
Abstract
Objective
In this study leukocyte, lymphocyte, neutrophil, platelet count, mean platelet volume (MPV), neutrophil/lymphocyte (NLR) ratio and platelet/lymphocyte ratio (PLR) were retrospectively evaluated in patients with idiopathic acute anterior uveitis.
Materials and methods
Medical records were retrospectively reviewed from March 2016 to February 2020. Fifty patients (25 men and 25 women) and as the control group, 50 healthy volunteers (25 males and 25 females) were included in this study. Blood samples of the patients were taken before starting treatment. A complete ophthalmological examination, including corrected visual acuity, tonometry, slit lamp and fundus examination, was performed in all patients. Gender, age, leukocyte, neutrophil, lymphocyte, platelet, MPV, PLR, and NLR values of the patients were recorded.
Results
In this study, a statistically significant difference was found in leukocyte (p < .001), neutrophil (p < .001), platelet (p < .001), NLR (p < .001) and PLR (p < .001) values. No significant difference was found between the two groups in terms of lymphocyte count (p = .063) and in the MPV value (p = .051). Leukocyte, neutrophil, platelet count, NLR, and PLR values were higher in the uveitis group compared to the control group. In the receiver operating characteristic (ROC) curve analysis, the area under the curve (AUC) for NLR was 0.805, with a sensitivity of 56.0% and a specificity of 98.0%. The AUC for PLR was 0.657, with a sensitivity of 52.0% and a specificity of 98.0%.
Conclusion
In this retrospective study, leukocyte, neutrophil, platelet count, PLR, and NLR levels were significantly higher in patients with idiopathic acute anterior uveitis compared to the control group. These blood parameters are useful as diagnostic markers and can be used in early diagnosis.
Introduction
Uveitis is an inflammation of the uvea, the middle vascular layer of the eye. It is an important cause of blindness and low vision. It may occur at any age, most commonly between the ages of 20–59. The incidence in the community is 17–52/100,000 per year.1,2
Uveitis is divided into groups according to its localization; anterior uveitis (involves the iris and ciliary body), intermediate uveitis (vitreous, pars plana of the ciliary body and peripheral retina), posterior uveitis (choroid and retina), panuveitis (generalized inflammation of the entire uvea).3–5 In most cases, the causes of anterior uveitis cannot be found. Uveitis in this group, defined as idiopathic anterior uveitis, constitutes 38-88% of all anterior uveitis. It is the most common form of uveitis in the community.5,6
The underlying mechanisms causing acute anterior uveitis are unknown. It has been reported that immune complex and cell-mediated autoimmune processes may be responsible. 7 Since the middle of the last century, with the development of laboratory techniques used to diagnose uveitis, the etiology of uveitis has become more pronounced. 8 The association of systemic diseases with uveitis is known. The frequency of systemic disease underlying uveitis is 19–46%.3,4 In recent studies, it has been reported that white blood cells, neutrophils, neutrophil/lymphocyte ratio, and platelet/lymphocyte ratio can be easily counted in whole blood count and used as an inflammation biomarker in subclinical systemic inflammation. Its significance in predicting prognosis in cancers, diabetes mellitus, hypertension and cardiovascular diseases has been stated. It has been reported that it may be a biomarker in eye diseases, such as idiopathic acute anterior uveitis, retinal vein occlusion, age-related macular degeneration, keratoconus, pseudoexfoliation syndrome, and neovascular glaucoma.9,10
In this study, leukocyte, lymphocyte, neutrophil, platelet count, neutrophil/lymphocyte ratio (NLR), platelet/lymphocyte ratio (PLR) and mean platelet volume (MPV) were retrospectively evaluated in patients with idiopathic acute anterior uveitis. Few studies have shown that these parameters can be used as biomarkers of inflammation in idiopathic acute anterior uveitis. The findings obtained in this study are consistent with the previous studies on this subject in the literature.
