
Abstract
Individuals with cerebral palsy (CP) develop skeletal muscle contractures that impair muscle function. In turn, contractures affect the ability to ambulate and often promote a sedentary lifestyle. The aim of the present study was to investigate the systemic inflammatory markers transforming growth factor beta-1 (TGFβ1), C-reactive protein (CRP), and interleukin-6 (IL-6) in children and adults with CP. Blood samples of n = 34 participants (24 individuals with CP (n = 14 children with CP age 10.36 ± 1.1 and n = 10 adults with CP age 38.80 ± 3.6) and 10 healthy adults age 36.63 ± 3.8) were analyzed for circulating levels of TGFβ1, CRP, and IL-6 using Sandwich Enzyme linked immunosorbent assay (ELISA) analyses (R&D systems). TGFβ1 and CRP levels were significantly higher in children with CP compared to both adults with CP (TGFβ1: P < 0.0005 and P < 0.0002, respectively) and healthy adults (CRP: P < 0.0001 and P < 0.0001, respectively), while no differences were observed between the adults with CP and healthy adults in TGFβ1 (P = 0.29) and CRP (P = 0.59), respectively. Furthermore, IL-6 levels showed no significant differences between the groups. The present findings indicate that the level of systemic inflammation is increased in children with CP. We speculate that persisting inflammation in children with CP might influence the development of muscle contractures, resulting in reduced muscle mass and marked muscle weakness in adults with CP.
Keywords
Introduction
Cerebral palsy (CP) describes a spectrum of movement disorders caused by a lesion of the developing brain.1,2 The upper motor neuron lesion impairs neuromotor development 2 and results in a cascade of secondary musculoskeletal changes including muscle contractures. 1 Contracture development in individuals with CP is progressive and leads to a step-wise reduction in musculoskeletal development, muscle fatigability, and reduced physical activity. 2 As a consequence of poor muscle health and a sedentary lifestyle, the prevalence of chronic conditions such as diabetes, hypertension, and arthritis is greater in individuals with CP as compared to typically developed (TD) peers. 3 In typically developing individuals, all of these impairments and conditions have been associated with elevated circulating systemic inflammatory markers, which can contribute to the development or progression of certain conditions. 4
Transforming growth factor beta-1 (TGFβ1) is one systemic pro-inflammatory cytokine that has been shown to influence muscle development and elevated mRNA levels of TGFβ1 and TGFβR2 have been observed in muscle tissue of children with CP with fixed contractures. 5 In addition, C-reactive protein (CRP) is another important systemic inflammatory marker and indicator of muscle tissue catabolism and previous findings have shown that CRP might have a direct negative influence on skeletal muscle cells and underlies the connection between poor muscle function and systemic inflammation. 6 Another pro-inflammatory cytokine that has received considerable attention in connection to exercise and muscle growth is interleukin 6 (IL-6), as chronically elevated levels promote skeletal muscle wasting. 7 Early and accelerated loss of strength and functional capabilities occur in individuals with CP relative to healthy individuals. 8 Little is known about what factors contribute to the decline. Systemic inflammatory cytokines and acute phase proteins may also affect muscle growth and quality and thus musculoskeletal development. Therefore, the aim of this study was to investigate the circulating levels of TGFβ1, CRP, and IL-6 in children and adults with CP compared to typically developing healthy individuals.
Methods
Design
Thirty-four participants (24 individuals with CP and 10 healthy adult participants) were recruited to the study. Anthropometric data are presented in Table 1. Inclusion criteria of the individuals with CP: (1) clinical diagnosis of CP (brain lesion diagnosed within the first 2 years of life); (2) the clinical history of each participant with CP and gross motor function classification system (GMFCS) scores are shown in Table 2. Exclusion criteria: Other brain lesion(s) that have been diagnosed after the first 2 years of life. The healthy participants were included in the study if they had no history of previous musculoskeletal disorders. The research protocol was approved by the Regional Ethics Committee for Copenhagen (H-4-2014-047), in compliance with the Helsinki Declaration. Participants were recruited via the Orthopedic Department, University Hospital, Hvidovre, Denmark, or from the University of Copenhagen. All adult participants, and parent/guardian of child participants, gave informed consent to be involved in the study.
Subject characteristics.
