
Abstract
Background
Bedside insertion of peripherally inserted central venous catheter (PICC) is still needed in the various clinical settings. For this procedure, the accuracy of predicting the PICC catheter length is important, however, only a few methods have been proposed so far.
Purpose
A new formula using pre-procedural chest X ray (pre-CXR) was validated for placing the PICC catheter tip precisely in the actual clinical setting.
Material and Methods
The formula predicting the PICC catheter length was formed by the hybrids of the calculated expression in the thorax and the actual measurement of the outer arm. The predicted length in the thorax was based on the half ellipse formed by the three landmarks on the pre-CXR. Prospectively, this formula was applied in the 110 patients. The results were compared to those in the traditional anthropometrical measurements (TAM) in the 48 patients.
Results
The discrepancy of the catheter distance from the carina and the variance of the tip position were smaller by using the Formula than by the TAM (P = .00053 and P = .038). Comparing to the other patient’s valuables, the Formula had the strongest correlation coefficient with the true PICC length (r = 0.787). Evaluation of validation success showed that the tip position was “optimal” in 79 cases (71.8%) and “suboptimal” in 26 cases (23.6%) in the clinical setting. There were no venous thromboses or catheter occlusions during the catheter placements.
Conclusion
This Formula could be acceptable in performing the bedside PICC placement in the real clinical settings.
Keywords
Introduction
Peripherally inserted central venous catheter (PICC) is widely used for venous access for nutritional supports, the stable deliveries of vasoactive and chemotherapeutic drugs. Compared to the centrally inserted venous catheter via the internal jugular or subclavian vein, the PICC shows the lower risk of procedure-related major complications. 1 However, this technique remains an issue having the relatively higher risk of catheter occlusion 2 or thrombotic complications, 3 often derived from the catheter tip malposition. Although the placement with fluoroscopic guidance is more reliable for placing the catheter tip precisely,4,5 the bedside PICC placement should be often inevitable in the real clinical situations such that the patients have a hemodynamic instability or some kind of infection such as COVID-19.
Empirically, the anthropometric measurement techniques have been widely applied at bedside PICC placement. 6 The magnetic tracking and/or electrocardiograph-guided tip location technique7–9 have been proposed for intending more accurate catheter tip positioning at bedside insertion. However, these modalities have not yet been prevalent in Japan due to their intricacies and the costs. Then, simpler and lower cost methods have been expected to be reported in the clinical fields. Ramamurthi et al. first showed the measurement technique using pre-procedural chest X rays (pre-CXR) in children. 10 Especially, recent studies from South Korea have demonstrated the formulas statistically induced by measuring the landmarks on pre-CXR.11–13 Apart from these formulas, we examined the formula based on the calculation for predicting the catheter length in the thorax by using the pre-CXR combined with the direct measurement of arm length. On this prospective study, the feasibility of this formula was estimated in the clinical bedside PICC placement.
Materials and methods
Patients
From April 2021 to June 2025, a total of 121 patients had experienced the upper arm PICC placement at the bedside based on the Formula mentioned below after acquiring the ethical approval from the Hospital Review Board (No.2021-2). Since November 2022, the traditional anthropometrical measurements also had been continuously performed for comparison with the Formula. All the patients approved the significance of this procedure with the written informed consent. The information of the patients was collected through the electronic medical records and all measurements were made using the software available with the PACS system. The collected data were patient’s disease, age, sex, height, weight, body mass index (BMI), the PICC insertion side (right or left), the selected veins, and the clinical course. Ethical approval for this study was obtained from ethics committee of the Saiseikai Ibaraki Hospital (No. 2025-10).
Exclusion criteria
Eleven cases that the CXR for confirming the catheter placement after PICC procedure performed in the upright positions were excluded, because the PICC tip position was reported to move at a higher location than the supine position at the range from 2 to 3 cm, 14 so that the other 110 cases that post-procedural CXRs (post-CXR) performed in the supine positions were included in this study for standardizing the procedures. Among the 110 cases, three cases could not be applied to the calculation of the Formula, because these catheter tip positions were too far from the carina to measure the catheter distance: being the ipsilateral internal jugular vein in one case and the ipsilateral brachiocephalic veins in the other two cases. These three cases were regarded as the case of “malposition.”
