Patients died or discharged against medical advice within 72 h of admission were regarded as clinically instable as well.
Statistical methods
IBM SPSS Statistics 24.0 for Windows, version 24.0. (Armonk, NY: IBM Corp.), was employed for statistical analysis here, and variables are denoted as mean ± standard deviation (SD) or as frequencies, unless indicated otherwise. The comparison of all continuous variables was drawn by Student’s t-test. The chi-square test was performed to compare proportions and Fishers exact test was performed if appropriate. Pearson’s correlation coefficients were used to characterize the relationship between changes of variables. Collinearity among factors was tested with the variance inflation factor (VIF) test, and the discriminant analysis (with the stepwise method) was performed to screen risk factors. Receiver operator characteristics (ROC) curves were plotted for the CURB-65 and NLR. Results of ROC statistics are reported as area under the curve (AUC) with 95% confidence interval (CI). All tests were explorative and two sided, and the significance level was set to α = 0.05.
Results
Baseline characteristics
A total of 230 adult patients were finally recruited, including 156 men and 74 women (mean age, 69.07 ± 17.42 years; range, 18–95 years). A total of 107 (46.32%) of the recruited patients were smokers. Comorbidities largely included cerebrovascular disease (24 patients), gastroduodenal disease (45 patients), liver disease (12 patients), kidney diseases (33 patients), cancer (5 patients, the diagnoses were multiple myeloma, laryngeal cancer, prostate cancer, esophageal carcinoma, and myelodysplastic syndrome), chronic obstructive pulmonary disease (COPD, 91 patients), hypertension (72 patients), heart failure (41 patients), and diabetes mellitus (31 patients). No significant differences between groups were found in the demographic features, comorbidities, and antibiotic therapy (P > 0.05, Table 1).
Baseline characteristics between groups.

COPD: Chronic obstructive pulmonary disease.
Clinical scores and laboratory tests
For the effects of clinical scores and admission laboratory tests (Table 2), the instable group had significantly higher CURB-65, PSI, WBC, neutrophil, and NLR than the stable group (P < 0.05).
