
Abstract
The aim of this study was to evaluate the relationship between T helper type 17 (Th17) cells and Kawasaki disease (KD). Flow cytometry results showed that the number of Th17 cells in the peripheral blood mononuclear cells (PBMCs) of KD patients was significantly elevated. Enzyme-linked immunosorbent assay (ELISA) results showed that the serum concentrations of two Th17 cytokines, interleukin (IL)-17 and IL-6, were significantly increased in KD patients. In addition, real-time quantitative polymerase chain reaction (PCR) results showed that the messenger RNA (mRNA) expression of two molecules related to Th17 cell differentiation, retinoic acid–related orphan receptor C (RORC) and NR4A2, was upregulated in the CD4+ T cells of KD patients. Intravenous immunoglobulin (IVIG) infusion significantly reduced the proportion of Th17 cells, decreased serum concentrations of IL-7 and IL-6, and lowered the mRNA levels of RORC and NR4A2 in IVIG treatment–sensitive KD patients. Finally, the results of a Pearson’s correlation analysis illustrated that IL-17 mRNA levels in CD4+ T cells of KD patients were positively correlated with NR4A2 but not RORC mRNA expression. Our results demonstrate that Th17 cells play an important role in KD development and IVIG treatment and that Th17 cells and IL-17 may be used as markers for the occurrence of KD or as treatment targets for KD therapies. In addition, our results suggest that the underlying mechanism of IL-17 production in KD is NR4A2 dependent.
Introduction
Kawasaki disease (KD) is an acute multisystem vasculitis, and the most serious complication of KD is coronary artery lesions (CALs). 1 The suggested global standard treatment for KD is a high dose (2 g/kg) of intravenous immunoglobulin (IVIG) infusion. However, some IVIG-resistant (IVIG-R) patients (approximately 10%–15%) cannot benefit from IVIG treatment. 2 Until now, the immunopathogenesis of KD and the pharmacological mechanisms of IVIG were not fully understood.
T helper type 17 (Th17) cells represent a subset lineage of CD4+ T cells that are distinct from Th1 and Th2 cells. 3 Important features of Th17 cells include their ability to produce interleukin (IL)-17, including IL-17A and IL-17F, as well as express the lineage-specific transcription factor retinoic acid–related orphan receptor C (RORC). 4 Inflammatory cytokines, such as IL-6, IL-21, IL-1, and IL-23, play central roles in the generation of IL-17. Moreover, NR4A2 (nuclear receptor subfamily 4 group A member 2), an orphan nuclear receptor, is strikingly overexpressed by infiltrating Th17 cells in several autoimmune diseases and enhances nonspecific production of Th17 cytokines. 5 Increasing evidence has shown that Th17 cells and their effector molecules are associated with the pathogenesis of several autoimmune and inflammatory diseases. 6 Nevertheless, reports regarding the association of Th17 with KD are limited.
Therefore, we observed alterations in Th17 cells and Th17 cytokines before and after IVIG treatment. Our results demonstrate that Th17 cells play an important role in KD development and IVIG treatment. In addition, our results suggest that the underlying mechanism of IL-17 production in KD is NR4A2 dependent.
Materials and methods
Patients
In total, 38 children with an acute febrile stage of KD, 12 age-matched children with active infectious diseases (IDs), and 8 age-matched healthy volunteers (determined from a routine health examination) were enrolled in this study at Xi’an Children’s Hospital (Xi’an, China). KD was diagnosed in any child with a fever that lasted longer than 5 days and manifested four of the following five criteria: diffuse mucosal inflammation with strawberry tongue and fissure lips, bilateral nonpurulent conjunctivitis, indurative angioedema of the hands and feet, dysmorphic skin rashes, and unilateral cervical lymphadenopathy. 7 CAL formation in KD children was determined by two-dimensional echocardiographic examination. CALs were defined as having an internal diameter of the coronary artery greater than 3 mm (age less than 5 years) or greater than 4 mm (age greater than 5 years) or having an internal diameter of a segment at least 1.5 times greater than that of an adjacent segment.8,9 All KD children received a single dose of IVIG (2 g/kg) administered over an 8- to 12-h period. Low-dose aspirin (3–5 mg/kg/day) was administered until all inflammation signs were resolved or until the CAL regressed.
