
Abstract
Background
The role of radiology in patients with clinical suspicion of COVID-19 is evolving with scientific evidence, but there are differences in opinion on when and how the technique should be used for clinical diagnosis.
Purpose
To estimate the pre-test and post-test probability that a patient has COVID-19 in the event of a positive and/or negative result from chest X-ray and chest computed tomography (CT) radiological studies, comparing with those of real time polymerase chain reaction (RT-PCR) tests.
Methods
The literature on the sensitivity and specificity of the chest X-ray, chest CT, and RT-PCR was reviewed. Based on these reported data, the likelihood ratios (LR) were estimated and the pre-test probabilities were related to the post-test probabilities after positive or negative results.
Results
The chest X-ray has only a confirmatory value in cases of high suspicion. Chest CT analyses showed that when it is used as a general study, it has almost confirmatory value under high clinical suspicion. A chest CT classified with CO-RADS ≥ 4 has almost a diagnostic certainty of COVID-19 even with moderate or low clinical presumptions, and the CO-RADS 5 classification is almost pathognomonic before any clinical presumption. To rule out COVID-19 completely is only possible in very low clinical assumptions with negative RT-PCR and/or CT.
Conclusions
Chest X-ray and especially CT are fast studies that have the capacity to report high probability of COVID-19, being a real contribution to the concept of “probable case” and allowing support to be installed in an early and timely manner.
Introduction
The world has experimented the most important health challenge in recent times since December 2019, with the COVID-19 pandemic that has already affected more than 600 million people and produced more than 6 million deaths. 1 From the experience of countries with large-scale community transmission, it has been learned that COVID-19 requires an unprecedented mobilization of health systems.2–5 The demand on health care systems has been stressed, especially intensive care units for large numbers of people who become ill simultaneously. The ability of the health care system to respond will depend on available resources, including hospital beds and intensive care units. It also requires personnel trained in the rapid and timely diagnosis and treatment of COVID-19, where imaging plays a fundamental role.
In the daily experience of radiology, we are faced with the diagnosis of SARS CoV-2 pneumonia with plain radiographs (chest X-ray) or computed tomography (chest CT). Although the Gold Standard for the diagnosis of COVID-19 is the real time polymerase chain reaction (RT-PCR), this may be unknown at the time of image analysis. 6 The sensitivity of RT-PCR is not very high either, 42–83%, 7 which makes many patients with a negative result (PCR (−)) for COVID-19 consult. The role of chest CT in patients with clinical suspicion of COVID-19 is evolving with scientific evidence, but there are substantial differences in opinion on when and how the technique should be used for clinical diagnosis. 3 While the American College of Radiology only recommends the use of CT to solve problems, the Fleishner society assigns it a role as an important tool to use if symptoms worsen or in a resource-limited setting for RT-PCR.8,9