PICC placement procedure
All PICC catheters were placed at bedside while the patients were in supine position with the abducted arms to 90 degrees under US guidance. Principally, the selected arm was preferred to be the opposite side of dominant hand, and the basilic vein was decided the first choice for minimizing the risk of injuring the median nerve or the brachial artery. The venipuncture site selection was based on a vein diameter, depth or a straight shape. A skin puncture site was designated and marked. The distance from the axilla to the puncture site was measured and recorded, to which the pre-calculated catheter length in the thorax (from axilla to carina) was added, meaning the “Formula” predicting catheter length from the puncture site to the carina in this study. The predicted ideal catheter lengths were determined by the additional 2 cm to the length of Formula and the actual catheter lengths inserted in this study were the same as these lengths. The Groshong PICC catheter used was 4 Fr. in diameter and silicone single lumen (CR Bard, Salt Lake City, UT, USA). During the insertion of catheter, the patient’s head was rotated toward the insertion side and tilted the chin to the chest to minimize the tip malposition into the internal jugular vein. After the PICC placements, all the catheter tip positions were confirmed by the post-procedural CXR (post-CXR) in supine position with the arm adducted back to the trunk.
Determination of the true catheter length from the puncture site to the carina
The true catheter length from the puncture site to the carina was adjusted from the actual catheter length on the post-CXR by subtracting or adding the distance of the actual tip position from the carina.
The predictive formula using the pre-procedural chest radiograph (pre-CXR)