Blood samples of all participants were collected after written informed consent was obtained from their parents or guardians. Blood samples of the KD children were collected before and 10 days after IVIG treatment. IVIG responsiveness (IVIG sensitivity) was defined as fever reduction within 48 h after the initial IVIG treatment and no reoccurrence of fever (>38°C) for 7 or more days.
Flow cytometry
Blood samples (5 mL) were anticoagulated with heparin, and peripheral blood mononuclear cells (PBMCs) were separated using a lymphocyte separation medium (Corning Life Sciences, New York, NY). PBMCs were then suspended at a density of 2 × 106 cells/mL and washed once in phosphate-buffered saline (PBS). Phycoerythrin (PE) antihuman CD4 antibody (Cell Signaling Technology (CST), Danvers, MA) and FITC antihuman IL-17A antibody (CST) were used to detect the proportion of Th17 cells. A permeabilization procedure was conducted before IL-17A antibody staining according to the manufacturer’s instructions. Flow cytometry (FCM) analysis was performed using an EPICS XL-4 cytometer equipped with EXPO32 ADC software (Beckman Coulter, San Diego, CA).
Enzyme-linked immunosorbent assay
Serum of each blood sample (0.5 mL) without anticoagulation was separated using a pipette after the blood clotted (4°C, overnight) and stored at −80°C until use. The levels of IL-17 and IL-6 in the serum were determined in triplicate using human enzyme-linked immunosorbent assay (ELISA) kits (R&D, Minneapolis, MN) according to the manufacturer’s instructions.
Real-time quantitative polymerase chain reaction (qRT-PCR)
CD4+ T cells were sorted and collected during FCM analysis of PBMCs. All the RNA from the sorted CD4+ T cells was isolated using TRIzol reagent (Life Technologies, Gaithersburg, MD) and then reverse-transcribed using an iScript complementary DNA (cDNA) synthesis kit (Bio-Rad, Hercules, CA). Real-time quantitative polymerase chain reaction (qRT-PCR) was performed using iTaq Universal SYBR Green Supermix (Bio-Rad) on a polymerase chain reaction (PCR) system (7500; Applied Biosystems, Waltham, MA). Relative messenger RNA (mRNA) expression levels of RORC, NR4A2, IL-17A, IL-17F, and β-actin (the internal control) were detected using the following primers: RORC: 5′-CCGCTGAGAGGGCTTCAC-3′ (forward), 5′-TGCA GGAGTAGGCCACATTACA-3′ (reverse); IL-17A: 5′-CAGATTACTACAACCGA TCC-3′(forward), 5′-CATGTGGTAGTCCACGTTCC-3′ (reverse); IL-17F: 5′-CC GTTCCCATCCAGCAAGAG-3′ (forward), 5′-ACAGTCACCAGCACCTTCTC-3′ (reverse); NR4A2: 5′-CGACATTTCTGCCTT CTCC-3′ (forward), 5′-GGTAAAGT GTCCAGGAAAAG-3′ (reverse); and β-actin: 5′-AGAGGGAAATCGTGCGTG AC-3′ (forward), 5′-CAATAGTGATGACCTGGCCGT-3′ (reverse).
Statistical analysis
SPSS software Windows version 11.0 (SPSS, Chicago, IL) was used for the statistical analysis. The data are presented as the means ± standard deviation (SD). Differences between the values were determined using Student’s t-test or a one-way analysis of variance (ANOVA). For analyzing the correlation, we used a two-sided Pearson’s test. A value of P < 0.05 was regarded as statistically significant.
