
Abstract
Community-acquired pneumonia is a common disease associated with high mortality. This retrospective study examined whether the neutrophil–lymphocyte count ratio (NLR), already widely used as an index of inflammation, can be used to predict in-hospital mortality of adults with community-acquired pneumonia. Clinical characteristics, CURB-65 and pneumonia severity index score of pneumonia severity, NLR, serum levels of C-reactive protein and procalcitonin, and in-hospital mortality were analyzed for 318 consecutive adults with community-acquired pneumonia admitted to West China Hospital between July 2012 and December 2013. The ability of NLR and other parameters to predict in-hospital mortality was assessed using receiver operating characteristic (ROC) curves. Results showed that NLR increased with increasing CURB-65 (P < 0.05) and pneumonia severity index (P < 0.05), and NLR correlated positively with serum levels of C-reactive protein (r = 0.239, P < 0.05) and procalcitonin (r = 0.211, P < 0.05). The median value of NLR was significantly higher among patients who died in hospital (11.96) than among those who were alive at the end of hospitalization (4.19, P < 0.05). Based on a cut-off NLR of 7.12, this index predicted in-hospital mortality with a sensitivity of 82.61% and specificity of 72.20% (area under ROC curve, 0.799). Predictive power was greater for the combination of NLR and serum levels of C-reactive protein and procalcitonin. These results suggest that NLR may be useful for predicting prognosis in Chinese adults with community-acquired pneumonia, and it may work better in combination with traditional markers.
Introduction
Despite advances in diagnosis and treatment, community-acquired pneumonia (CAP) remains a common, potentially fatal disease associated with significant morbidity, mortality, and health care expenditure.1,2 Overall annual incidence is approximately 1600 per 100,000 in the United States and 1100 per 100,000 in Europe, with approximately 250 of 100,000 patients requiring hospitalization. 3 While mortality associated with CAP is below 5% among outpatients, it can be as high as 10% among inpatients and can exceed 30% among patients admitted to the intensive care unit. 4 Identifying patients at high risk of mortality could substantially improve their treatment and management.
Risk-stratification and prognostic evaluation of CAP remain challenging. Classical biomarkers such as C-reactive protein and procalcitonin are often used, preferably in combination with clinical risk scores, to identify patients with CAP who are at high risk of mortality and to guide antibiotic therapy. 5 However, these two biomarkers do not always perform satisfactorily,6,7 highlighting the need to identify better biomarkers.
One possibility is the neutrophil-lymphocyte count ratio (NLR), an easily determined index already widely used to evaluate systemic inflammatory responses. 8 NLR has proven superior to C-reactive protein level, white blood cell count and neutrophil count for predicting bacteremia in an emergency care unit. 9 NLR may also have prognostic potential in other diseases, such as cancer, ST elevation myocardial infarction, and critical illness.10–12 Few studies have assessed the potential of NLR to help predict prognosis of patients with CAP. Therefore, we examined this question retrospectively in a cohort of patients treated at our hospital in southwest China.
Patients and methods
Patients
A consecutive series of 318 adult patients (18 years or older) diagnosed and treated for CAP at West China Hospital (Chengdu, China) between July 2012 and December 2013 were included in this retrospective study. CAP was diagnosed according to criteria of the Infectious Diseases Society of America as well as results of chest X-ray or thoracic computed tomography. 13 Patients were excluded from the study if they were younger than 18, had hospital-acquired pneumonia, had been treated with antibiotics outside our hospital, or had cancer. Patients were also excluded if insufficient clinical information was available. The study protocol was approved by the Human Research Ethics Committee of West China Hospital.
Data collection and outcome analysis
The following patient characteristics, clinical features, and laboratory data at admission were extracted from the centralized hospital database: age; gender; serum levels of C-reactive protein and procalcitonin; counts of white blood cells, neutrophils, and lymphocytes; and NLR. Each patient was followed up until in-hospital mortality or discharge. The outcome of interest was in-hospital mortality or survival. All these biomarkers were measured as part of routine clinical care at our hospital. Serum levels of C-reactive protein were measured using rate nephelometry on an IMMAGE analyzer (BECKMAN, USA), while serum levels of procalcitonin were determined by immunofluorescence assay (Roche, IN, USA). Counts of white blood cells, neutrophils, and lymphocytes were made using an XE-2100 hematology analyzer (Sysmex, Kobe, Japan).