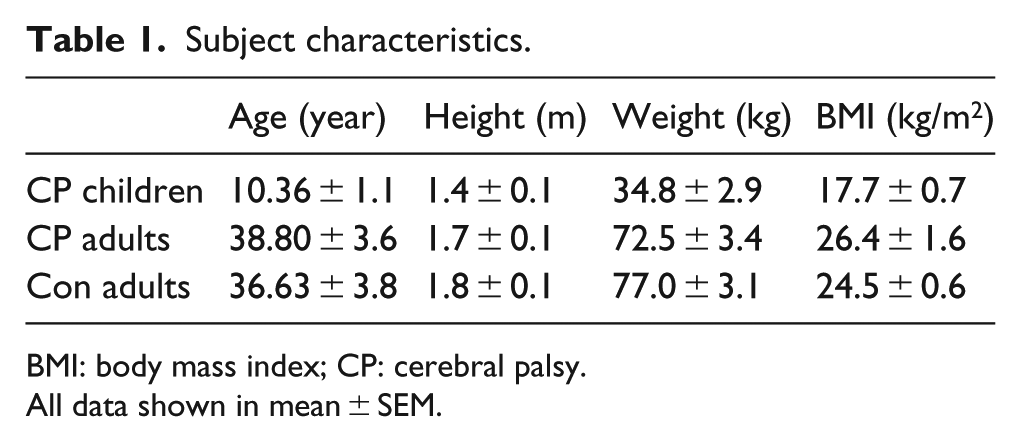
BMI: body mass index; CP: cerebral palsy.
All data shown in mean ± SEM.
Clinical history of all patients.

GMFCS: gross motor function classification system; CP: cerebral palsy.
Blood samples were taken from n = 14 children with CP (CP_C), n = 10 adults with CP (CP_A), and n = 10 healthy adults (Con_A). All blood samples were taken in the morning while the participant rested in a quiet laboratory room. The blood samples of children were taken the day before a planned orthopedic surgery. All children were examined prior to surgery by the treating surgeon and considered medically healthy (without any present cold or flu infections) and able to proceed to surgery. Blood samples were taken from all adults with CP were also taken in a non-stressful environment 1–4 days before a planned orthopedic surgery, and from all healthy adults after inclusion in the study. Blood samples were collected using a butterfly needle (Terumo; cannula 0.8 × 19 mm, 18 cm) from the antecubital vein in one arm and left on slush ice for 15 min before they were spun and plasma was removed. The plasma was stored at −80°C for subsequent Enzyme linked immunosorbent assay (ELISA) analysis.
ELISA analysis
Samples were analyzed for TGFβ1, CRP, and IL-6 using a quantitative sandwich enzyme immunoassay (all from R&D Systems, Minneapolis, MN, USA) in accordance with the manufacturer’s recommendations. TGFβ1 ELISA: plasma samples were first activated and then neutralized according to the manufacturer’s instructions. Samples from all participants were analyzed in the same assay. The minimum detectable dose (MDD) ranged from 1.7–15.4 pg/mL, and the intra-assay variation (coefficient of variation) was 2.7%. Human CRP ELISA: plasma samples were diluted 100-fold according to the protocol. Samples from all participants were analyzed in the same assay. The MDD ranged from 0.005–0.022 ng/mL, and the intra-assay variation (coefficient of variation) was 5.5%. One CP-C sample was under the detectable range and the data were not included in the statistical analysis. IL-6 ELISA: MDD was less than 0.70 pg/mL, and the intra-assay variation (coefficient of variation) was 2.6%. In total, six samples were under the detectable range and not included in the statistical analysis. Final participant data included in analysis were CP_C, n = 11 (three missing samples); CP_A, n = 8 (two missing samples); and Con_A, n = 9 (one missing sample).
Statistics
All data are presented as mean ± SEM. Non-parametric unpaired t-tests were used to analyze differences between the CRP, TGFβ1, and IL-6 levels of the three groups. The level of significance was P < 0.05. All statistical analyses and Figure 1 were generated in GraphPad Prism 6.04 (GraphPad Software, Inc., San Diego, CA, USA).