Results
Patient characteristics
Between December 2014 and May 2016, 38 patients with KD, 12 patients with ID, and 8 age-matched healthy volunteers were enrolled in this case–control study. The patient characteristics are summarized in Table 1. Among the KD participants, 14 patients (36.8%) had CAL formation (KD-CAL+) and 5 patients (13.2%) were IVIG-R. Among the ID cohort, five patients were diagnosed with measles and seven with influenza. No significant differences in age or gender were found between the KD and ID patients. In addition, the age distribution of KD patients with or without CAL showed no significant differences (KD-CAL+ vs KD-CAL−, P > 0.05). Similarly, the age distribution of IVIG-sensitive (IVIG-S) and IVIG-R KD patients showed no significant differences (IVIG-S vs IVIG-R, P > 0.05). Blood samples of KD patients were collected before and 10 days after IVIG treatment.
Demographic data of Kawasaki disease patients and control subjects.

CAL+, coronary artery lesion–positive; IVIG-R, intravenous immunoglobulin treatment resistant.
Comparisons were conducted with an unpaired t-test between the Kawasaki disease cohort and the febrile cohort or healthy volunteers. All P values are two sided.
The proportion of Th17 cells in PBMCs are increased in KD patients
In the FCM analysis, the concurrent expression of CD4+ and IL-17A+ was used to determine the proportion of Th17 cells in the PBMCs of all cohorts. The average Th17 proportion in the PBMCs of the KD children was significantly higher than that of the ID children and the volunteers (Figure 1(a)). The KD children had the highest Th17 proportion in the PBMCs. Moreover, the Th17 proportion of the KD children with CAL formation (KD-CAL+) was significantly higher than that of the KD children without CAL formation (KD-CAL−; Figure 1(b)).
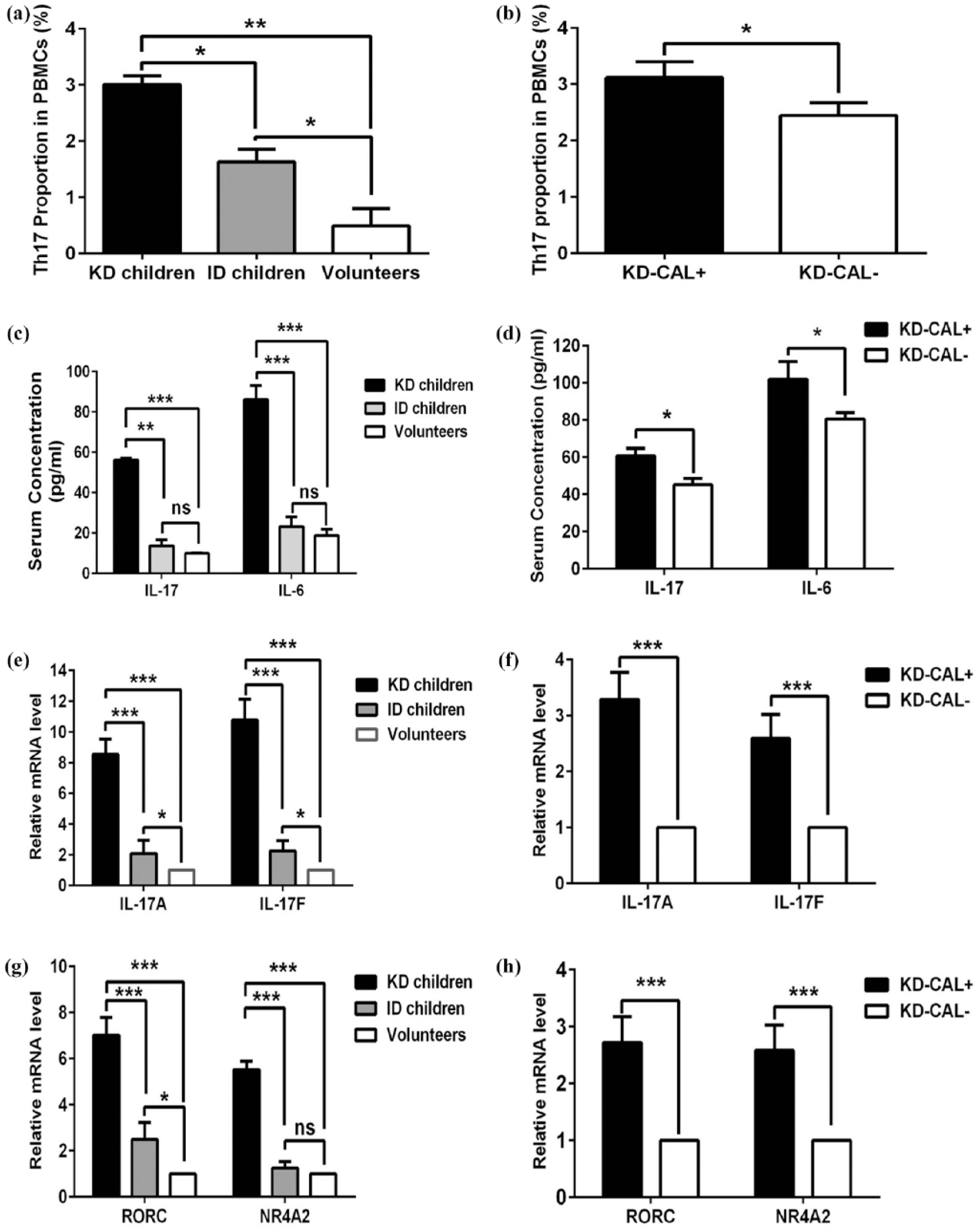
(a and b) The proportion of Th17 cells in peripheral blood mononuclear cells (PBMCs) increases in Kawasaki disease (KD) patients. (c–f) Th17 cytokines are increased in Kawasaki disease (KD) patients. (g and h) Molecules related to Th17 cell differentiation are increased in Kawasaki disease (KD) patients.
IL-17 and IL-6 are increased in KD patients