Disease severity
The CURB-65 and pneumonia severity index (PSI) score was calculated for all patients upon admission. This CURB-65 score takes into account five risk factors associated with increased mortality: 14 confusion or decreased consciousness, abnormal renal function (blood urea nitrogen >7 mmol/L), respiratory frequency ⩾30/min, systolic blood pressure <90 mmHg or diastolic blood pressure ⩽60 mmHg, and age ⩾65 years. PSI score was calculated based on age, comorbidities, abnormal physical findings, and abnormal laboratory findings on admission.
Statistical analysis
Data were represented as median ± inter quartile range (IQR). Student’s t test was used to assess the significance of differences in NLR, levels of C-reactive protein or procalcitonin or counts of white blood cells, neutrophils, or lymphocytes between patients who died in-hospital and those who did not. Possible correlations of patient and laboratory results with in-hospital mortality were explored using the bivariate Pearson’s correlation test. Receiver operating characteristic (ROC) curves were generated to evaluate the sensitivity and specificity of different potential predictors of in-hospital mortality. ROC curves display sensitivity versus 1-specificity such that the area under the curves (AUC) varies from 0.5 to 1.0, with higher values indicating higher discriminatory ability. 15 Data were analyzed using SPSS 18.0 for Windows (IBM, Chicago, IL, USA). The level of significance for all statistical tests was a two-sided P of 0.05.
Results
Characteristics of included subjects
A total of 318 patients (211 men, 107 women) with median age of 61 years met our inclusion criteria and were included in our study. Median length of hospitalization was 13 days, and 23 patients (7.2%) died during hospitalization. The clinical characteristics, comorbidities, main laboratory findings, and CURB-65, PSI score distributions of enrolled subjects were listed in Table 1.
Clinical characteristic of included subjects.

AUC: area under the curve; CAP: community-acquired pneumonia; COPD: chronic obstructive pulmonary disease; CRP: C-reactive protein; NLR: neutrophil-lymphocyte count ratio; PCT: procalcitonin; PSI: pneumonia severity index; WBC: white blood cell.
The data were presented as median ± inter quartile range deviation;
NLR
The median NLR across all patients was 4.67 (IQR 2.49–8.69), and the ratio increased significantly when moving from a lower CURB-65 risk group to a higher one (P < 0.001) based on four risk groups: low (0), low (1), moderate (2), and high (⩾3) (Figure 1). The NLR also correlated positively with PSI score (r = 0.443, P < 0.001). NLR correlated positively with serum levels of C-reactive protein (r = 0.239, P < 0.001; Figure 2(a)) and procalcitonin (r = 0.211, P < 0.001; Figure 2(b)).

Correlation between NLR and CURB-65 score. Neutrophil-lymphocyte count ratio (NLR) levels in community-acquired pneumonia patients were classified into four CURB-65 categories (0, I, II, and III+IV+V). NLR increased with increasing CURB-65 score (P < 0.05).
