
Abstract
Objective
To evaluate the value of single or combined detection of procalcitonin (PCT), interleukin-6 (IL-6), serum amyloid A (SAA) and c-reactive protein (CRP) in the differential diagnosis of simple and strangulated intestinal obstruction.
Methods
This retrospectively study collected 61 patients with intestinal obstruction. The patients were classified into the group of simple or strangulated intestinal obstruction according to operation. The age, sex, basic diseases, lesion sites and inflammatory indicators such as PCT, IL-6, SAA and CRP in two groups were collected and analyzed. The Students’ T-test and the Mann-Whitney U test were used to analyze normally and non-normally distributed data, respectively. The categorical variable was analyzed by the chi-square test. The receiver-operating characteristic (ROC) curve and the area under the curve (AUC) were used to predict the differential diagnostic value of single and combined detection of the above clinical inflammatory indicators.
Results
The serum levels of PCT, IL-6, SAA and CRP of the strangulated group were significantly higher than those of the simple group (p < .05). The areas under the ROC curve (AUC) were 0.907 for PCT, 0.712 for IL-6, 0.723 for SAA and 0.681 for CRP. With the cutoff values of PCT (0.24 ng/L), IL-6 (19.55 pg/L), SAA (282.50 mg/L) and CRP (63.00 mg/L), the sensitivity and specificity were 86.40% and 87.20% for PCT, 68.20% and 76.90% for IL-6, 59.10% and 87.20% for SAA, 63.60% and 87.20% for CRP, respectively. And the sensitivity and specificity were 86.40% and 89.70% for combined model. The differences between PCT and the combined model are tiny and neither clinically nor statistically significant.
Conclusions
For discriminating strangulated intestinal obstruction from simple intestinal obstruction, PCT alone may be the preferred approach due to its simplicity.
Introduction
Intestinal obstruction, which is a block in the intestinal tract that prevents food from passing through, is generally divided into the two types: the strangulated and simple intestinal obstruction. 1 However, in comparison to simple intestinal obstruction, the strangulated intestinal obstruction linked to the intestinal ischemia and necrosis is a more severe clinical emergency and its mortality rate ranges from 20% to 30% which is significantly higher than 5 to 8% mortality rate of simple intestinal obstruction.2–4 Without the prompt and appropriate treatment, the patients with strangulated intestinal obstruction will die within a few days of onset. 4 Distinguishing the strangulation and the simple is one of the major problems for physicians. 5 In order to reduce the mortality rate of patients suffering from strangulated intestinal obstruction, the accurate diagnosis and the timely treatment are cardinal. 6
The identification between strangulated and simple intestinal obstruction is fraught with difficulties. The clinical symptoms, signs and laboratory parameters like fever, continuous abdominal pain, peritoneal irritation sign, hyperamylasemia, leukocytosis and tachycardia cannot be used as the basis for the diagnosis or exclusion of strangulated intestinal obstruction.3,7–12 Therefore, imaging study is a vital method for diagnosing the types of intestinal obstruction. 10 Although the abdominal ultrasonography, traditional radiography and magnetic resonance imaging (MRI) can confirm the location of lesion and so on, their diagnostic values are limited.7,11–15 The computed tomography (CT) serves as a main role to solve this difficulty, which can identify etiology, severity, site and complications.13–17 But the possibility of radiation-related cancers is also increased on account of ionizing radiation.5,6,10,14
The tissue hypoxia, impaired intestinal microcirculation, ischemia and necrosis are the primary pathological findings of the strangulated intestinal obstruction, which are related to the inflammation. 6 Serum inflammatory biomarkers for the identification of the simple and strangulation would be of great diagnostic value. The procalcitonin (PCT) elevated in bacterial infection serves as a specific and sensitive index of infected necrosis in some diseases. 18 The C-reactive protein (CRP), a plasma protein associated with the infection, acute inflammation and tissue necrosis, is an acute inflammatory marker.19,20 The interleukin-6 (IL-6) is a biochemical marker of inflammation. 21 PCT, CRP and IL-6 have been studied in the identification of the categories of intestinal obstruction.21–23 Serum amyloid A (SAA) is an indicator of inflammation in clinical laboratory tests and persistently elevates in inflammation.24,25 But there is no clinical use for the identification of types of intestinal obstruction.
