
Abstract
To analyze the diagnostic value of CD40 ligand (CD40L), soluble growth stimulating expression gene 2 protein (ST2), interleukin-6 (IL-6), and C-reactive protein (CRP) are used in patients with acute coronary syndrome (ACS). Serum samples were collected from 259 ACS patients admitted to our hospital. Additionally, 119 healthy individuals who received physical examination in the hospital at the same time period were included as normal control. The levels of CD40L, ST2, IL-6, and CRP in 259 patients with ACS and 119 healthy subjects were detected by ELISA. The levels of CD40L, ST2, IL-6, and CRP were significantly increased in unstable angina (UA) patients, while ST2, CRP, and IL-6 were significantly elevated in acute myocardial infarction (AMI) patients. Pearson correlation analysis showed that ST2 was also closely related to CRP in ACS patients, while ST2 was positively correlated with creatine kinase (CK), creatine kinase isoenzyme (CK-MB), and troponin I (cTnI) in AMI patients. The levels of glucose (GLU) and low-density lipoprotein cholesterol (LDL-c) were significantly decreased, while the levels of high-density lipoprotein cholesterol (HDL-c) were significantly increased in AMI patients treated with stent implantation. Furthermore, the level of serum CD40 L was significantly elevated in coronary heart disease (CHD) patients treated with stent implantation, while the levels of ST2 and IL-6 in AMI patients treated with the stent implantation decreased significantly. The levels of inflammatory factors significantly changed in patients with ACS. These inflammatory factors may involve in the pathological progression of ACS and can be used as diagnostic indexes for ACS.
Keywords
Introduction
Acute coronary syndrome (ACS) refers to a group of clinical syndromes associated with rupture or invasion of coronary atherosclerotic plaque and secondary to complete or incomplete occlusive thrombosis, including unstable angina (UA) pectoris and acute myocardial infarction (AMI). It is characterized by pathophysiological changes of coronary arteries such as fat accumulation, fibrosis, and inflammatory response. To our best knowledge, several cytokines and immune cells, including IL-2, IL-6, IFN-γ, TNF-α, T lymphocytes, and mononuclear macrophages, 1 are reported to involve in the pathological processes. Apart from monocytes, T lymphocytes also play an important role in the pathogenesis of ACS. T cells are rare in arterial intima of normal individuals; however, the numbers of T cells show significant increase in the arterial intima of patients with atherosclerosis-related diseases. 2 To date, creatine kinase (CK), creatine kinase isoenzyme (CK-MB), and troponin I (cTnI) or T (cTnT) have been commonly used as serological markers for the diagnosis of such disease in clinical settings, but their levels show no elevation until AMI. In addition, other markers such as hepatocyte growth factor, soluble Fas, Fas ligands, chemokines, and high-density lipoprotein cholesterol (HDL-c) are still adequate for the risk assessment of ACS. 3 In view of the importance of immune and inflammation in the pathogenesis of coronary atherosclerosis, expression of serum inflammatory factors may serve as a new biomarker for the clinical diagnosis of ACS.