The predicted PICC length from the axilla to the carina in the thorax was calculated by using the three landmarks (the axilla, the middle of SVC and the clavicle convex) on the pre-CXR (Fig. 1). The middle of SVC at the horizontal level of the carina was pointed as Ⓐ. The point of axilla presented as Ⓑ was determined 1 cm outer from the chest wall along the straight line from the point Ⓐ to the middle of the lateral line of the scapula. The width of “1 cm” was estimated as the average width of subcutaneous tissue around the axilla. The clavicle convex shown as Ⓓ was the point of the middle of the inferior crossing line between the clavicle and the first rib. The crossing point between the Ⓐ-Ⓑ line and the vertical straight line from the clavicle convex (Ⓓ) toward the Ⓐ-Ⓑ line was shown as the point Ⓒ. The half of the circumference of the ellipse formed by the two lines (Ⓐ-Ⓑ: major axis and Ⓔ-Ⓕ: minor axis; the line slid from Ⓒ-Ⓓ line onto the middle of Ⓐ-Ⓑ line) seems to trace the PICC catheter well. The estimated length of the half ellipse was mathematically calculated by the expression in the following: The half ellipse formed by the radiologic parameters on the chest radiographs in both sides. Ⓐ: A midpoint in the SVC on the carina line. Ⓑ: A point of 1 cm from the thoracic wall along the line from the point of Ⓐ to the middle of the lateral line of the scapula. Ⓒ: A crossing point of the vertical line from Ⓓ toward Ⓐ-Ⓑ line. Ⓓ: Middle of the inferior crossing line between clavicle and 1st rib. Ⓐ-Ⓑ line: Major axis. Ⓒ-Ⓓ line: Minor axis. Ⓔ-Ⓕ line: A line shifted Ⓒ-Ⓓ line on the middle of Ⓐ-Ⓑ line. Green dot line: Half ellipse formed by major axis (Ⓐ-Ⓑ line) and shifted minor axis (Ⓔ-Ⓕ line) seeming to trace the thoracic PICC line.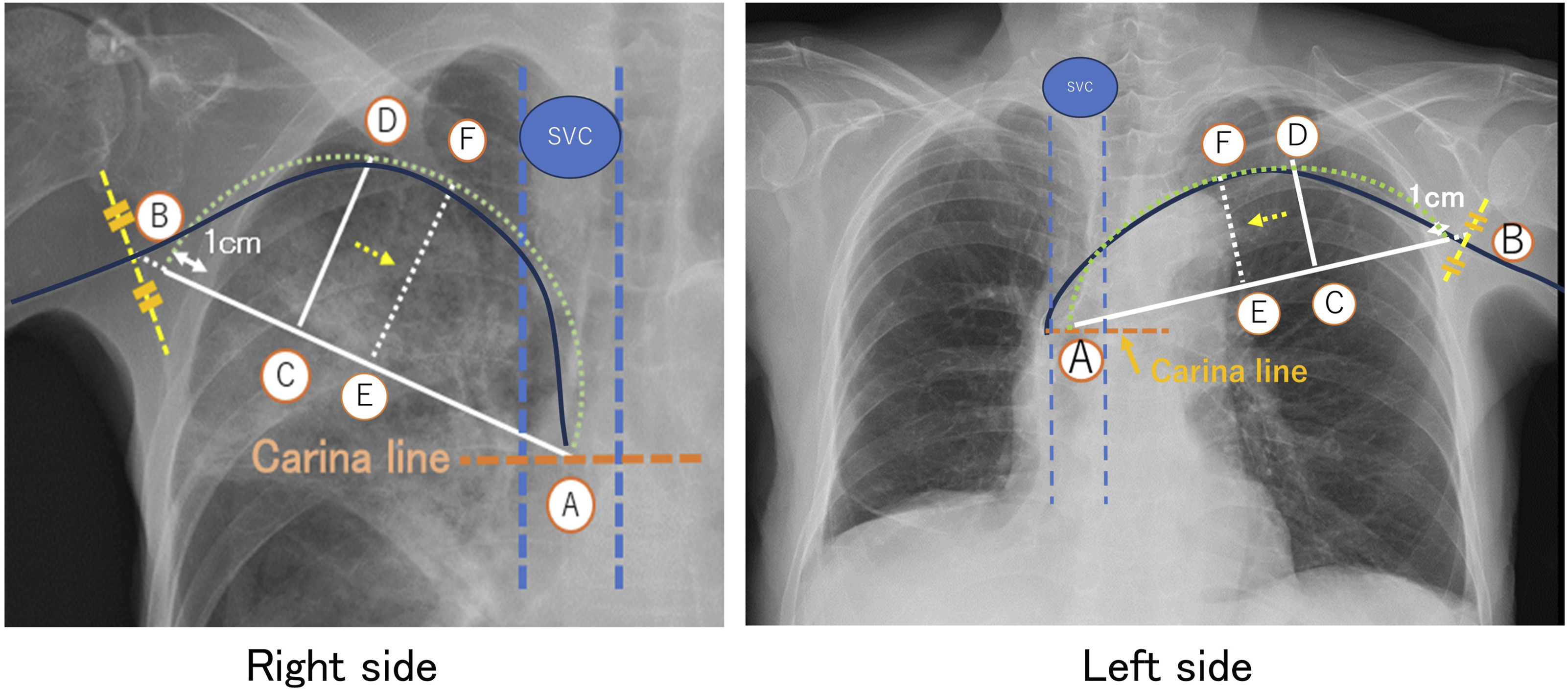