In this retrospective case-controlled study with the aim of assessing the effect of PCT, IL-6, SAA and CRP to distinguish strangulated from simple intestinal obstruction. We collected the patients suffering from intestinal obstruction and compared the biomarkers, reported their optimal cut-off value and assessed their diagnostic value.
Materials and methods
Study subjects and clinical data
131 patients with suspected intestinal obstruction from October 2019 to December 2020 were admitted. Due to the limited number of patients, no power calculation was done for estimation of sample size selected for the study. The basic information and inflammatory indicators of patients such as age, gender, the admission time, underlying disease, etiology, type, site, PCT, IL-6, SAA and CRP were collected.
The definitive diagnosis of intestinal obstruction was based on the operation and observing the bowel. Excluding 70 cases, the 61 cases were finally included in this study. The inclusion criteria for: (1) complete clinical record; (2) all patients were diagnosed as intestinal obstruction. The exclusion criteria for: (1) diseases influencing the level of biomarkers, such as acute inflammation and cancers; (2) undergoing recent surgery and trauma.
The 61 patients were divided into two groups: the simple intestinal obstruction group (the simple group) and the strangulated intestinal obstruction group (the strangulated group) according to ischemia and necrosis of intestinal wall. And there were 22 and 39 patients in the strangulated group and simple group, respectively. The PCT, IL-6, SAA and CRP were detected in all cases.
Statistical analysis
Data was presented as maximum-minimum or percentage. The Students’ T-test and the Mann-Whitney U test were used to analyze normally and non-normally distributed data, respectively. The categorical variables were analyzed by the chi-square test. p < .05 was considered to be statistically significant. The diagnostic value of single and combined indicators was determined according to the receiver-operating characteristic (ROC) curve and the area under the curve (AUC). The optimum cutoff values were selected by Youden index. All statistical analyses were performed using SPSS version 25.0 software package.
Results