Materials and methods
In this study, patients diagnosed with acute idiopathic anterior uveitis at Inonu University Faculty of Medicine, the Department of Ophthalmology, Malatya, Turkey, between March 2016 and February 2020 were included. Patients diagnosed with chronic form of uveitis were not included in the study. The notes of all patients were retrospectively analysed and their clinical results were reported. Written informed consent was obtained routinely in our hospital from all patients and healthy volunteers before initiating any procedure after a thorough explanation. This study was performed in accordance with the Declaration of Helsinki and approved by the local ethics committee (Inonu University Clinical Research Ethics Committee. Number: 2022/3946). Fifty patients (25 men and 25 women) and as the control group, 50 people (25 males and 25 females), consisting of healthy volunteers, were included in this study. Blood samples of the patients were taken into ethylenediaminetetraacetic acid (EDTA) tubes before starting treatment.
A complete ophthalmological examination, including corrected visual acuity, tonometry, slit lamp and fundus examination, was performed in all patients. Gender, age, leukocyte, neutrophil, lymphocyte, platelet count, MPV, PLR, and NLR values of the patients, were recorded. The NLR was calculated by dividing the absolute number of neutrophils in the blood by the absolute number of lymphocytes. PLR was calculated by dividing the absolute number of platelets in the blood by the absolute number of lymphocytes. Each parameter of uveitis and control groups was compared with each other. Blood parameters were measured using an automated blood cell counter (Beckman Coulter LH 780 Hematology Analyzer, Miami, Florida, USA). The following reference values were determined for leukocyte: 4.3–10.3 × 103/mL, neutrophil: 2.0–6.9 × 103/mL, lymphocyte: 0.6–3.4 × 103/mL, platelet: 150–400 × 103/mL, and MPV: 6.8 – 10.8 fL.
The diagnosis of idiopathic anterior uveitis includes patients with the ophthalmologic examination, iritis and iridocyclitis with cells and/or flare in the anterior chamber and no evidence of vitreous and posterior segments. Disease-specific laboratory tests (liver and renal function tests, anti-nuclear antibodies, rheumatoid factor, and anti-thyroglobulin) were administered for etiology and bacterial, viral, fungal, and protozoal infectious diseases were investigated and no cause of uveitis was found.
Patients diagnosed with idiopathic anterior uveitis were included in this study and patients with chronic diseases (diabetes mellitus, hypertension, cancer, hematological diseases, rheumatologic diseases, infectious diseases, autoimmune diseases, pulmonary diseases and endocrine disorders), patients with a history of ocular disease, ocular trauma, ocular surgery, ocular infections, drug treatment and smokers were excluded. The control group consisted of healthy volunteers with no evidence of intraocular inflammation and the history of ocular and systemic disease except refractive error.
Statistical analysis
The statistical analyses were conducted using the Statistical Package for Social Science v25.0 software (SPSS, Chicago, IL, USA). Demographic, clinical and biochemical variables were classified as categorical variables or continuous variables. A Kolmogorov-Smirnov test for normality was performed. Student’s t-test or Mann-Whitney U test was used to compare the groups as appropriate. p-values less than 0.05 were considered to be statistically significant. Receiver operating characteristic (ROC) analysis was also performed to identify the cut-off threshold and quantify the accuracy of N/L and P/L. Sensitivity, specificity and the area under the ROC curve were used for an overall estimation of the accuracy of the classifier.
Results
Comparison of demographic and laboratory parameters between the genders.