The length from the axilla to the puncture site was directly measured as shown in Fig. 2. Then, the predictive Formula of the length from the puncture site to the carina was the length of the half ellipse plus direct measurement from the axilla to the puncture site (Figs. 1 and 2). The direct measurement of the distance from the axilla to the puncture site. ➀: Before performing PICC placement, a length of half ellipse was calculated in advance by using the parameters on pre-CXR as the thoracic PICC length. ➁: A planned puncture site was decided by US and marked, the length from axilla to the puncture site was practically measured. The predicted PICC length from the carina level to the puncture site was extrapolated a length of half ellipse plus an actually measured length from axilla to puncture site.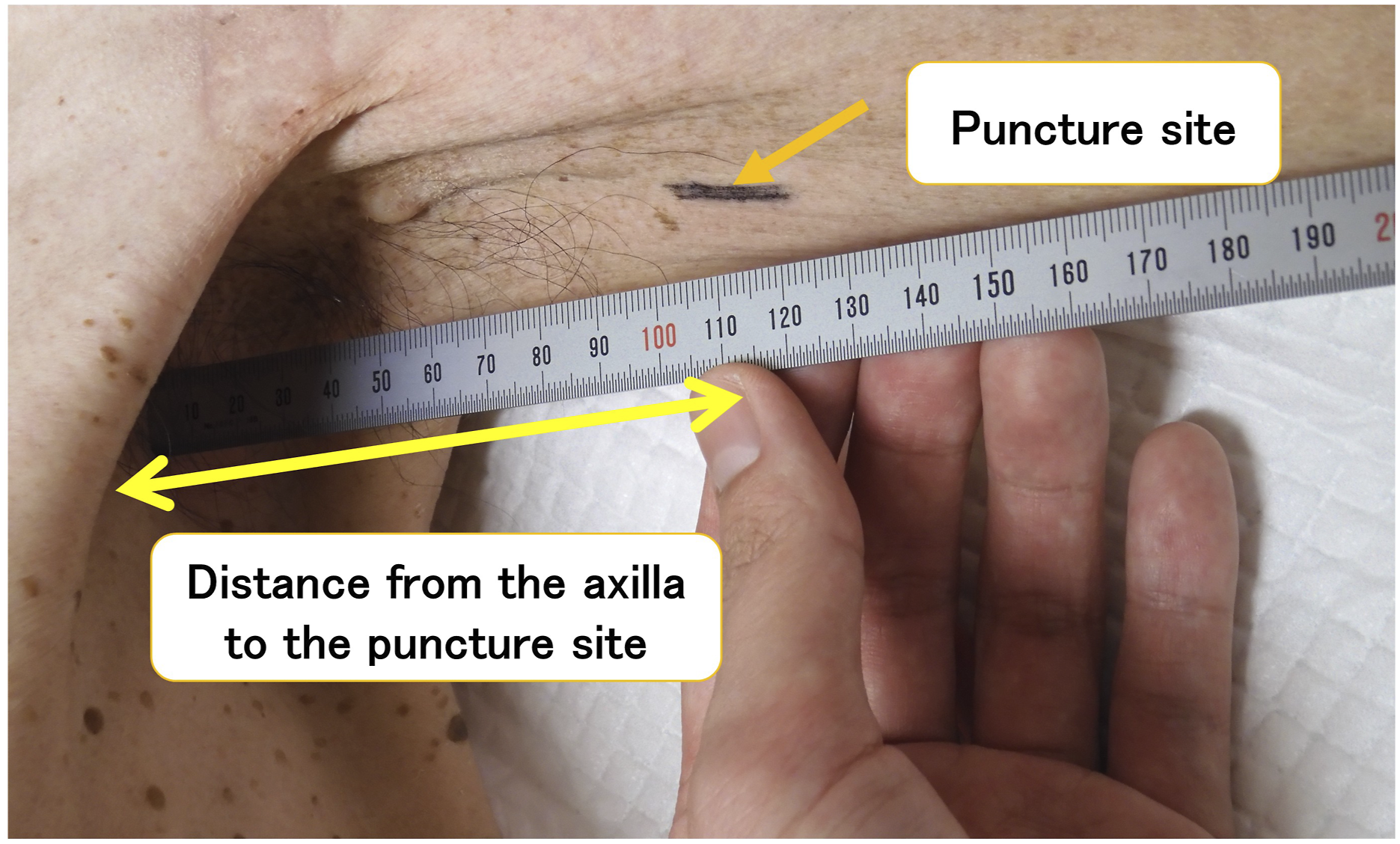
The traditional anthropometrical measurement (TAM)
The traditional anthropometrics from the puncture site to the fourth intercostal space via the central portion of the right clavicle head, were performed in the 48 patients as the other predictive method for the PICC catheter length from the puncture site to the carina (Fig. 3). Traditional anthropometrical measurement (TAM). TAM means the direct measurement from the puncture site to the fourth intercostal space via the central portion of the right clavicle head.
The classification of tip position
The catheter tip positions were classified into the three groups: optimal, suboptimal, and malposition. In the optimal position, the tip of the catheter was determined to locate between the middle of the SVC and the upper portion of the right atrium (RA), within 7 cm below the carina.15–18 In the suboptimal position, it was estimated to locate in the other area from the upper line of the SVC to the mid-RA, in the rage of 3 cm above the carina, or in the rage of 7 to 9 cm below the carina.15–18 The other positions were regarded as malposition. The ideal predicted PICC length that was actually inserted in this clinical study, was designated the result of the Formula plus 2 cm.