Comparison of clinical scores and laboratory findings between groups.

CURB-65: (confusion, urea > 7 mmol/L, respiratory rate ⩾ 30 breaths/min, low blood pressure and age ⩾ 65 years); PSI: pneumonia severity index; WBC: white blood cell; HCT: haematocrit; HGB: hemoglobin; Hs-CRP: hypersensitive C-reactive protein; Alb: albumin; PCT: procalcitonin; NLR: neutrophil–lymphocyte ratio.
Correlation analysis
Correlation of NLR with CURB-65 (Figure 1(a)) and PSI score (Figure 1(b)). Neutrophil–lymphocyte count ratio (NLR) levels in patients with CAP correlated positively with CURB-65 score (r = 0.270, P < 0.001) and PSI score (r = 0.316, P < 0.001).
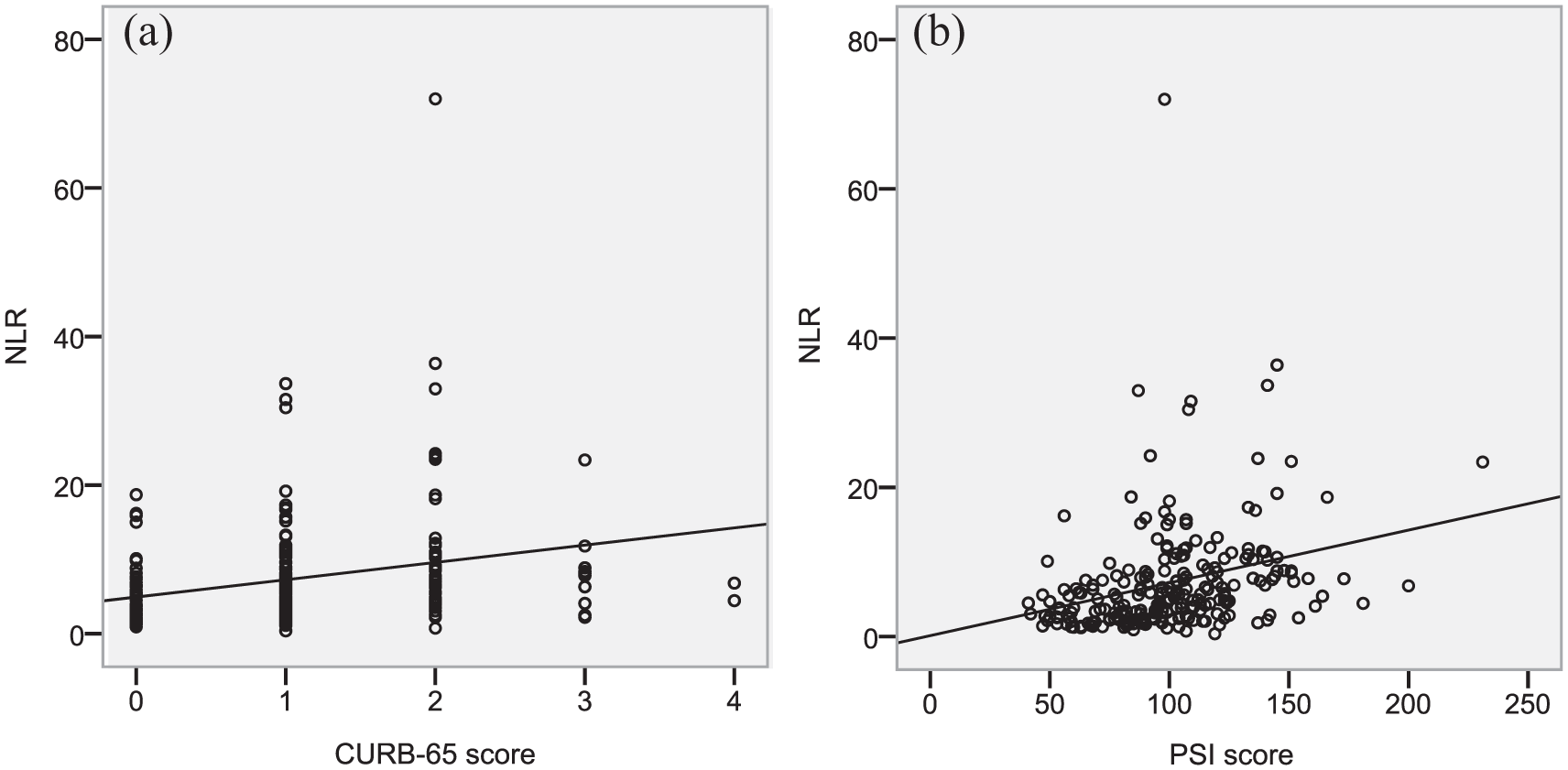
Correlation of NLR with CURB-65 score and PSI score.
Predicting power of NLR and CURB-65
The discriminant analysis (using the stepwise method) was performed to further screen risk factors, and NLR and CURB-65 were finally employed for ROC analysis (Wilks’ lambda = 0.918, x2 = 19.483, P < 0.001), and 71.3% of original cases were correctly classified between the stable and instable group. Both CURB-65 and NLR were statistically significant to predict the early clinical stability, the area under the ROC curve was 0.670 for CURB-65 score (AUC = 0.670, 95% CI (0.569, 0.772), P = 0.001), 0.611, 0.662 for NLR (AUC = 0.662, 95% CI (0.569, 0.756), P = 0.002), the ROC curves for the selected indexes for assessing early clinical stability are listed in Table 3 and Figure 2(a). The enhanced predictive power was observed for the combination of NLR-CURB-65 with the AUC of 0.704 (95% CI (0.606, 0.802), P < 0.001), (Figure 2(b)). ROC curve revealed that an NLR cut-off value of 6.161, the risk of early clinical instability was significantly higher in patients with NLR ⩾6.161 (odds ratio (OR) = 3.440, 95% CI (1.741, 6.798)). With the CURB-65 cut-off value of 2 (cut-off value = 1.5), patients with CURB-65⩾ 2 on admission have significantly higher hospitalization costs, and patients with higher NLR showed the significantly higher risk of early clinical instability (OR = 3.797, 95% CI (1.741, 6.798)).