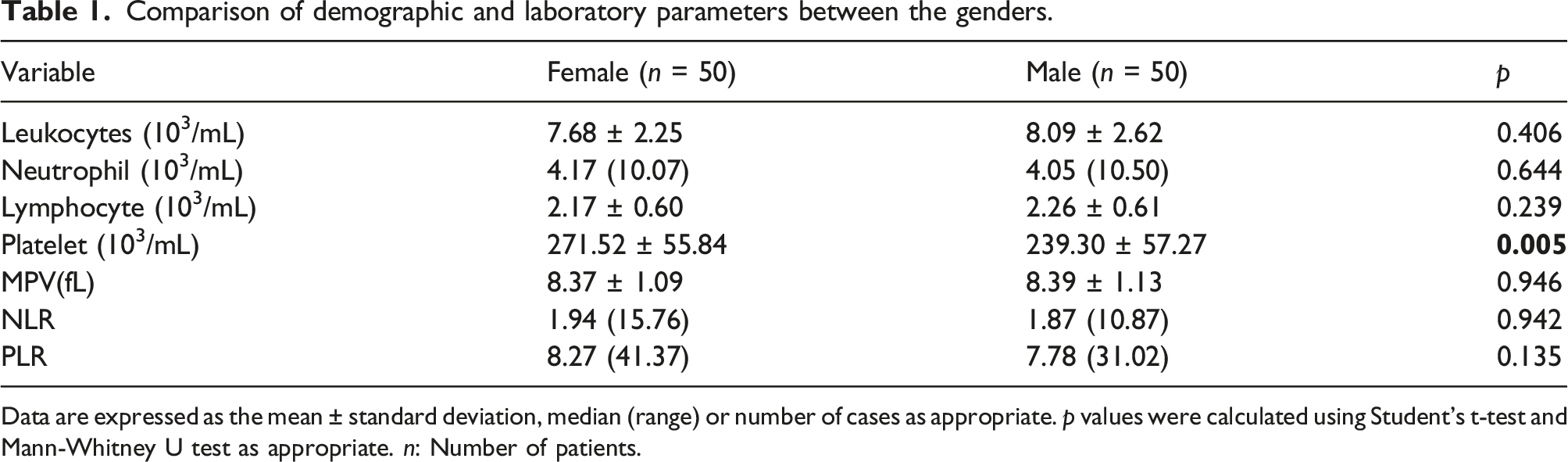
Data are expressed as the mean ± standard deviation, median (range) or number of cases as appropriate. p values were calculated using Student’s t-test and Mann-Whitney U test as appropriate. n: Number of patients.
Comparison of demographic and laboratory parameters between the groups.
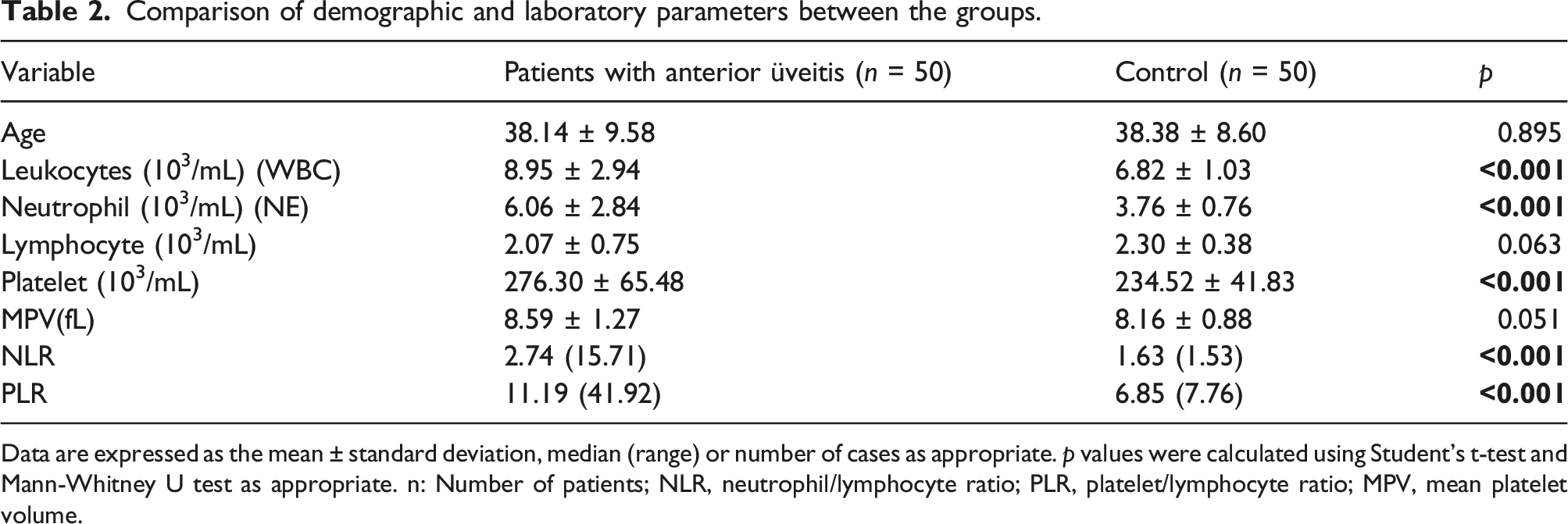
Data are expressed as the mean ± standard deviation, median (range) or number of cases as appropriate. p values were