Statistical analysis
All statistical analyses were performed using EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan), which is a graphical user interface for R (The R Foundation for Statistical Computing, Viena, Austria). Statistical significance was set at P values <0.05. Normal distribution was assessed using visual histograms and analytical methods (Kolmogorov-Smirnov test). Differences between 2 independent quantitative variables were determined by the Student’s t test, or the Welch test was used when variances were unequal. For more than 2 groups, ANOVA (Analysis of Variance) was employed. For correlation analysis of continuous variables, Pearson’s correlation coefficient was used, Continuous variables were summarized using mean ± standard deviation (SD). Categorical variables are described as percentages (%).
Results
Patient characteristics
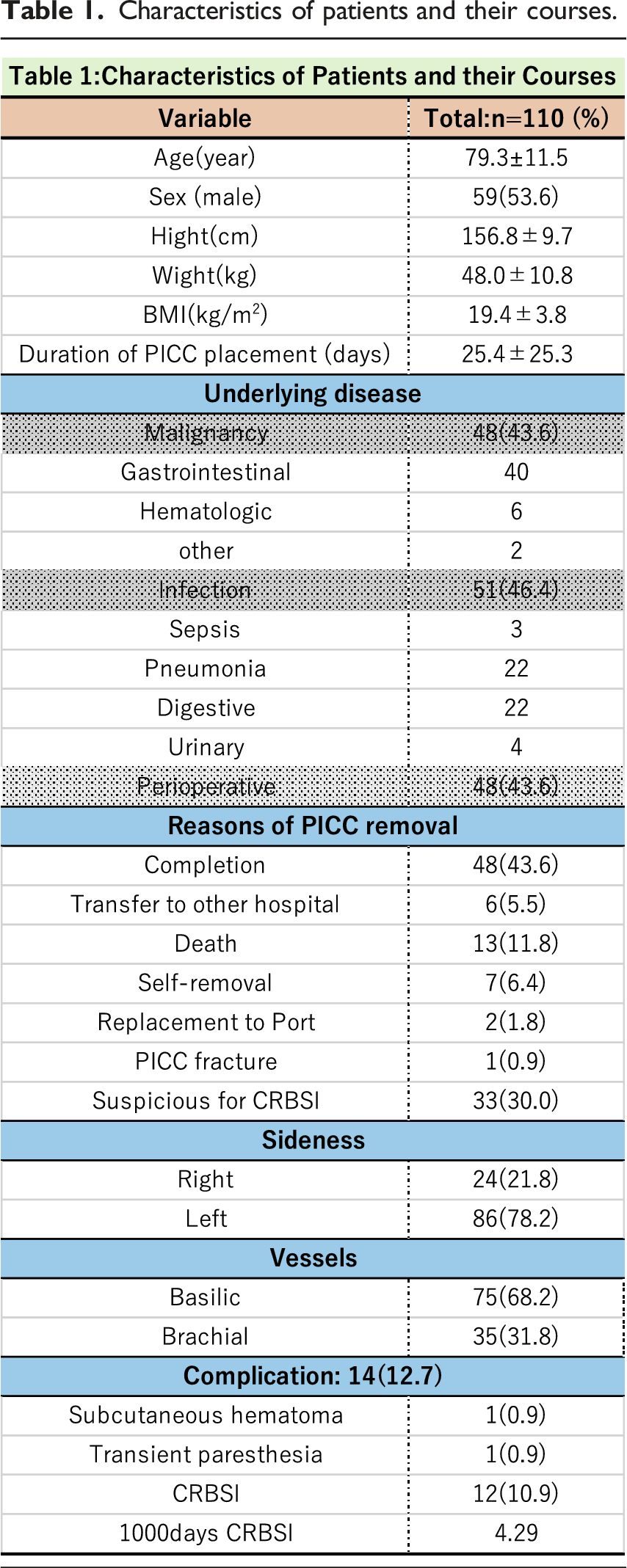
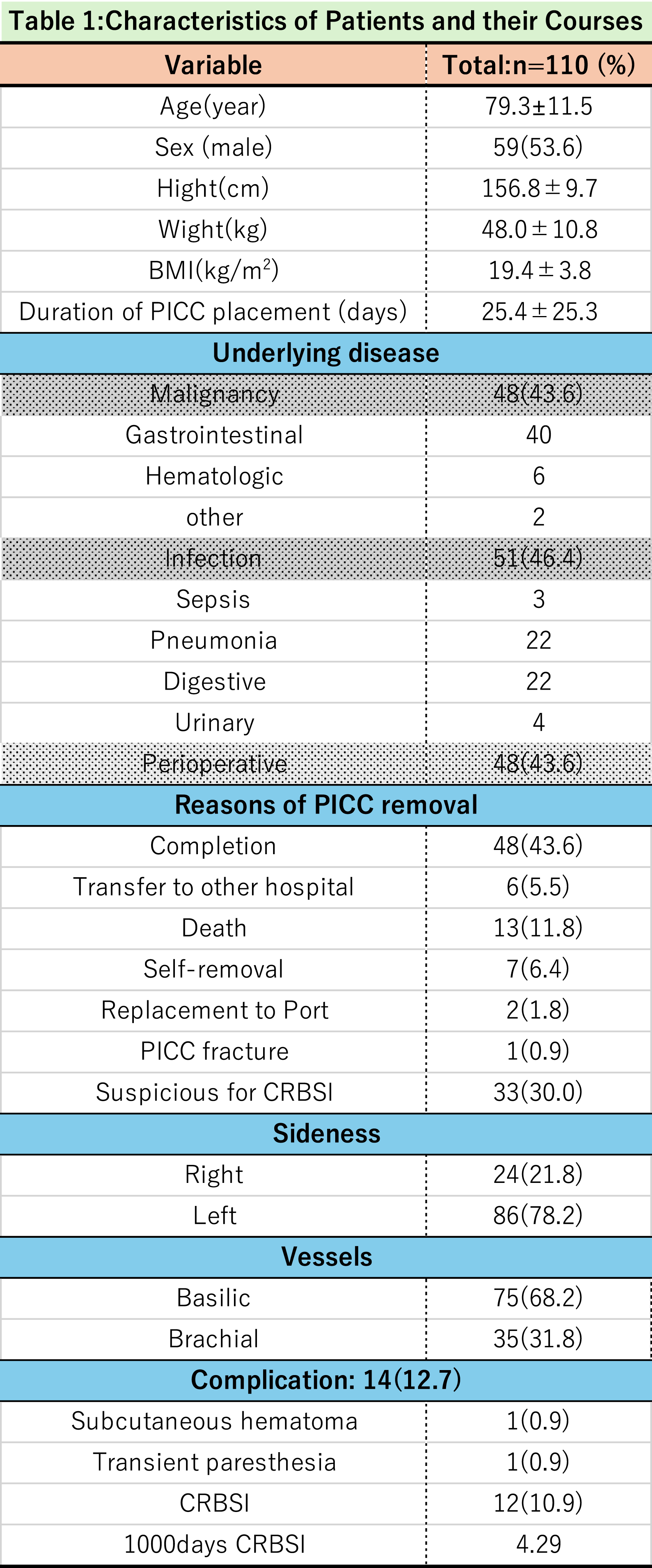
Characteristics of patients and their courses.