Soluble CD40L (sCD40L) is a soluble form of leukocyte differentiation antigen 40 ligand and is an important marker for the evaluation of platelet activation.4,5 Nowadays, CD40/CD40L has been reported to be closely related to vulnerable plaque rupture. As is known to all, CD40 and CD40L are expressed in AS-related cells including endothelial cells, vascular smooth muscle cells, monocytes or macrophages, T lymphocytes, and platelets. The expression of CD40 and CD40L is up-regulated in both ASC patients and experimental atherosclerotic plaques. 6
As a member of the interleukin-1 receptor family, suppression of tumorigenicity 2 (ST2) is a myocardial protein produced by myocardial cells under biomechanical stress. 7 Recently, ST2 level is considered to be associated with the severity of cardiac failure, left ventricular ejection fraction, brain natriuretic peptide, B-type brain natriuretic peptide, and creatinine clearance. 8 Therefore, it may serve as a marker for evaluating the progression of myocardial fibrosis. Interleukin-6 (IL-6) and C-reactive protein (CRP) are the markers of inflammation. IL-6 can be produced by various cells such as macrophages, T cells, and B cells. IL-6 involves in the proliferation and differentiation of a variety of cells, immune response, acute phase reaction, hematopoietic function, and anti-infective immune response. On this basis, it plays an important role in immune response, bone marrow hematopoiesis, and inflammatory response. In clinical settings, IL-6 concentration in body fluids can reflect changes in the patient’s condition. CRP is a sharply rising protein, also termed as acute phase protein, in the plasma in the presence of infection or tissue or organ damages. It can activate the complement and enhance the phagocytosis of phagocytic cells to clear the pathogenic microorganisms and necrotic or apoptotic cells. Furthermore, levels of IL-6 and CRP were significantly elevated in patients with ACS, 9 which could be used as a marker to assess the progression and prognosis of ACS.
In this study, T cell activation–related inflammatory factors, including CD40L, ST2, IL-6, and CRP, were selected to analyze their changes and clinical significance in the pathogenesis and prognosis of ACS. Our study contributed to the evaluation of progression and risk of ACS.
Materials and methods
Sample size
The main objective of this study was to investigate the diagnostic value of CD40 ligand (CD40L), soluble growth stimulating expression gene 2 protein (ST2), IL-6, and C-reactive protein (CRP) in patients with ACS. Among them, the area under the curve (AUC) of CD40L was the smallest according to the pre-experimental results. Therefore, we chose CD40L as the indicator for sample size calculation. The sample size parameters (power = 0.90, alpha = 0.05, N+:N- = 1:1, AUC0 = 0.5, AUC1 = 0.65, lower FPR = 0.00, and upper FPR = 1.00) were set according to the pre-experiment results of CD40L, and the PASS 11.0 software was used to calculate the sample size. The results showed that at least 41 ACS patients and 41 healthy individuals were needed.
Patients
The study protocols of this retrospective study were approved by the Ethics Committee of Taizhou People’s Hospital (No. KY201917501). Written informed consent was obtained from all subjects before the study.
In the experiment group, serum samples were collected from 259 ACS patients admitted to the Taizhou People’s Hospital (Jiangsu, China) from June 2019 to September 2019. Among the 259 ACS patients, 147 were confirmed with UA, 56 with AMI, and 56 with AMI stent implantation, respectively. We declare that all these diagnoses were based on the diagnosis criteria of the Center for Human Development (CHD). Inclusion criteria were as follows: cases of coronary heart disease (CHD) in patients who were diagnosed and treated at Jiangsu Taizhou People’s Hospital; diagnoses that were confirmed through coronary angiography; and coronary arteriography that was performed to observe the angiostenosis. The stent could be implanted if the degree of angiostenosis was over 75%. Exclusion criteria were as follows: patients with heart diseases including congenital heart disease, valvular disease, cardiomyopathy, and combining severe ventricular dysfunction; patients who were attacked by autoimmune disease, acute or chronic infectious diseases, or allergic dermatitis; patients who suffered from renal insufficiency, blood system diseases, digestive system disease, or hepatic disease; cancer patients or patients with thyroid dysfunction except those with normal thyroid hormone level measured at admission; patients who had history of trauma or surgery recently; and patients who took medicines including glucocorticoid or immunosuppressor within the last month. In the control group, 119 patients were normal in cardiac markers, ECG after admission, and examination of coronary angiogram, as well as had no history of coronary heart disease.
Serum sample collection
Serum samples were collected from the venous blood of ACS patients and healthy control in the morning. The samples were stored at −80°C for until further analysis.