calculated using Student’s t-test and Mann-Whitney U test as appropriate. n: Number of patients; NLR, neutrophil/lymphocyte ratio; PLR, platelet/lymphocyte ratio; MPV, mean platelet volume.
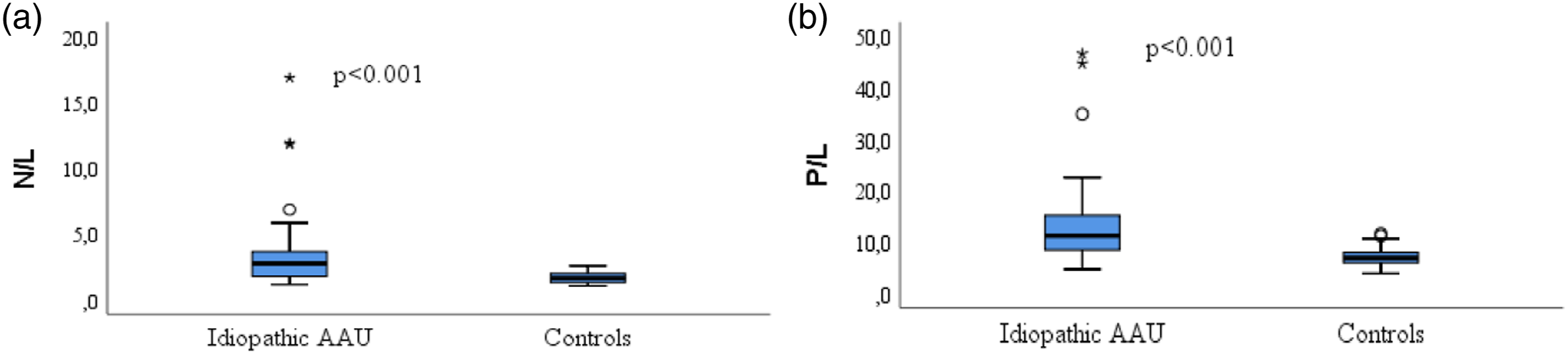
Boxplot showing N/L and P/L values. (a): Comparison of two groups in terms of N/L: p < .001; (b): Comparison of two groups in terms of P/L: p < .001. AAU: Acute anterior uveitis; N/L: Neutrophil to lymphocyte ratio; P/L: Platelet to lymphocyte ratio.