The Expert Consensus Statement on Reporting of the Radiological Society of North America (RSNA) 10 has proposed a standardized classification for CT: (a) typical appearance (Cov19Typ): characterized by peripheral, bilateral, ground glass opacities (GGO) with or without consolidation or intralobular lines (crazy paving), multifocal GGO and/or findings of organizing pneumonia; (b) indeterminate appearance (Cov19Ind): characterized by absence of typical pattern but with multifocal, diffuse, perihilar, unilateral or few very small GGO; (c) atypical appearance (Cov19Aty) characterized by signs of other pneumonias; and (d) negative for pneumonia (Cov19Neg). The British Society of Thoracic Imaging (BSTI) has also proposed a classification for Rx that includes the categories: (a) classic/probable, with peripheral GGO, (b) indeterminate due to central/basal consolidation or poor quality film, (c) non-pneumonic findings, and (d) normal. 11 The Dutch Radiological Society developed a standardized assessment scheme for pulmonary involvement of COVID-19 in CT that would make it possible to compare data across populations. The authors chose the term CO-RADS, the COVID-19 Reporting and Data System. These authors analyzed 105 randomly selected Chest-CT obtained in a group of consecutive patients who presented to an emergency department, all with RT-PCR results. CT images were extracted from the picture archive and communication system, anonymized and analyzed by eight observers, who assigned CO-RADS scores without clinical or PCR information. They established a very rigorous classification of the levels of suspicion of pulmonary involvement of COVID-19, with the following categories: 0, not interpretable; 1, very low; 2, low; 3, equivocal/unsure; 4, high; 5, very high; and 6, proven by RT-PCR. Each of these categories was defined very precisely, and they related each category to the proportion of cases with RT-PCR positive, which makes this system ideal for use in quantitative/comparative studies. 8
In clinical practice, including radiology, the diagnostic process follows a Bayesian inference structure, increasing the probability of a test-based diagnosis (i.e., chest X-ray, chest CT, RT-PCR, etc.) and clinical presumptions (pre-test probabilities), which in turn are based on signs and symptoms reported by the patient or observed by the doctor.12–14 The classical form of the Bayes’s theorem can be presented as follows. If we have a set of events {B
i
} (set of possible diagnosis), mutually exclusive, and an event A (a medical image), we can obtain the probability of B
i
given A from the following expression

Being P (
Although this procedure does not involve those calculations when a diagnosis is proposed in clinical practice, the method is based on estimates of sensitivity, specificity and likelihood ratios that allow a quantitative approximation of the usefulness of the tests.12,14 It is important to note that the clinical presumption is influenced by the epidemiological context of the patient who consults. 14
Based on current knowledge, when we report a chest CT or a chest X-ray we ask ourselves how likely it is that the patient has COVID-19 when we report a positive result, and conversely, how likely it is that they do not have COVID-19 when we report negative test results. The aim of this paper is using Bayesian approach, to relate the clinical presumptions (pre-test probabilities) to the post-test probabilities of having COVID-19 with different X-ray and CT results, comparing with those of RT-PCR.
Material and methods

Studies included in our analyses, excluding systematic reviews and meta-analyses.

For different values of clinical presumption of having COVID-19 (pre-test probabilities, p0), the a priori odds were calculated by
Results
Sensitivity (S), Specificity (Sp), positive and negative likelihood ratios (LR (+) and LR (−), respectively) for RT-PCR, chest Rx and chest computed tomography, without using (General) and using the CO-RADS system.
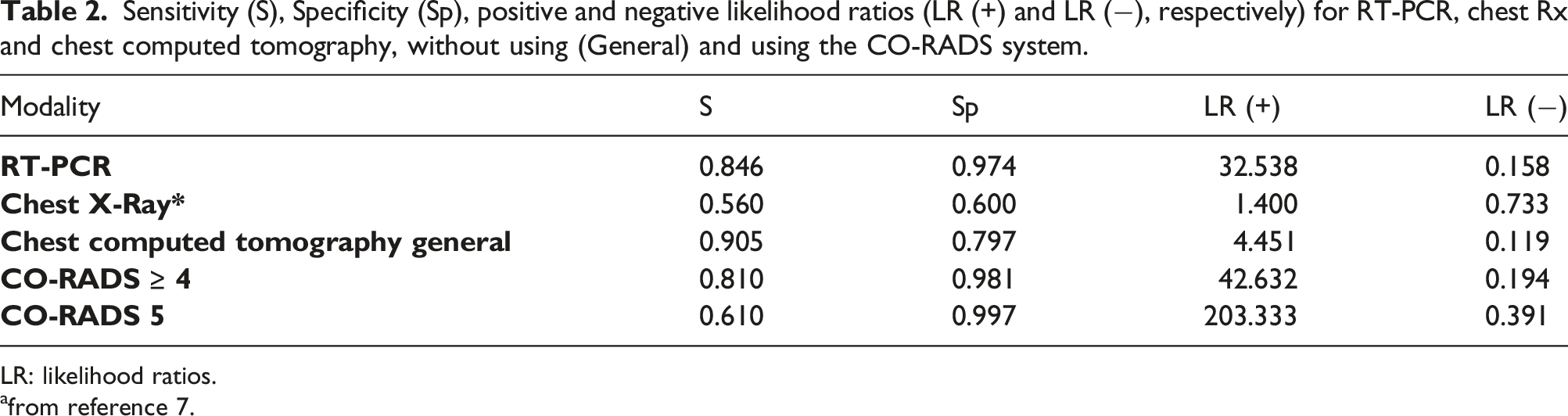
LR: likelihood ratios.
afrom reference 7.