ELISA analysis
ST2 concentration was determined by using a commercial ELISA kit (Critical Diagnostics Inc.,) according to the manufacturer’s protocols. Human sCD40L ELISA kit was provided by Bright Scistar Tech (Suzhou, China). The plates were blocked with 2% bovine serum albumin at room temperature for 1 h. The dilution of the standard fusion protein and serum samples was added to the wells and incubated at room temperature for 2 h. Afterward, the biotin-labeled monoclonal antibodies (0.5 μg/mL, 100 μL/well) were added to the wells and were incubated at room temperature for 1 h. Then, the plates were incubated with streptavidin-HRP (1:8000, 100 μL/well) at room temperature for 1 h. After washing with PBS 8 times, HRP reaction substrate TMB (100 μL/well) was added to the wells. The absorbance was measured at OD450 nm by a microplate reader.
Biochemical indicators’ determination
Blood glucose (GLU), total cholesterol, triglyceride, low-density lipoprotein cholesterol (LDL-c), high-density lipoprotein cholesterol, and CRP detection reagents were measured using a Beckman Coulter 5800 automatic biochemical analyzer (Beckman, CA, USA). IL-6 level was analyzed by using upward luminescence method (Hotgen Biotech, Beijing, China) and detected on the UPT-3A up-conversion luminescence analyzer (Hotgen Biotech, Beijing, China).
Statistical analysis
Statistical analysis was performed using SigmaPlot 12.0 software. The normal distribution data in the text were reported as mean ± standard deviation. The data were represented that were not normally distributed were presented as median (25%–75%). Student’s t-test or nonparametric Mann–Whitney U test was used for two independent samples. Chi-square test was used to compare the ratio of female to male. Pearson correlation analysis was used to evaluate correlations between the selected four indices and the laboratory indices. One-way ANOVA was performed to compare means of more than two groups. p < 0.05 was considered to be statistically significant. ROC curvature was utilized to analyze the efficiency of CD40L, ST2, IL-6, and CRP in the diagnosis of ACS.
Results
Patients’ characteristics
Clinical characteristics of patients with UA or AMI.

HS: healthy subject; *Compared with HS, p<0.001; †Compared with UA; p<0.001.
AMI, acute myocardial infarction; UA, nustable angina; GLU, glucose; TG, triglyceride; HDL-c, high-density lipoprotein cholesterol; LDL-c, low-density lipoprotein cholesterol.