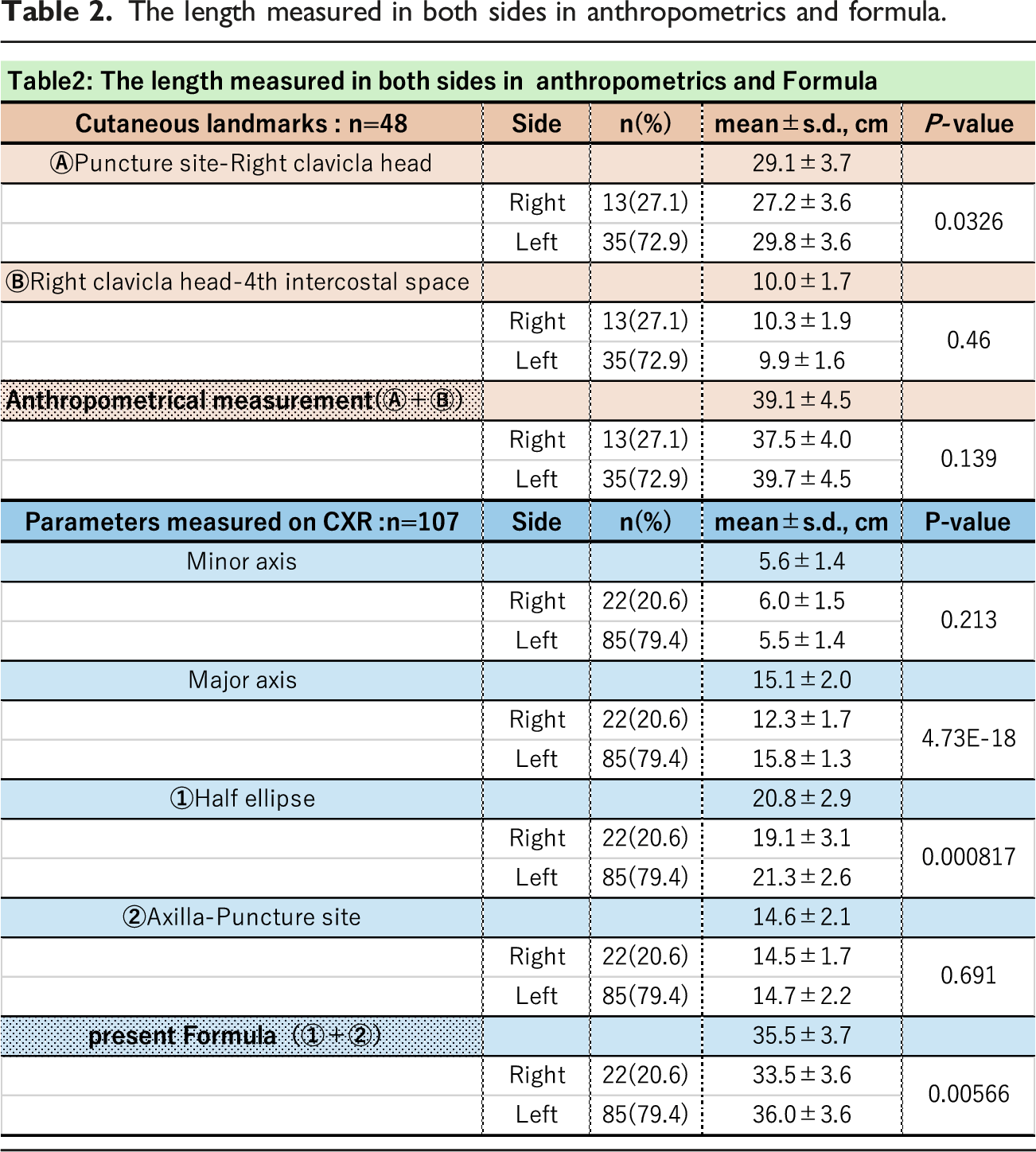
The discrepancies of the lengths measured in both sides between the two predictive measurements
The length measured in both sides in anthropometrics and formula.

Correlation coefficient between the true PICC lengths and the main-effect valuables.


The comparison of the difference of the catheter distance from the carina between the two predictive methods
Fig. 4 shows the box plots of the differences of the PICC catheter distance from the carina between the two predictive methods. The Formula plus 2 cm means the actually inserted PICC catheter length based on the ideal PICC length induced by the Formula plus 2 cm. On the other hand, the PICC lengths of the TAM were the only theoretical results and not applied in the clinical setting. The mean distance from the carina according to the Formula plus 2 cm was 2.3 cm which was almost the same as the ideal PICC length (the PICC length of the Formula is the level of the carina and plus 2 cm) The differences were smaller in the Formula than in the TAM (P = .00053). Additionally, the variances of the values were not equal between them, meaning that the variance in the Formula was smaller than in the TAM (P = .038). Box plots representing the PICC catheter distance from the carina between the two predictive methods. The variances of the tip positions ended up being smaller in the Formula plus 2 cm than the TAM (P = .038). Additionally, the tip positions could be more gathered around the ideal position, 2 cm below the carina in the Formula plus 2 cm (P = .00053)
The actual PICC length prediction by the formula plus 2 cm in the clinical setting
The results of the bedside PICC catheter placements with this Formula plus 2 cm in the 110 patients were in the followings: the tip positions regarded as “optimal” were in 79 cases (71.8%), “suboptimal” in 26 cases (23.6%) and the other 5 cases (4.5%) were classified as “malposition.” Consequently, the catheter tips were acceptably located from the superior margin of the SVC to the middle of the right atrium (RA) in the 105 cases (95.5%) (Fig. 5). The real PICC catheter positions from carina in 110 cases performed with this Formula plus 2 cm. The dot plots showed the results of the PICC catheter positions in the clinical settings. The tip positions regarded as “optimal” were in 79 cases (71.8%). Twenty-six cases (23.6%) were evaluated as “suboptimal” and the other 5 cases (4.5%) were classified as “malposition.” In the 105 cases (95.5%), the catheter tips were acceptably located from the superior margin of the SVC to the middle of the right atrium (RA).