ROC analysis of the studied variables is shown in Figure 2. According to ROC analysis, the area under the ROC (AUROC) value of the N/L to distinguish controls and patients was 0.805. The best cut-off value was 2.49. Sensitivity was 56.0% and specificity was 98.0% (Figure 2). The AUROC value of the P/L to distinguish controls and patients was 0.657, with a cut-off value of 11.17. Sensitivity was 52.0%, and specificity was 98.0% (Figure 2). ROC curve analysis for discrimination between controls and idiopathic AAU. AAU: Acute anterior uveitis; N/L: Neutrophil to lymphocyte ratio; P/L: Platelet to lymphocyte ratio; AUC: Area under the curve.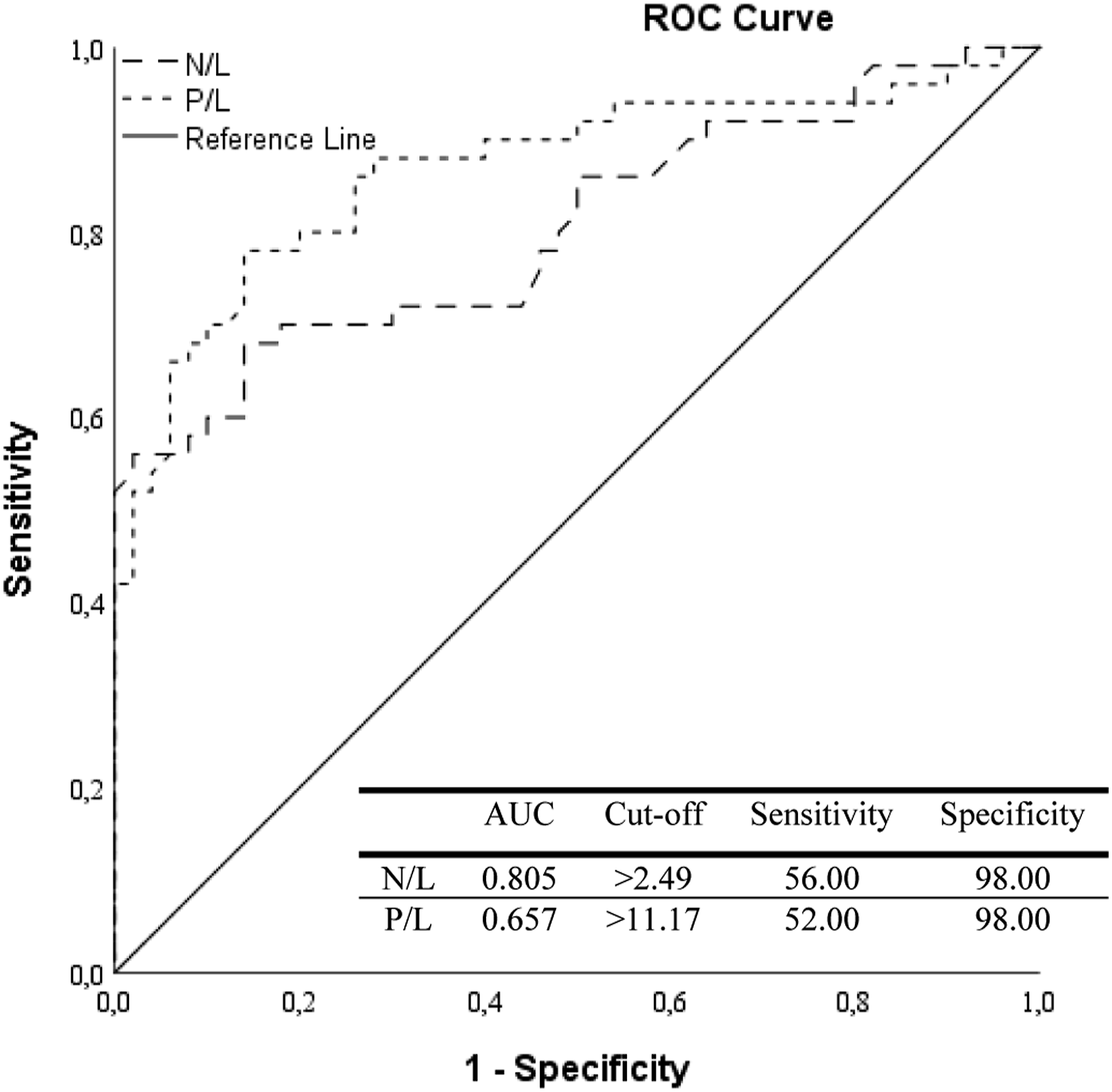
Discussion
All over the world, the etiology of uveitis includes infections, cancers, systemic diseases, immunological diseases, traumas, and drugs. 8 In 60% to 80% of people diagnosed with acute anterior uveitis, the cause of the disease cannot be found and this group is called ‘idiopathic anterior uveitis.’ Acute anterior uveitis is usually self-limiting, but there is no evidence for how long and how often in which patients it will spontaneously regress. 11 History, physical examination, various laboratory tests and imaging techniques are used to determine the etiology of the patient presenting with an acute uveitis attack. One of these tests is a whole blood count test. Its application is simple, and it is widely used in diagnosis. 12 In this study, Ileukocyte, neutrophil, lymphocyte, platelet count, NLR, PLR, and MPV levels were analysed.