The difference of serological CD40L, ST2, CRP, and IL-6 levels among healthy subjects, UA patients, and AMI patients
The difference of serological markers among healthy subjects, UA patients, and AMI patients.

*Compared with HS, p < 0.05; †Compared with UA; p < 0.05.
HS: healthy subject; AMI, acute myocardial infarction; UA, unstable angina; IL-6, interleukin-6; CD40L, CD40 ligand.
The correlation between ST2 and other serumal markers in patients with ACS
Person correlation analysis showed that ST2 was positively correlated with CRP in ACS patients (r=0.234, p<0.01, Figure 1(a)). ST2 was also positively correlated with CK (r = 0.297, p < 0.05), CK-MB (r = 0.289, p < 0.05), and CTNI (r = 0.318, p < 0.05) in ACS patients (Figures 1(b) and (c)). There was no correlation between ST2 and other indices (p > 0.05). These results demonstrated that ST2 level was associated with the inflammatory response in patients with ACS. Correlation analysis between ST2 and inflammatory factors in ACS patients. (a) ST2 was positively correlated with CRP in ACS patients (r = 0.234, p < 0.01). (b) ST2 was positively correlated with CK in AMI patients (r = 0.297, p < 0.05). (c) ST2 was positively correlated with CK-MB in AMI patients (r = 0.289, p < 0.05). (d) ST2 was positively correlated with CTNI in AMI patients (r = 0.318, p < 0.05).Note: CRP: C-reactive protein; ACS: acute coronary syndrome; AMI: acute myocardial infarction.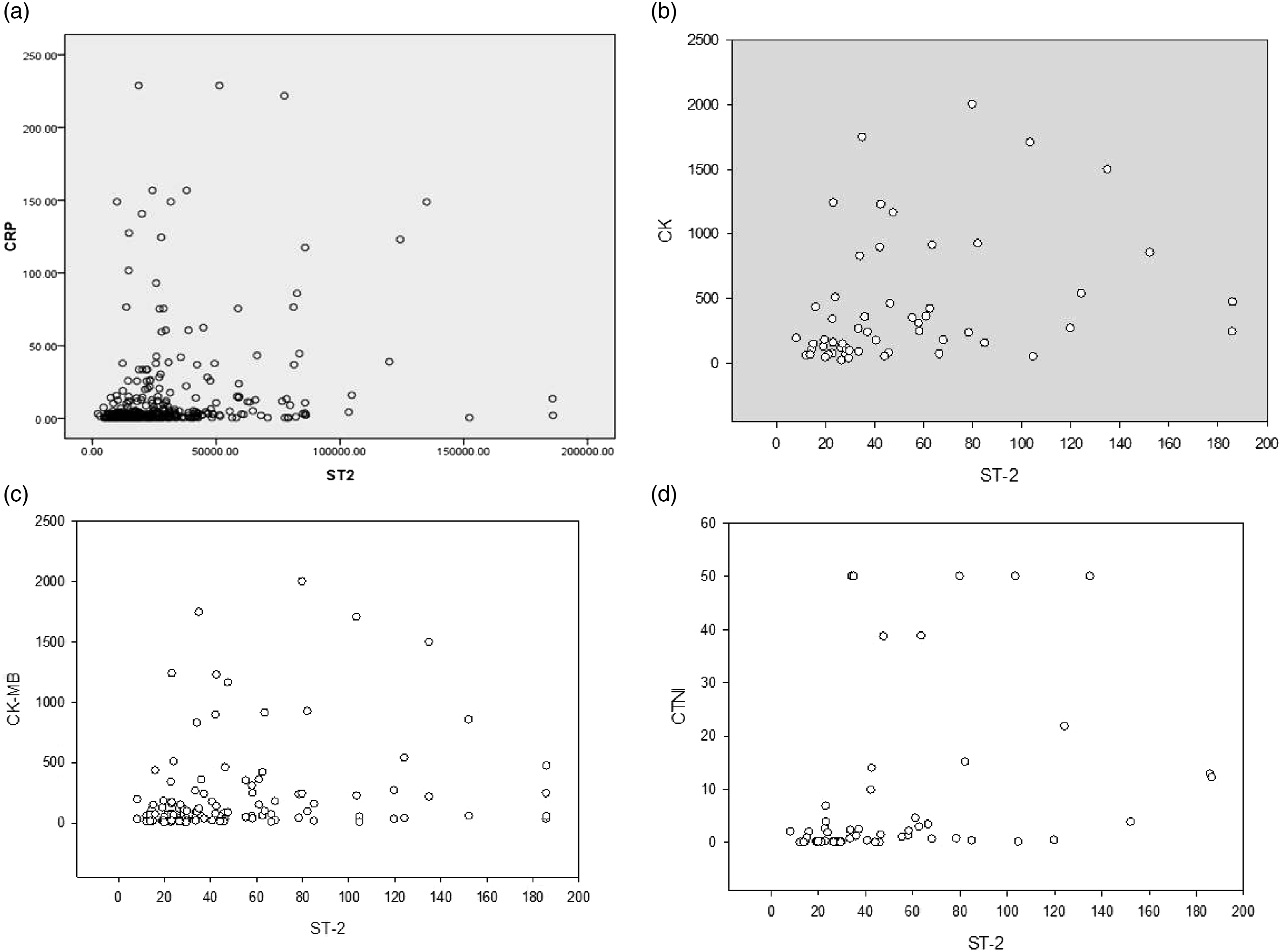
The diagnostic value of serum CD40L, ST2, IL-6, and CRP for ACS
We further analyzed the diagnostic value of CD40L, ST2, IL-6, and CRP for ACS. Our results showed that ST2 demonstrated the highest sensitivity (92.2%), followed by CRP (75.2%) and CD40L (77.5%, Figure 2 and Table 3). CRP demonstrated the highest specificity (100%), followed by ST2 (72.9%, Figure 2 and Table 3). The results indicated that these indicators were efficient for ACS diagnosis. In addition, ST2, CD40L, and CRP were independent risk factors for CHD (p < 0.01), with the OR values of 2.959, 5.612, and 22.438, respectively. The receiver operating characteristic (ROC) curve analysis for discriminative ability between ACS cases and healthy subjects enrolled in the training and validation sets by the ST2, CD40L, CRP, and IL-6 levels. Note: CRP: C-reactive protein; ACS: acute coronary syndrome. The diagnostic value of ST2, CD40L, CRP, and IL-6 for ACS. CD40L, CD40 ligand; CRP, C-reactive protein; IL-6, interleukin-6; ACS, acute coronary syndrome.