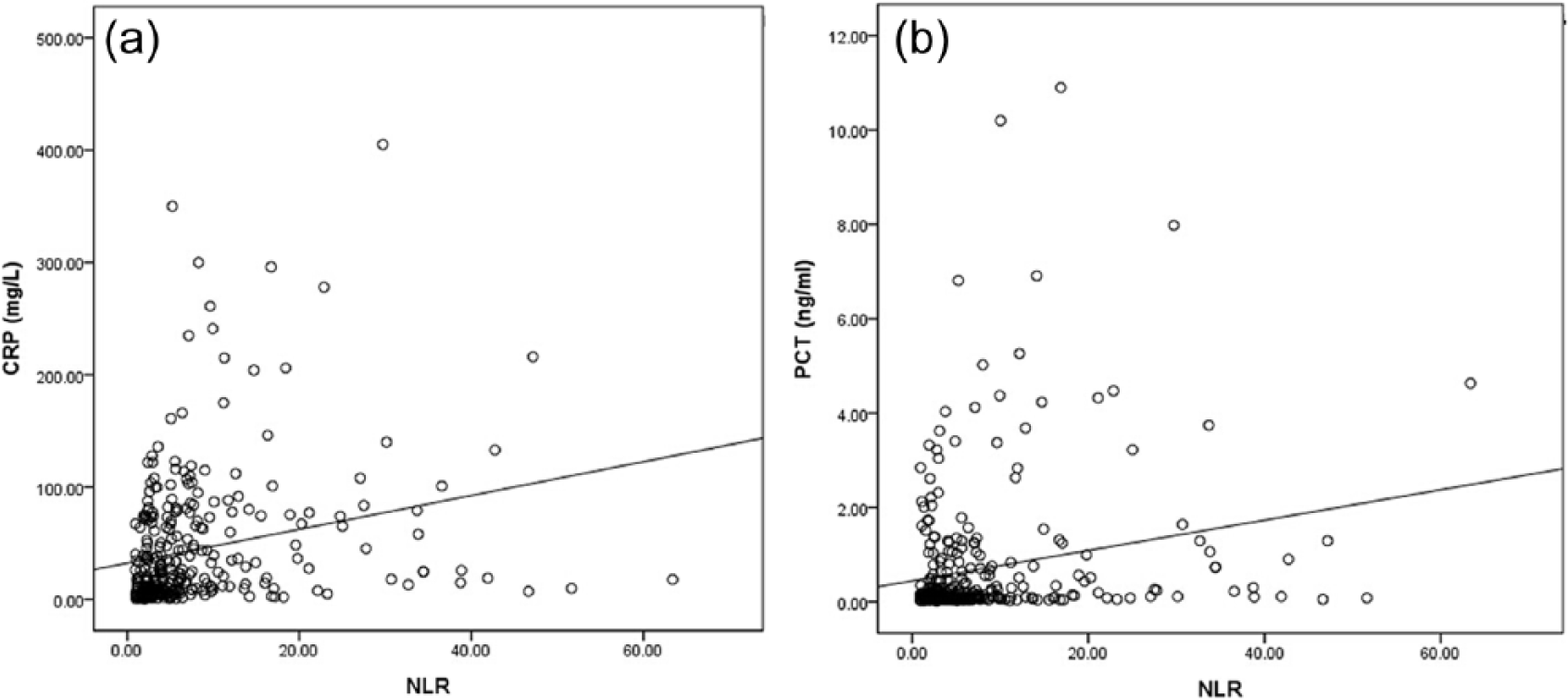
Correlation of NLR with C-reactive protein and procalcitonin. Neutrophil-lymphocyte count ratio (NLR) levels in patients with community-acquired pneumonia correlated significantly with serum levels of (a) C-reactive protein (CRP; r = 0.239, P < 0.001) and (b) procalcitonin (PCT; r = 0.211, P < 0.001).
Predictive power of NLR
NLR was significantly higher among patients who died in hospital (11.96, IQR 7.26–30.68) than among those who survived (4.19, IQR 2.39–7.52, P < 0.001). Similarly, patients who died showed significantly higher white blood cell counts (8.63 vs. 7.12 × 109/L, P < 0.001), C-reactive protein (27.50 vs. 19 mg/L, P = 0.023), and procalcitonin (0.84 vs. 0.11 ng/ml, p < 0.001).
ROC curve analysis for using NLR alone to predict in-hospital mortality indicated an optimal cut-off NLR of 7.12, AUC of 0.799, sensitivity of 82.61%, and specificity of 72.20% (Figure 3(a)). This predictive ability exceeded that of C-reactive protein, white blood cell count or procalcitonin on their own (Table 2). Combining NLR with other markers increased predictive accuracy, with the best AUC of 0.828 obtained using the combination of NLR and procalcitonin (Figure 3(b)).

(a) ROC curves of NLR, procalcitonin, C-reactive protein, or white blood cell count for predicting in-hospital mortality of patients with community-acquired pneumonia. The ROC curves for single predictors had the following areas: neutrophil-lymphocyte count ratio (NLR), 0.799; C-reactive protein (CRP), 0.681; procalcitonin (PCT), 0.789; white blood cell count (WBC), 0.679. (b) ROC curves for combined predictors had the following areas: NLR+CRP, 0.794; NLR+PCT, 0.828; NLR+CRP+PCT, 0.827; NLR+CRP+PCT+WBC, 0.801.