Characteristics and comparative analysis of the study subjects in the simple and strangulated group
That’s 131 patients in all, the 61 cases were finally included this retrospectively study. The 70 patients were excluded from this study due to the following conditions: incomplete medical record (n = 28), inflammation (n = 21), cancers (n = 19) and recent surgery history (n = 2).
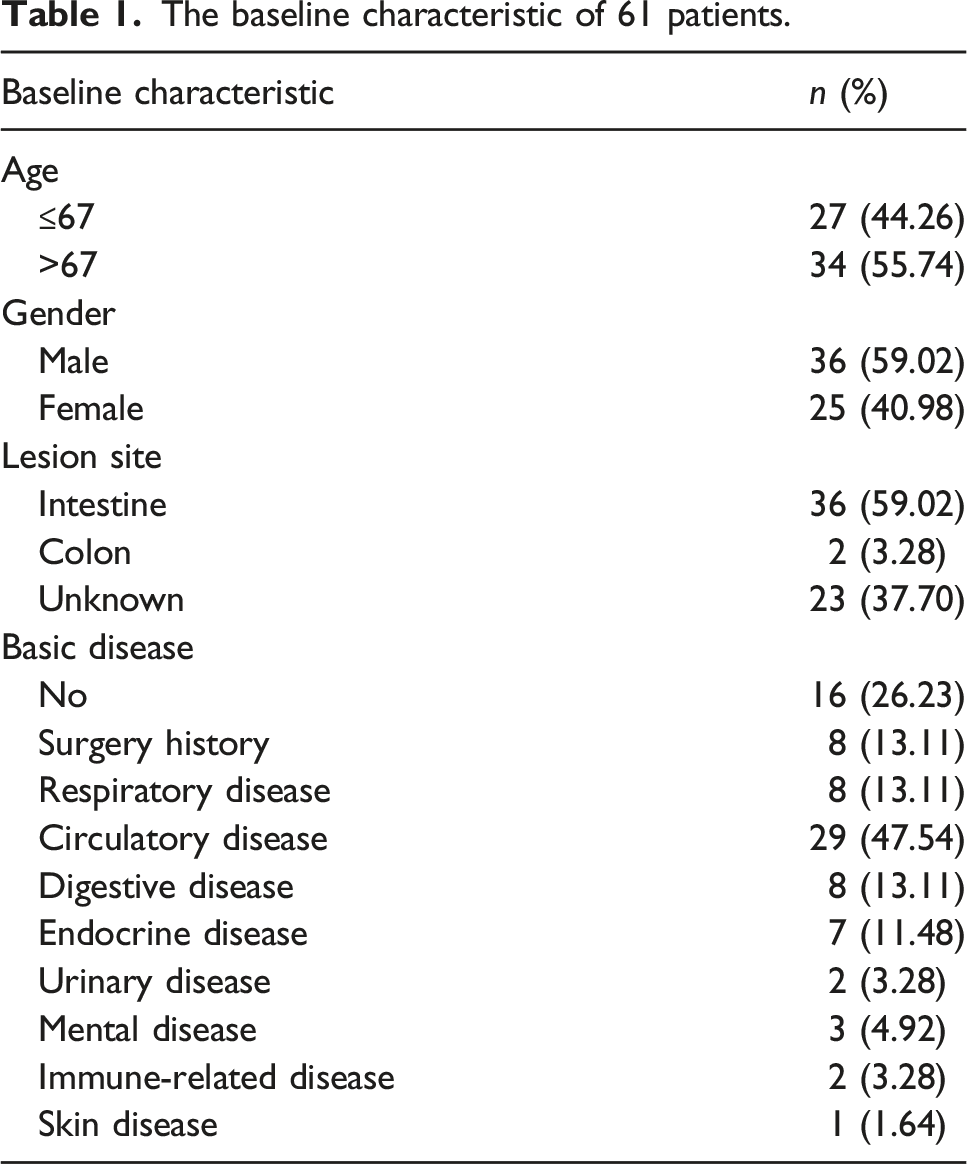
The baseline characteristic of 61 patients.
The comparison of characteristics and clinical data of 61 patients in two groups.

Comparative analysis of the single detection of PCT, SAA, CRP and IL-6 in the simple and strangulated group
The levels of PCT, SAA, CRP and IL-6 were compared between the two groups. As shown in Table 2, the concentration of PCT (ng/L), SAA (mg/L), IL-6 (pg/L) and CRP (mg/L) in the strangulated group were 96.00-0.04 (max-min), 2304.000-0.900, 613.600-0.010 and 317.000-0.010, respectively. And the concentration of PCT (ng/L) is 0.650-0.010 in the simple group, as well as SAA (mg/L) 1800.500-1.200, IL-6 (pg/L) 5527.080-0.010 and CRP (mg/L) 118.90-0.20, respectively. The levels of PCT, SAA, IL-6 and CRP were significantly lower in the simple group than those in the strangulated group. The data showed that PCT, SAA, IL-6 and CRP were significantly statistical (p < .05) in the identifying intestinal obstruction. Thus, it can refer that the PCT, CRP, SAA and IL-6 can be utilized as indicators in clinical differential diagnosis between simple and strangulated intestinal obstruction.
The diagnostic value of these clinical indices in discriminating the strangulated from simple intestinal obstruction was evaluated by ROC curve. The Figure 1 showed that the AUC is 0.723 (95% CI 0.581–0.864) for SAA, as well as 0.907 (95% CI 0.818–0.995) for PCT, 0.712 (95% CI 0.568–0.856) for IL-6 and 0.681 (95% CI 0.510–0.853) for CRP. The optimal cutoff values of PCT, SAA, CRP and IL-6 were presented in Table 3. The cutoff values were set at 282.500 (59.100% and 87.200%) for SAA, 0.240 (sensitivity 86.400% and specificity 87.200%) for PCT, 19.550 (68.200% and 76.900%) for IL-6 and 63.000 (63.600% and 87.200%) for CRP, respectively. Receiver operating characteristic curves for Serum amyloid A, C-reactive protein, Procalcitonin, Interleukin-6. The AUC of SAA, CRP, PCT and IL-6 of the 61 patients in two groups.