Clinical significance of serum metabolic markers and inflammatory factors in AMI patients treated with stent implantation
The difference of serological markers in AMI patients treated with or without stent implantation.
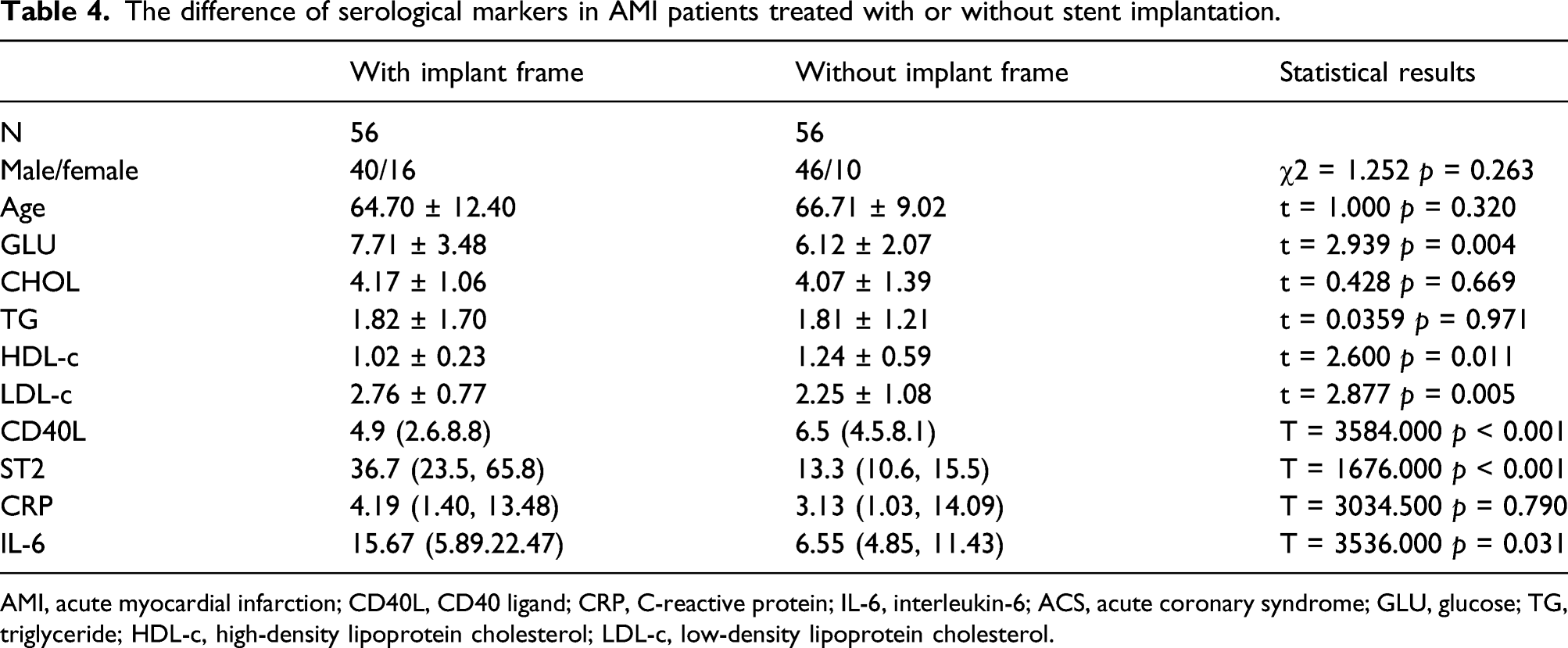
AMI, acute myocardial infarction; CD40L, CD40 ligand; CRP, C-reactive protein; IL-6, interleukin-6; ACS, acute coronary syndrome; GLU, glucose; TG, triglyceride; HDL-c, high-density lipoprotein cholesterol; LDL-c, low-density lipoprotein cholesterol.