Leukocytes (White blood cells) make up less than 1% of the total blood volume. There are several types of leukocytes in different sizes, functions and structures (neutrophil, lymphocyte, monocyte, eosinophil, basophil) Neutrophils make up 50–70% of circulating leukocytes. They are short-lived, but their lifespan is prolonged in inflammatory and infectious conditions.13,14 Neutrophils migrate for phagocytosis of various particles found in inflamed areas in the acute inflammatory state. They induce an immune response by releasing cytokines, eicosanoids, platelet-activating factors and cationic proteins. 7 Intraocular inflammation in uveitis may cause blood-aqueous barrier dysfunction. Due to this dysfunction, inflammatory cytokine levels are increased in serum in cases of uveitis.15 In their study, Zhang et al. found that mean levels of neutrophils were significantly higher in patients with neovascular glaucoma secondary to retinal vein occlusion. 10 In this study, the neutrophil count was significantly higher in the uveitis group than in the control group.
Lymphocytes make up 20–30% of the white blood cells in the circulation. They are responsible for the specific defense known as immunity against infections.16 In their study, Şimşek et al. investigated the relationship between Fuchs uveitis syndrome and complete blood count inflammation. They stated that inflammation in Fuchs uveitis syndrome is not only limited to the eye locally but also causes systemic inflammation. Generally, in acute inflammation, an increase in the number of neutrophils and monocytes is observed, while an increase in the number of lymphocytes is observed in chronic inflammation. They reported that, unlike other acute uveitis etiologies, an increase in lymphocyte count and a decrease in NLR level were observed due to the chronic nature of Fuchs uveitis syndrome.15 In this study, there was no significant difference in the lymphocyte count between the two groups.
Platelets are specialized blood cells that play a central role in hemostasis, thrombosis, inflammation and wound healing. 17 Leukocytes and platelets are markers of inflammation.9,10,18 MPV is a parameter of whole blood count. It is associated with platelet function and activation. In inflammation, cytokines have been shown to suppress the size of the platelets by affecting the megakaryopoiesis and causing the release and decrease of smaller platelets into the bloodstream. In some other studies, it has been stated that larger platelets resulting from increased turnover as a result of platelet activation are released into the bloodstream. MPV is an indicator of inflammation and disease activity in various inflammatory diseases.19–21 In the study of Kısacık et al., MPV was significantly lower in patients with ankylosing spondylitis and patients with active rheumatoid arthritis compared to the control group. 19 Türkçü et al. reported that the MPV in patients with active uveitis was lower than in controls. 22 In this study, the platelet counts were significantly higher in the uveitis group than the control group and no significant difference was found between the two groups in MPV level.