A positive result of CT with high clinical presumption of COVID-19 (p0 ≥ 0.8) had confirmatory value (p (+)> 0.95); the Gold Standard RT-PCR would have confirmatory value even with low clinical presumptions (p0 ≥ 0.37) (Figure 1(a)). Categorizing a CT with CO-RADS ≥ 4 confirms the diagnosis of COVID-19 (p (+) > 0.95) with clinical presumption p0 ≥ 0.31 similar to RT-PCR. Interestingly, the typical image for COVID-19 pneumonia (CO-RADS 5) would have confirmatory value for any level of clinical presumption (Figure 1(b)). Variation of post-test probabilities of chest X-ray, chest computed tomography and RT PCR (as reference), for several pre-test probabilities to have COVID-19 when the result is positive (a), for CO-RADS ≥ 4 and CO-RADS 5 categories (b), and for a negative result (c). Horizontal green and black lines represent post-test probabilities 0.95 and 0.05, respectively.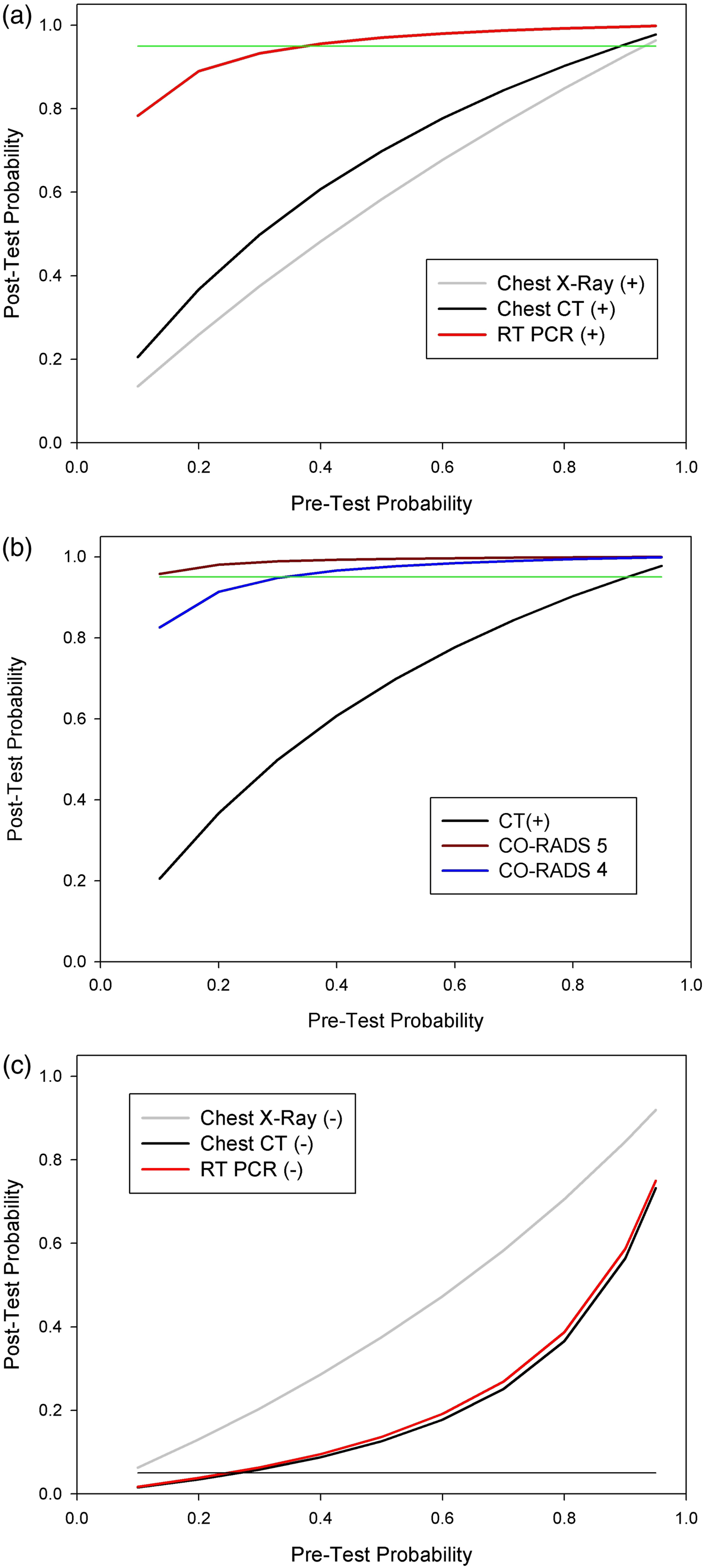
In the event of a negative result, chest X-ray does not allow ruling out COVID-19 (i.e., when p (−) <0.05) in any case, and RT-PCR and CT can only do so with very low clinical assumptions, p0 ≥ 0.24 and 0.33, respectively (Figure 1(c)).