Discussion
Inflammatory factors including CD40L and ST2 are related to T cell activation. As a member of the IL-1 receptor family, ST2 is the ligand for IL-33. To date, there are two major subtypes for ST2, including the transmembrane ST2 and soluble ST2 (sST2). IL-33 and its receptor play an important role in heart protection and contribute to prevention of cardiomyocytes hypertrophy and apoptosis. Upon binding with IL-33, sST2 could inhibit the function of IL-33, resulting in an increase in cardiovascular stress and fibrosis. The sST2 promoted the myocardial fibrosis and might trigger the cardiac failure. The concentration of sST2 in serum was associated with the severity of cardiac failure. 8 Previous studies demonstrated that the elevated sST2 levels were associated with acute and chronic cardiac failure.10–12 Moreover, the levels of sST2 were related to the increased mortality of patients. 13 Our data showed that the levels of sST2 were significantly elevated in patients with UA or AMI. In addition, the sST2 levels were significantly decreased in AMI patients after stent implantation (p < 0.001). For the reason, it may be related to the fact that stent implantation could significantly contribute to the myocardial blood supply and myocardial fibrosis. This indicated that stent implantation could significantly improve the progression of cardiac fibrosis.
CD40L is mainly expressed on T lymphocytes, B lymphocytes, and platelets in the healthy population. It has been well acknowledged that CD40L is not expressed in normal arteries, and only a small amount of CD40L is expressed in the vascular endothelium cells. According to the previous studies, 14 CD40 and CD40L were expressed on endothelial cells, vascular smooth muscle cells, monocytes/macrophages, T lymphocytes, and platelets of coronary atherosclerosis (AS) patients. Moreover, CD40 and CD40L levels were up-regulated in AS patients and experimental atherosclerotic plaques. 6 CD40L is not expressed on the surface of static platelets. Upon activation of platelets by thrombin, adenosine diphosphate (ADP), or collagen, CD40L can be expressed on the surface of platelets. 15 Upon expression of CD40L on the surface of platelet membrane, CD40L could fall into the blood to form soluble CD40L (sCD40L). As the active form of CD40L, more than 95% of sCD40L in circulating blood is derived from activated platelets.16,17 CD40L could up-regulate P-selectin expression in platelets, which suggested that elevated CD40L may be one of the mechanisms of platelet activation. 18 As an important ligand of inflammatory signaling pathway, CD40L is closely involved in the pathogenesis of atherosclerosis. Previous studies showed that CD40L could bind to its receptors on macrophage surface and promote the secretion of inflammatory factors during infection, atherosclerosis, and myocardial infarction.19–21 In this study, the sCD40L level was significantly higher in UA patients than that of healthy control. This may be caused by platelet activation. With the prolongation of disease course, the platelets are continuously activated, resulting in decline of cardiac sCD40L level during the progression of atherosclerosis. Moreover, sCD40L binds to CD40 on the surface of monocytes, promotes the migration of monocytes to coronary atherosclerosis, and simultaneously activates mononuclear macrophages to release a large number of inflammatory factors. Meanwhile, sCD40L binds to a large number of T cells and macrophages under the plaque, causing macrophages to release a large amount of metalloproteinases together with the thinning of the fibrous cap and plaque rupture. Stent implantation can improve the depletion state of platelet SCD40L. Additionally, with the saturation of CD40 on the surface of macrophages in the fiber cap, the levels of sCD40L are up-regulated.