Serum concentrations of Th17 cytokines (IL-17 and IL-6) were determined by ELISA. The results showed that the serum concentrations of IL-17 and IL-6 in KD children were both significantly higher than those of the ID children or the volunteers. No significant differences were detected between the ID children and the volunteers (Figure 1(c)). Similarly, serum concentrations of IL-17 and IL-6 in KD children with CAL formation (KD-CAL+) were significantly higher than those in KD children without CAL formation (KD-CAL−; Figure 1(d)).
The mRNA levels of IL-17A and IL-17F in CD4+ T cells of the patients were evaluated by qRT-PCR. Compared to ID children and healthy volunteers, both IL-17A and IL-17F mRNA levels increased significantly in KD children (Figure 1(e)). In addition, CAL formation in KD children (KD-CAL+) was accompanied by higher IL-17A and IL-17F mRNA levels (Figure 1(f)).
The mRNA levels of RORC and NR4A2 are increased in KD patients
The mRNA levels of RORC and NR4A2, two important molecules involved in the differentiation of Th17 cells from CD4+ T cells, were determined by qRT-PCR. Both RORC and NR4A2 were significantly elevated in KD children compared to ID children and volunteers (Figure 1(g)). In addition, CAL formation in KD children (KD-CAL+) was accompanied by higher RORC and NR4A2 mRNA levels (Figure 1(h)).
Changes in Th17 cells, Th17 cytokines, and related molecules are inhibited by IVIG treatment in KD-sensitive patients
After IVIG treatment, the proportion of Th17 cells in PBMCs, the serum concentrations of IL-17 and IL-6, and the mRNA levels of RORC and NR4A2 in CD4+ T cells were investigated by FCM, ELISA, and qRT-PCR, respectively. In IVIG-S children (n = 33), IVIG treatment significantly decreased the proportion of Th17 cells in PBMCs, reduced the serum levels of IL-17 and IL-6 (Figure 2(a)), and inhibited the mRNA levels of RORC and NR4A2 in CD4+ T cells (Figure 2(b)). In IVIG-R patients (n = 5), no such inhibition effects were observed (Figure 2(a) and (b)). In addition, compared with IVIG-S patients, the clinical manifestations of IVIG-R patients showed no improvement (Table 2).

IVIG treatment in KD-sensitive patients decreases the proportion of Th17 cells, Th17-related cytokines, and mRNA levels of RORC and NR4A2.