Discussion
There is ongoing controversy regarding the optimal location of the central venous catheter tips. 19 European guidelines indicate the tip of the catheter should be located between the lower middle of the SVC and the upper third of the RA. 15 The KDOQI guidelines recommended that the proper catheter tip was at mid-RA. 16 The Infusion Nurses Society advocated that central catheters should be in the SVC. 17 Based on these statements, in the present study, the “optimal” catheter tip position was decided the range from the middle of the SVC to the upper portion of RA. The “suboptimal” position was broadly set from the upper portion of the SVC to the mid-RA. The range of these areas was arbitrarily set according to Venkatesan T. et al. 18 In our study, the level of around 2 cm below the carina was established to be an ideal tip position in performing the bedside PICC insertion, and the acceptable placements within the range of the optimal and the suboptimal area were achieved in 105 patients (95.5%) (Fig. 5).
This study selected the simple two straight lines for estimating the PICC catheter length in the thorax. The present Formula is based on the concept that the half ellipse formed by the two lines well traces the actual PICC catheter line in the thorax. This Formula is, namely, composed by the two measurement methods with the calculation part in the thorax and with the direct measurement part in the arm (from the axilla to the puncture site). Although the mathematical expression for the half ellipse seems to be complex, it will easily applied to the clinical settings if it is once inputted into the computer systems. As compared with the predictive PICC length by the TAM based only on the direct measurement with anatomical landmarks, it was clearly shown that the values predicted by the Formula showed more precise (Fig. 4) and higher relationship with the true PICC length (Table 3). The inferiority of TAM seemed to be derived from the measurement errors. As shown in Table 3, the distance from the right clavicle head to the 4th intercostal space indicated no significant correlation with the true PICC length, meaning the dispersion of measuring the area was wide. To minimize the measurement errors, an objective method such as using pre-CXR is generally preferred.
Recent report by Lee et al. 13 indicated the validation of the prediction formula based on pre-CXR, showing the rate of optimal tip position was 90.1%. The updated formula was consisted of many kinds of parameters statistically selected on the pre-CXR: humero-vertebral distance, thoraco-carinal distance, second ribs horizontal distance, distance of two vertebral body units, and contralateral clavicle length. Apart from the statistically induced formula, our Formula was based on the concept of directly tracing the PICC catheter, so that being easy to be perceived and applicable to the clinical settings.
However, this study had several limitations. First, this study was achieved by a single institution and the sample size was small. Second, the lengths of the major or minor axis on pre-CXR could be changed according to the patient’s positions. For example, in the case of patient with stooped posture, the minor axis would tend to be shorter. Additionally, the PICC tip was reported to tend to move in a caudal direction more than 2 cm with changing the arm position from 90 degrees abduction to adduction. 20 So, the tip position checked at the post-CXR should be recognized as the result after the patients’ arm had already moved. Third, the signation of the landmarks in the axilla (the point Ⓑ on the pre-CXR in Figs. 1 and 2) might have better to be modified, because the point would be supposed to change according to the patient’s chest subcutaneous width.
In conclusion, this study suggested that the formula could help predict the reliable tip position within the central vein. This method is expected to benefit the patients that have the restriction of the intra-hospital transportation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This prospective study was approved by the hospital review broad (No.1018). All the patients approved this procedure with the written informed consent.