(a) Plasma TGFβ1 levels shown in picograms per milliliter (pg/mL), (b) plasma CRP levels shown in nanograms per milliliter (ng/mL), and (c) plasma IL-6 levels shown in picograms per milliliter (pg/mL). No significant differences in IL-6 levels were observed between the groups (P = 0.08). Data from n = 14 children with CP (CP_C), n = 10 healthy adults (Con_A), and n = 10 adults with CP (CP_A) are shown. The plasma CRP levels of one CP_C sample were under the detectable range and are therefore missing. Furthermore, the IL-6 plasma levels of six samples were under the detectable range and are therefore missing.
Results
TGFβ1 levels were significantly higher in children with CP (13.21 ± 2.31 pg/mL) compared to both adults with CP (1.97 ± 0.70 pg/mL; P < 0.0005) and healthy adults (1.19 ± 0.16 pg/mL; P < 0.0002) (Figure 1(a)). No differences were observed between adults with CP and healthy adults (P = 0.289). In the assay description from R&D systems, the normal level of TGFβ1 is stated to be lower than detection limit mean of 1165 pg/mL (measured in n = 23 healthy individuals).
The CRP levels of the children with CP (57.22 ± 17.98 ng/mL) were significantly higher when compared to both adults with CP (7.91 ± 2.21 ng/mL; P < 0.0001) and healthy adults (6.89 ± 2.66 ng/mL; P < 0.0001) (Figure 1(b)). No differences were observed between adults with CP and healthy adults (P = 0.588). In the assay description from R&D systems, the normal level of CRP is stated to be lower than detection limit mean of 1547 ng/mL (measured in n = 35 healthy individuals).
The IL-6 levels were also higher but not significant in children with CP (2.61 ± 1.06 pg/mL) compared to both adult groups (adults with CP: 1.44 ± 0.49 pg/mL (P < 0.5916); healthy control adults: 1.25 ± 0.77 pg/mL (P < 0.51) (Figure 1(c))). In the assay description from R&D systems, it is stated the normal level of IL-6 in n = 33 healthy individuals was measured to be lower than detection limit (3.13 pg/mL), while n = 7 further individuals had IL-6 levels that ranged from 3.13 to 12.5 pg/mL.
Discussion
The present study shows that children with CP have significantly higher systemic levels of TGFβ1 and CRP, when compared to adults with CP and healthy adults and also when compared to TD child normative values. 9 Persistent or recurrent elevated blood concentrations of inflammation-related proteins during the first two postnatal weeks in preterm infants are associated with CP 10 ; however, little is known about elevated systemic inflammation and the effects thereof on neurological and/or musculoskeletal development of school-age children with CP. All children that were included in the present study had muscle contractures and needed surgical corrections. It may be speculated that elevated levels of multiple systemic inflammatory markers in this group of children were related to skeletal muscle contractures. Systemic inflammation may be the consequence of the muscle tissue attempting to repair muscle damage following chronic overload. 11 In the growing muscle tissue of children with CP, systemic inflammation may also contribute to the failure of normal hypertrophic growth and tissue remodeling through a reduction of protein synthesis rate as previously observed in muscular dystrophies. 12 Elevated levels of TGFβ1, CRP, and IL-6 have been accompanied by reduced muscle mass, 7 indicating a catabolic effect of inflammation on muscle tissue. However, the present study can unfortunately not conclude any cause and effect relationship between systemic inflammation and severity of muscle contractures. The relationship between the severity of the brain lesion causing CP (as indicated by brain magnetic resonance imaging (MRI)) and levels of systemic inflammation may offer promising opportunities for future studies. One major drawback of the current study is the lack of blood samples from TD children. Therefore, the results from the present study cannot rule out that a general difference exists in inflammatory levels between children and adults, or individuals with differing levels of activity. However, all of our participants were considered medically healthy (no current infections/medical disorders); therefore, any systemic inflammation was expected to be very low. Furthermore, in order to limit stress prior to surgery as a confounding factor, the blood samples have been taken at least 1 day before the surgical intervention. The present study shows that systemic levels of TGFβ1 and CRP are significantly increased in children with CP when compared to healthy adults and adults with CP. An inclusion of blood samples from TD children and CP children without muscle contractures and children who have different neuromuscular disorders might offer interesting and important extensions of this study.
Footnotes
Acknowledgements
All authors have contributed equally to this work and have approved the final version of the manuscript. All authors are designated as authors and are qualified for authorship, and are all listed as authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the Danish research Council (DFF-1333-00197) and the Elsass Foundation.