Comparative analysis of the combined detection of PCT, SAA, IL-6, CRP in the simple and strangulated group
The above data showed that the PCT was higher specific and sensitive than SAA, IL-6 and CRP in intestinal obstruction. The AUC was also used to determine the diagnostic value of combined indicators. The AUC, sensitivity and specificity of the combined detection of PCT, SAA, IL-6 and CRP in the differential diagnosis of intestinal obstruction were no significantly differences than PCT alone. (Figure 1 and Table 3).
Discussion
The main findings of this retrospective study designed to differentiate strangulation from simple intestinal obstruction are as follows: (1) the concentrations of PCT, SAA, CRP and IL-6 are significantly greater in the strangulated group than those in the simple group; (2) SAA, PCT, IL-6 and CRP (p < .05) are statistically significant for the distinguishing intestinal obstruction; (3) The differences between PCT and the combined model are tiny and neither clinically nor statistically significant; (4) For discriminating strangulated intestinal obstruction from simple intestinal obstruction, PCT alone may be the preferred approach due to its simplicity.
Strangulated intestinal obstruction is a critical clinical emergency requiring accurate and early diagnosis as well as prompt treatment to minimize the mortality rate.4,6 In the past, the discrimination of strangulated intestinal obstruction is based on the symptoms, signs, laboratory tests and imaging examinations which are decisive. 15 But there are some limitations of the identification methods. For example, the abundant gas in the gastrointestinal tract and patient body habitus significantly obscure sonogram that require professional operator to obtain and interpret. 13 Furthermore, radiography has a variable sensitivity ranging from 40% to 80% and may lead to an erroneous diagnosis because of visible fluid-filled loops. 14 Although the CT and MRI have higher sensitivity and specificity, but ionization radiation and expensive cost cannot be ignored.14,16 So, the identification between the simple and strangulated intestinal obstruction is still difficult for the physicians.
PCT is a marker of bacterial infection and can be used to evaluate occurrence and progression of infection, guide antibiotic application and predict mortality rate. 26 In an animal experiment, 18 at 120 min, the level of PCT was significantly statistical different in comparison with the control and simple group (p < .05). In another clinical research, 23 PCT was an independent predictor of tissue ischemia and necrosis with significantly statistical differences in the ischemia group (p = .009) and the necrosis group (p = .005). In ischemia and necrosis group, the AUCs of PCT were 0.77 and 0.87, respectively. In addition, the PCT cutoff levels at ≥0.25 ng/mL for predicting ischemia yielded 72% sensitivity and 73% specificity, as well as ≥0.25 ng/mL, 83% and 78% for necrosis, respectively. In our study, we found the highest AUC of 0.907 for PCT and the highest sensitivity of 86.4%. The results suggested that the PCT should be a useful inflammation indicator for discriminating the strangulated intestinal obstruction.
CRP is an acute reaction plasma protein and its concentration may signally increase in the severe inflammation. 27 The concentration of CRP can help diagnose strangulated intestinal obstruction and indicate its benign or malign origin. In the study of Li et al, 6 the value of the CRP was correlated to the degree of the ischemia and the type of intestinal obstruction. The AUC of the CRP was 0.78, with the sensitivity of 56.25% and the specificity of 94.44% in discriminating strangulated ileus. In another study, 28 there was no significant difference in CRP concentration between strangulation and non-strangulation group. In our research, the level of CRP is statistically significant between two groups. And we found that the AUC of CRP (0.681) was lower than PCT (0.907), SAA (0.723) and IL-6 (0.712). Moreover, the sensitivity of CRP was also significantly lower than specificity. Therefore, the usefulness of CRP remains to be discussed.