Prediction accuracy of NLR, PCT, CRP, and WBC for mortality of CAP patients.

AUC: area under the curve; CAP: community-acquired pneumonia; CRP: C-reactive protein; NLR: neutrophil-lymphocyte count ratio; NPV: negative predictive value; PCT: procalcitonin; PPV: positive predictive value; WBC: white blood cell.
Discussion
Reliable prediction of patients with CAP may substantially improve patient management, timely anti-infectious therapy, and nurse intervention. 16 Our results suggest that NLR, which correlates with the severity of the disease, may predict in-hospital mortality with reasonable specificity and selectivity, and even more so when it is combined with classical indices such as C-reactive protein, procalcitonin, and white blood cell count.
Our results are consistent with previous work showing elevated NLR in patients with CAP, and even higher levels among patients who die in hospital than among those who survive. 17 The AUC of NLR to predict mortality was 0.701 in that study, while we determined an AUC of 0.799. The authors of that study concluded that NLR predicts severity of CAP and in-hospital mortality more accurately than traditional markers of infection. Another study found evidence that NLR is significantly higher in patients with CAP of bacterial origin than in patients with pulmonary tuberculosis, suggesting the possibility of discriminatory diagnosis. 18 These studies, together with the present work, justify further work into the diagnostic and prognostic usefulness of NLR in CAP, as well as mechanistic studies to explain this predictive ability.
We found that although procalcitonin levels on their own could predict in-hospital mortality with an AUC of 0.789, this index did not perform as well as NLR. Procalcitonin is a classical biomarker of inflammation useful for assessing infection in patients with CAP as well as for predicting mortality among such patients. Procalcitonin seems to be the best among the most prevalent inflammatory biomarkers, and it correlates with scoring systems for CAP used in the clinic.19,20 While consideration of procalcitonin can reduce unnecessary antibiotic use, 21 its cost-effectiveness as a biomarker remains controversial. 22 Our results suggest that procalcitonin is most useful as a prognostic indicator when combined with NLR.
Like procalcitonin, C-reactive protein on its own could predict in-hospital mortality with an AUC of 0.681, but it did not perform as well as NLR. C-reactive protein has previously proven helpful for assessing severity of CAP and predicting prognosis. 23 It can also aid patient management by helping clinicians determine whether patients not responding to therapy are true non-responders or are responding quite slowly.24,25 Our results suggest that C-reactive protein is even more useful as a prognostic indicator when combined with NLR. Further study should examine whether the triple index of NLR, C-reactive protein, and procalcitonin can also be useful for predicting treatment response.
Our results in this Chinese cohort from a single medical center should be verified in larger studies with different ethnic groups. In our cohort, 48% had a CURB-65 score of 0, whereas only 24% had this score in a previous study; 17 and the median PSI score was only 86, this may explain why NLR in our cohort (4.67) was much lower than reported in that study. 17 Further work is needed to examine the validity of our results for patients with more severe pneumonia. In addition, future work should examine how the predictive power of NLR relates to infection, since our patients showed a low rate of positive sputum culture.
If verified as a mortality predictor in other patient populations with CAP, NLR would present several advantages over other potential predictors, including mid-regional proadrenomedullin and lysophosphatidylcholine.26,27 NLR is calculated from routine blood test results, so no additional testing is necessary, saving time and expense. It can be combined with white blood cell count, also routinely tested, in order to improve prognostic power.
Conclusion
This study suggests that NLR is a simple, promising marker for assessing the severity of CAP and for identifying adult patients at elevated risk of in-hospital mortality. These findings justify further work into the role of NLR in comprehensive management of patients.
Footnotes
Acknowledgements
Ting Yang, Chun Wan, and Hao Wang authors contributed equally to this work and share joint first authorship.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work is supported by grants from the National Natural Science Foundation of China (81230001, 81300032), and Projects in the Science and Technology Pillar Program from the Department of science and technology of Sichuan province (2015SZ0151). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.