Discussion
All the literature reviewed reported moderate to high sensitivity and high specificity of RT-PCR,7,8–11,21–25 which leads to values of LR (+) = 40.0, implying that a positive result increases by 40 times the odds of having COVID-19, so this test has a Gold Standard value. The chest X-ray, on the other hand, has poor S and Sp,15,26 so it has only a confirmatory value in cases of high suspicion of COVID-19. Although the values presented here for chest X-ray come from a single study, this has a sample size (n = 1198), one order of magnitude larger than the other analyzed studies and also the estimations of S are similar to those studies. For example, S = 0.44, 17 S = 0.591, 18 S = 0.59, 20 S = 0.25, 19 and S = 0.67. 16 Some of these studies reported high Sp, but values of Sp = 1 17 and Sp = 0.9 19 may be a consequence of low sample sizes (n = 40–50). A chest X-ray can be useful as a confirmatory test when the clinical symptomatology is very clear and RT-PCR or chest CT are not available. 15 It must also be considered that many hospitals in the world are employing chest X-ray as the first-line method, with faster results than with RT-PCR and chest-CT, especially using portable X-ray units. This test reduces the movement of patients and minimizes the risk of cross-infection considering that these patients need to be isolated. 16
This analysis shows interesting aspects with respect to the chest-CT. When CT is used as a general study without using the CO-RADS classification, it has almost confirmatory value (p (+)> 0.95) only when the clinical presumption is high (i.e., p0 > 0.8). Consistent with other reports, these results suggest that CT is a real contribution to screening for COVID-19 in patients with clinical and epidemiologic features compatible with COVID-19 infection, particularly in patients without RT-PCR or when results of RT-PCR tests are negative, and thus rapidly initiate treatment.7,16 The use of CO-RADS classification allows systematizing the diagnosis of COVID-19, agreeing with other studies.
8
The sensitivity of the CO-RADS classification test decreases for high CO-RADS categories but its specificity increases, being very high for COVID-19 when an image is classified as CO-RADS 5. A chest CT classified with CO-RADS ≥ 4 allows almost certain diagnosis of COVID-19 even with moderate or low clinical presumptions (p0 ≥ 0.3) and the CO-RADS 5 category is almost pathognomonic before any clinical presumption (Figure 2). None of the analyzed studies (RT-PCR, chest X-ray and chest-CT) can be used to rule out COVID-19 completely, this being possible only at very low clinical assumptions with negative RT-PCR and/or CT. Images that can be found in a typical appearance of SARS CoV 2 pneumonia CO-RADS 5. (a) Chest X-ray with multiple peripheral patchy opacities in both lungs; (b) Chest computed tomography showing ground glass opacities mixed with areas of crazy paving; (c) Atoll sign probably indicating organized pneumonia with higher peripheral density and lower central density; (d) peripheral ground glass opacities and atoll sign probably indicating organizing pneumonia; (e) Extensive involvement of both lungs, with predominantly peripheral ground glass parenchymal opacities; (f) bulls-eye sign probably indicating organizing pneumonia; (g and h) Reticular areas of peripheral sub-cortical fibrosis.
This study has some limitations. It is based mainly on average estimates based on previous studies that allowed estimating likelihood ratios and probabilities a posteriori, therefore being dependent on the type and size of the samples of these previous studies. It does not consider intra- or inter-observer variability when analyzing radiological images or the intrinsic variability of the sensitivity and specificity estimates. However, it has the virtue of showing quickly and easily the relevance and contribution that radiological exams are making in clinical practice to the diagnostic support of COVID-19.
In conclusion, Chest X-ray and CT are very fast studies and have the capacity to report high probability of COVID-19, being a real contribution to the concept of “probable case” and allowing support to be installed in an early and timely manner.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Agency of Investigation and Development (ANID) of Chile [ANID COVID 0960 grant].
Ethical approval
Our study is based on published secondary data; therefore it did not require approval from the ethics committee of the Faculty of Medicine.