ROC analysis and cut-off points CURB-65 and NLR.

ROC: receiver operator characteristics; CURB-65: confusion, urea > 7 mmol/L, respiratory rate ⩾30 breaths/min, low blood pressure and age ⩾65 years; NLR: neutrophil–lymphocyte ratio; AUC: area under the curve; 95% CI: 95% confidence interval; LR(+): positive likelihood ratio; LR(–): negative likelihood ratio.

ROC curve of neutrophil–lymphocyte ratio (NLR), confusion, urea > 7 mmol/L, respiratory rate ≥30 breaths/min, low blood pressure and age ≥65 years (CURB-65) and the combined NLR-CURB-65 for predicting early clinical stability of adult community-acquired pneumonia. (a) The ROC curves for single predictors had the following areas: NLR, 0.662 (95% CI: [0.569, 0.756], P = 0.002); CURB-65, 0.670(95% CI [0.569,0.772], P = 0.001). (b) ROC curves for NLR-CURB-65 combined predictors had the AUC of 0.704 (95% CI [0.606, 0.802], P < 0.001).
Discussion
CAP remains one of the most common causes of morbidity and a potentially life-threatening illness in the world. Earlier assessment of patients is vital for successful management. CURB-65, an important clinical score system, has been proven for assessing severity and predicting mortality among patients in patients either hospitalized or admitted to emergency department. 8 Other biomarkers like procalcitonin and hypersensitive C-reactive protein (Hs-CRP) can also be considered as a potential factor for predicting CAP outcomes. 9 Routine peripheral blood test, one of the most commonly used measures for disease diagnosis, has long served as critical indicators for determining the severity of inflammation. Neutrophil-mediated and lymph-mediated lung damage have been verified capable of determining the outcome of infection, and NLR, a combination of neutrophil and lymphocytes, is naturally required. Previous studies have demonstrated the clinical implication of NLR as diagnostic or prognostic indicators of various diseases, for example, lung cancer, 10 pulmonary embolism, 11 and COPD. 12 Nevertheless, none of these studies have stressed the predictive implication of NLR as an easy-to-use admission index in assessing early clinical stability of adult CAP. In this study, the significance of NLR and other two indexes to the early clinical stability of CAP was analyzed to explore the value of NLR for assessing the early clinical stability of CAP. By the primary analysis, significant differences between stable and instable groups were found in CURB-65 score, PSI score, WBC, absolute neutrophil count (neutrophil), and NLR. Furthermore, NLR was found positively correlated with CURB-65 score and PSI score, and according to predictive accuracy tests by ROC curve, CURB-65 score, PSI score, WBC, neutrophil, and lymphocyte could be potential markers in assessing early clinical stability. Besides, CURB-65 score (AUC = 0.670) and NLR (AUC = 0.662) were verified to outperform PSI (AUC = 0.611), WBC (AUC = 0.611), and neutrophil (AUC = 0.623). The enhanced predictive power was observed for the combination of NLR-CURB-65 (AUC = 0.704), better than the combination of NLR-PSI (AUC = 0.658). However, compared with NLR-CURB-65 combined test, a greater predictive power was not observed for the combination of NLR-CURB-65-PSI (AUC = 0.704).
In conclusion, the present research suggests that NLR (an index easy to use and measure) and CURB-65 (a score system easy to measure) on admission are qualitatively accurate for the prediction of the early clinical stability of CAP, and further large-sample studies are required to validate the conclusion.
Footnotes
Acknowledgements
X.J. and S.T. contributed equally to this work and share joint first authorship. The authors thank standardized medical residency training doctors Yao Wang, Xu Zhang, and Wei Xu for their support and help of data collection in the research. Design: X.J. and Q.Z.; data collection: X.J. and S.T.; data analysis: H.Z., and Q.Z.; project administration: Q.Z.; writing the original draft: X.J.; and writing the review and editing: X.J., H.Z., and Q.Z.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Programs of the Health Commission of Sichuan Province (grant no.: 17PJ052; 18PJ405), the Program of Sichuan Medical Association (grant no.: S16002), and the Program of Sichuan Educational Committee (grant no.: 16ZB0426).