PLR is a new biomarker of inflammation. It is indicative of poor prognosis in people with peripheral arterial occlusive disease due to its key role in atherosclerosis and atherothrombosis. In addition, it is a sensitive marker and prognostic factor in many malignancies.21,23 Osami et al. reported that there was a significant difference in leukocyte, neutrophil, lymphocyte, platelet count, NLR and PLR levels in patients with ankylosing spondylitis when those with active disease and those with inactive disease were compared. 24 In the study reported by Jiang et al., NLR and PLR were significantly higher in patients with active Behçet's disease than in inactive Behçet’s disease and the control group. 25 İcel et al. reported that NLR and PLR levels significantly increased in patients with degenerative high axial myopia compared to patients with non-degenerative high axial myopia, and there was a connection between the development of myopia and increased inflammation. 26 Kurtul et al. reported that the PLR level was high in patients with retinal vein occlusion. 27 The relationship between inflammatory processes and uveitis has been known for a long time. Özgönül et al. reported in their study that PLR and NLR levels were significantly higher in patients with idiopathic acute anterior uveitis than the control group. 28 In this study, PLR was significantly higher in the uveitis group than in the control group.
NLR is an easily obtainable marker indicating the inflammation status in the body.21,29,30 It has been studied in inflammatory diseases, diabetes, hypertension, malignancy, age-related macular degeneration, diabetic retinopathy, keratoconus, and retinal vein occlusion. In the study reported by Bozkurt et al., no significant difference was found in the NLR level when the keratoconus group was compared with the control group. PLR was significantly higher in the keratoconus group compared to the control group. 31 Balci et al. stated that leukocyte, neutrophil, thrombocyte and NLR values are crucial in distinguishing systemic infectious and non-infectious etiology in patients presenting with a uveitis attack for the first time. In the study, they found that the leukocyte, neutrophil, platelet, and NLR levels were significantly higher in the systemic infectious group compared to the systemic non-infectious group. There was no significant difference in PLR between the groups. Lymphocyte level was lower in the systemic infectious group than in the non-infectious group. 12 Qin et al. found that PLR, NLR and MPV levels increased in patients with systemic lupus erythematosus in their study. They reported that increased NLR and PLR levels correlated with the activity of the disease. 21 In this study, NLR was significantly higher in the uveitis group compared to the control group.
In this study, the median NLR value was 2.74 and the median PLR value was 11.19 in the uveitis group, while the median NLR value was 1.63 and the median PLR value was 6.85 in the control group. In the ROC curve analysis, the AUC for NLR was 0.805, with a sensitivity of 56.0% and a specificity of 98.0%. The AUC for PLR was 0.657, with a sensitivity of 52.0% and a specificity of 98.0%. PLR and NLR have similar sensitivity. This indicates that N/L and P/L have equivalent values to distinguish the AAU group from controls. As given in recent studies, PLR and NLR, as inflammation markers, can guide the diagnosis of the disease, its severity, development of complications and prognosis prediction.15,18,21,28
This study has some limitations. It is limited by the relatively small sample size. However, since this study was retrospective, only the spot blood values of the patients have been studied. Since the blood values in the follow-up of the patients could not be checked, evaluation could not be made regarding prognosis. This study needs to be supported by prospective and controlled clinical studies with a larger sample size.
The weakness of this study is that only spot blood samples were studied and the sample size was relatively small. The strength of this study is that it is one of the very few studies in patients with acute idiopathic anterior uveitis.
Conclusion
Laboratory scans to diagnose the underlying disease causing uveitis are expensive and time-consuming. Whole blood parameters frequently used in the clinic are easily applicable and inexpensive. There are very few studies in the literature on this subject in patients with idiopathic anterior uveitis. This study supports the findings of previous similar studies. In this retrospective study, it is thought that leukocyte, neutrophil, platelet counts, PLR, and NLR levels are significant in patients with idiopathic acute anterior uveitis and can be used as a diagnostic marker in more studies in the future and will be useful in early diagnosis and predicting the disease prognosis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
Data supporting the findings of this study are available.