Extensive efforts have been paid to the identification of serum markers for the acute coronary atherosclerosis. In the ACS patients, there was significant elevation in the IL-6 and CRP that were associated with the myocardial ischemia and injury. They were considered as effective markers for ACS diagnosis. 22 In addition, there was significant elevation in the IL-6 in AMI patients, and evaluation of IL-6 contributed to the diagnosis of AMI. 23 Soluble ST2 could be used for the stratified analysis and diagnosis of cardiovascular diseases, together with acute heart failure and type 1 and type 2 AMI. 24 . Among the ACS patients, there was significant elevation in the CRP and sCD40L. The concentration of markers in the systemic circulation could directly reflex the concentration of markers in local coronary circulation. These markers may be effective for the prediction of plaque vulnerability. 25 Nevertheless, in a previous study, sCD40L was not proved as a diagnostic index for acute heart disease, cerebrovascular ischemia, or thromboembolic events. 26 In this study, we analyzed the diagnostic value of CD40L, ST2, IL-6, and CRP for ACS. Our data indicated that ST2 showed the highest sensitivity (92.2%), followed by CRP (75.2%) and CD40L (77.5%). CRP demonstrated the highest specificity (100%), followed by ST2 (72.9%). In general, these indicators showed good diagnostic value for ACS diagnosis.
In addition, the levels of CD40L showed significant increase in AMI patients who received stent implantation compared with that of the normal control, while significant decline was noticed in the ST2 and IL-6 levels in these patients. Stent implantation caused inflammatory response and platelet activation, which resulted in the elevation of CD40L. Although anti-inflammatory drugs were used, their levels were still higher than that before stent implantation. Anti-inflammatory agents led to significant decrease of IL-6 in AMI patients treated with stent implantation. ST2 is a kind of cardiac muscle protein which produces when myocardial cells are subjected to biomechanical stress. Recent studies showed that the concentration of ST2 is related to the severity of heart failure. Therefore, the decreasing ST2 concentration may mean that the myocardium blood flow was improved due to the implanted stent. Thus, the myocardial function was improved too. Therefore, the significance of these indicators in AMI patients treated with stent implantation remains to be further studied.
There are some limitations in this study. In this study, we only analyzed the differences of CD40L, ST2, IL-6, and CRP between AMI group and AMI stent group. In future studies, we will focus on the follow-up of the AMI patients who received stent implantation and investigate these indices on the efficiency of stent implantation.
Conclusion
Significant elevation was noticed in the CD40L, ST2, IL-6, and CRP in the peripheral blood of the ACS patients of various stages. After stent implantation, their levels may decline to some extent. ST2 was an important inflammatory factor for disease progression and myocardial damage. ST2 and CD40L showed satisfactory sensitivity, while CRP and IL-6 showed satisfactory specificity. CD40L, ST2, and CROP were the risk factors for the ACS. A comprehensive analysis to the inflammatory factors may contribute to the evaluation of the progression and risk of ACS.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Taizhou People’s Hospital Medical Innovation Team Foundation, China (CXTDB201904), 2019 Taizhou People’s Hospital Mandatory Project (No. ZL201904). 2020 Taizhou People’s Hospital Mandatory Project (No. ZL202022).
Ethics approval
Ethical approval for this study was obtained from the Ethics Committee of Jiangsu Taizhou People’s Hospital (No. KY201917501).
Informed consent
Written informed consent was obtained from all subjects before the study.
Contributorship
ZL wrote the manuscript; YJ revised the manuscript; ZCM, MGY did the data analysis; XJ, QJY, JLZ did the data collection.
Data availability
All the data were available upon appropriate request.