IL-6 is principally released by macrophages in response to pathogens or inflammation-associated molecular patterns. 29 The IL-6 was reported as a useful predictor for strangulation, with the sensitivity 86% and the specificity 95%. 21 In our study, the sensitivity and specificity were 68.20% and 76.90% with the AUC of 0.712. It can refer that the serum IL-6 is valuable diagnostic indicator of predicting strangulation.
SAA serves as a vital role in inflammation. And it is more conclusive for viral infections, severe acute pancreatitis, and rejection reactions for kidney transplants than CRP. 30 The SAA had widely used in clinical practice, such as atherosclerosis, 25 hepatitis, 31 sepsis, 32 breast cancer, 33 pulmonary fibrosis, 34 COVID-19 35 and giant cell arteritis. 36 For instance, except cases with the inactive chronic hepatitis B, patients with active liver diseases had higher plasma SAA concentration than the healthy control group, and the highest SAA level was detected in the patients with pyogenic liver abscess. 37 So, SAA can be used as a potential inflammatory marker. Strangulated intestinal obstruction correlates to the blood circulation disorder of the intestinal wall, which can lead to the acute ischemia and ultimately cause the intestinal necrosis and perforation. 14 In this process, the inflammation exists persistently. So, the increased concentration of serum SAA may be linked to the strangulation. In our study, elevated SAA concentration of patients with strangulated intestinal obstruction was statistically significant compared with the simple group. The cutoff values were set at 282.50 (59.10% sensitivity and 87.20% specificity) for SAA.
Our study also has several strengths. First, we collected fully detailed and real information of the patients in order to ensure the reality and credibility of the research. Second, we construct the strict including and excluding criterion to eliminate the factors that could influence the level of inflammatory indices as much as possible. Third, although the SAA, an effective indicator of the inflammation, had been used in the hepatitis, pneumonia, cancer and so on, there is no clinical research of SAA in identifying strangulated from simple intestinal obstruction. We firstly evaluated the significance of SAA for the identification of intestinal obstruction, and analyzed sensitivity, specificity and the optimal cutoff value. Fourth, diagnostic value of combined indicators was explored.
But in our study, only 61 patients were admitted. The few cases and the parameters with significant dispersion degree may lead to the statistical bias, such as the excessive specificity and sensitivity. In addition, in our study some patients had received the treatment on admission, such as the medicine, fasting, water-deprivation, intestinal decompression and exploratory laparotomy. On the one hand, treatment could lead to the remission and lower level of the parameters, on the other hand, the parameters level may rise after surgery due to the surgery trauma. In an animal experiment, after urgent abdominal surgery the SAA concentrations were significantly elevated in all cases. 38 Moreover, since PCT, SAA, CRP and IL-6 are linked to the inflammation, the higher concentrations of the indicators may result from basic diseases that already exist for a long time, such as the gastric ulcer, chronic gastric and COPD.
Conclusions
We conclude that the PCT and combined indicators are sensitive and specific to identify the strangulation from the simple in patients suffering from intestinal obstruction. For discriminating strangulated intestinal obstruction from simple intestinal obstruction, PCT alone may be the preferred approach due to its simplicity. And the abnormal increase of serum inflammatory indicators levels in patients with intestinal obstruction suggests that strangulation may exist.
Footnotes
Acknowledgements
The authors would like to acknowledge the helpful comments on this paper received from the reviewers.
Authors contributions
R Zhang contributed to writing the article and statistical analysis; J Peng provided the financial support and the information of patients; ZQ Jin, RN Xu and ZM Ran collected the data, and draw the cartogram; Y Sun and L Lang offered administrative support; J Tao revise article and provided the statistical analysis and administrative support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Research Project of Nursing Department of Children’s Hospital of Chongqing Medical University, China (CHCQMU2021.09) and the Scientific Research and Innovation Experiment Project of Chongqing Medical University, China (SRIEP 202035).
Ethics approval
All research protocols were approved by Chongqing University Central Hospital (no.2022-14) and in accordance with the Declaration of Helsinki.
Informed consent
Informed consent was not sought for the present study because this is a retrospective study, this requirement was waived by the Ethics Committee.