Clinical manifestations of KD patients before and after intravenous immunoglobulin (IVIG) infusion.

KD: Kawasaki disease; WBC: white blood cell; Hb: hemoglobin; Alb: serum albumin; LDH: lactate dehydrogenase.
P < 0.05 compared with the values of sensitive patients before IVIG treatment. The hematological index displays only the changed items.
IL-17 mRNA expression is positively related with that of NR4A2 but not RORC in KD patients
The relationship of IL-17, NR4A2, and RORC mRNA levels in each KD patient was analyzed. The results showed a significant positive correlation between mRNA levels of IL-17 and NR4A2 (Figure 3(a), two-sided Pearson’s correlation, R = 0.605, P < 0.01) but not between IL-17 and RORC (Figure 3(b), R = 0.165, P > 0.05). This preliminary analysis suggests that NR4A2 is required for the production of IL-17 in Th17 cells of KD patients, and the underlying mechanism is independent of RORC.

IL-17 mRNA expression is positively related with NR4A2 (a) but not RORC (b) in KD patients.
Discussion
In this study, we first investigated the proportions of Th17 cells in PBMCs in patients with KD. Our results showed that the proportions of Th17 cells significantly increased in children with KD when compared to healthy volunteers and children with other IDs. Importantly, the frequencies of Th17 cells were higher in the KD-CAL+ group than those in the KD-CAL− group. Our current study showed that Th17 cells play a crucial role in KD development and imply that a greater proportion of Th17 cells is associated with the exacerbation of KD.
IL-17 plays an important role in autoimmune diseases and Th17 functions. 10 Therefore, we assessed the plasma concentrations of IL-17 and IL-6 in patients with KD. As expected, the plasma concentrations of IL-17 and IL-6 in patients with KD were remarkably higher than those in healthy volunteers and in children with other IDs. In addition, the mRNA levels of IL-17A and IL-17F also increased in KD patients. Importantly, no significant differences were detected between IL-17 serum concentrations of ID children and those of the volunteers. These results illustrate that Th17 cells exert their function by upregulating and secreting Th17-related cytokines and that a high level of serum IL-17 may be a marker for KD.
Currently, the effective strategy for KD is a high dose of IVIG infusion. 11 In this study, we compared the proportion of Th17 cells in patient PBMCs and serum concentrations of IL-17 and IL-6 before and after IVIG treatment. These data illustrate again that Th17 cells play a crucial role in KD development. Moreover, the results suggest that the effects of IVIG treatment are related to the inhibition of Th17 cells.
RORC is considered the most important molecule for the differentiation of Th17 cells, and NR4A2 plays an essential role in the development of Th17-mediated autoimmune disease.12–15 In this study, we evaluated both RORC and NR4A2 mRNA levels in KD patients compared to the control cohorts, and we analyzed the correlations between IL-17, RORC, and NR4A2 mRNA levels. The results showed that the levels of IL-17 mRNA were positively related to that of NR4A2 but not RORC. This preliminary result suggests that the underlying mechanism of IL-17 production in KD patients is related to NR4A2 but not RORC.
In summary, we found that the proportion of Th17 cells and the serum concentrations of Th17 cytokines were significantly elevated in KD patients. In IVIG-S patients, the treatment effectively inhibited the quantity and functions of Th17 cells. IL-17 production in KD patients was related to NR4A2 expression. Our results demonstrate that Th17 cells play an important role in KD development and suggest that Th17 cells could be a target for KD treatment. Moreover, our preliminary results indicate that the underlying mechanism of IL-17 production in KD is NR4A2 dependent.
Footnotes
Acknowledgements
C.C. and M.L. conceived and designed the experiments. K.Z. and Z.L. performed all experiments. S.W. and Y.Z. performed the collection of clinical samples and the collection of patient consent forms. K.Z. contributed reagents and materials and analyzed the data. M.L. wrote this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the National Natural Science Foundation of China (NSFC 81673020) and the Natural Science Basic Research Plan in the Shaanxi Province of China (2016SF256; 2016JM8096).