
Abstract
Background
The increasing ratio of functional future liver remnant (functional %FLR) after modified associating liver partition and portal vein ligation/embolization for staged hepatectomy (modified-ALPPS) compared with portal vein embolization (PVE) has not been comprehensively evaluated.
Purpose
To compare the increasing ratio of functional %FLR between modified-ALPPS and PVE via technetium-99 m-galactosyl human serum albumin single-photon emission computed tomography (99mTc-GSA SPECT/CT) fusion imaging.
Material and Methods
Seven and six patients underwent modified-ALPPS (modified-ALPPS group) and PVE (PVE group) from 2015 to 2019. The functional %FLR on 99 mTc-GSA SPECT/CT fusion imaging was assessed before and 1 week (modified-ALPPS group) and 3 weeks (PVE group) after each procedure. The increasing ratio of functional %FLR (functional %FLR ratio) was calculated and compared between the two groups. Moreover, the hypertrophy ratio of future liver remnant volume (FLRV ratio) and atrophy ratio of embolized liver volume (.ELV ratio) were evaluated.
Results
The mean functional %FLR ratios of the modified-ALPPS group (1.47 ± 0.15) and the PVE group (1.49 ± 0.20) were comparable (p > .05). The median FLRV ratio of modified-ALPPS group (1.48) was higher than that of the PVE group (1.16), the median ELV ratio of the PVE group (0.81) was lower than that of the modified-ALPPS group (0.94), and the results significantly differed between the two groups (p < .05).
Conclusion
The increasing ratio of functional %FLR was comparable between modified-ALPPS and PVE. Compared with PVE, ALPPS was associated with a higher hypertrophy rate of the remnant liver but a lower atrophy rate of the embolized liver.
Keywords
Introduction
Portal vein embolization (PVE) and two-stage hepatectomy can be performed to induce compensatory hypertrophy of the remnant liver, thereby increasing the safety of major hepatectomy.1,2 If the residual liver parenchyma is normal, a future liver remnant volume (FLRV)-to-total liver volume ratio of at least 20% is required to prevent post-hepatectomy liver failure (PHLF). Moreover, the volumetric future liver remnant (%FLR) should be at least 30% in patients with chemotherapy-induced hepatic injury. However, a volumetric %FLR of at least 40% is recommended for patients with cirrhosis.3,4 Functional future liver remnant (functional %FLR) after hepatectomy can be assessed via technetium-99 m-galactosyl human serum albumin single-photon emission computed tomography (99 mTc-GSA SPECT/CT) fusion imaging, which is useful for identifying hepatectomy candidates.5–8 Several studies have shown that functional %FLR is more efficient in assessing future remnant liver function than volumetric %FLR.9–12
A recent study described the use of associating liver partition and portal vein ligation/embolization for staged hepatectomy (ALPPS), which is a novel two-stage technique for hepatic resection. 13 ALPPS can help increase the initial FLRV by 60%–80% within 7–10 days. 14 However, a high liver volume is not associated with an elevated liver function.15,16 Therefore, the increasing ratio of functional %FLR after ALPPS compared with PVE has not been comprehensively evaluated.
This retrospective clinical study was performed to compare the increasing ratio of functional %FLR between the modified-ALPPS and PVE for major hepatectomy via 99 mTc-GSA SPECT/CT fusion imaging.
Materials and methods
Patients
Indications for modified-ALPPS and PVE.

Abbreviations: Modified-ALPPS, modified associating liver partition and portal vein ligation/embolization; PVE, portal vein embolization; volumetric %FLR (%), ration of the future liver remnant volume to the total liver volume; ICGK-F, a future liver remnant plasma indocyanine green clearance rate.
Modified-ALPPS and PVE groups.
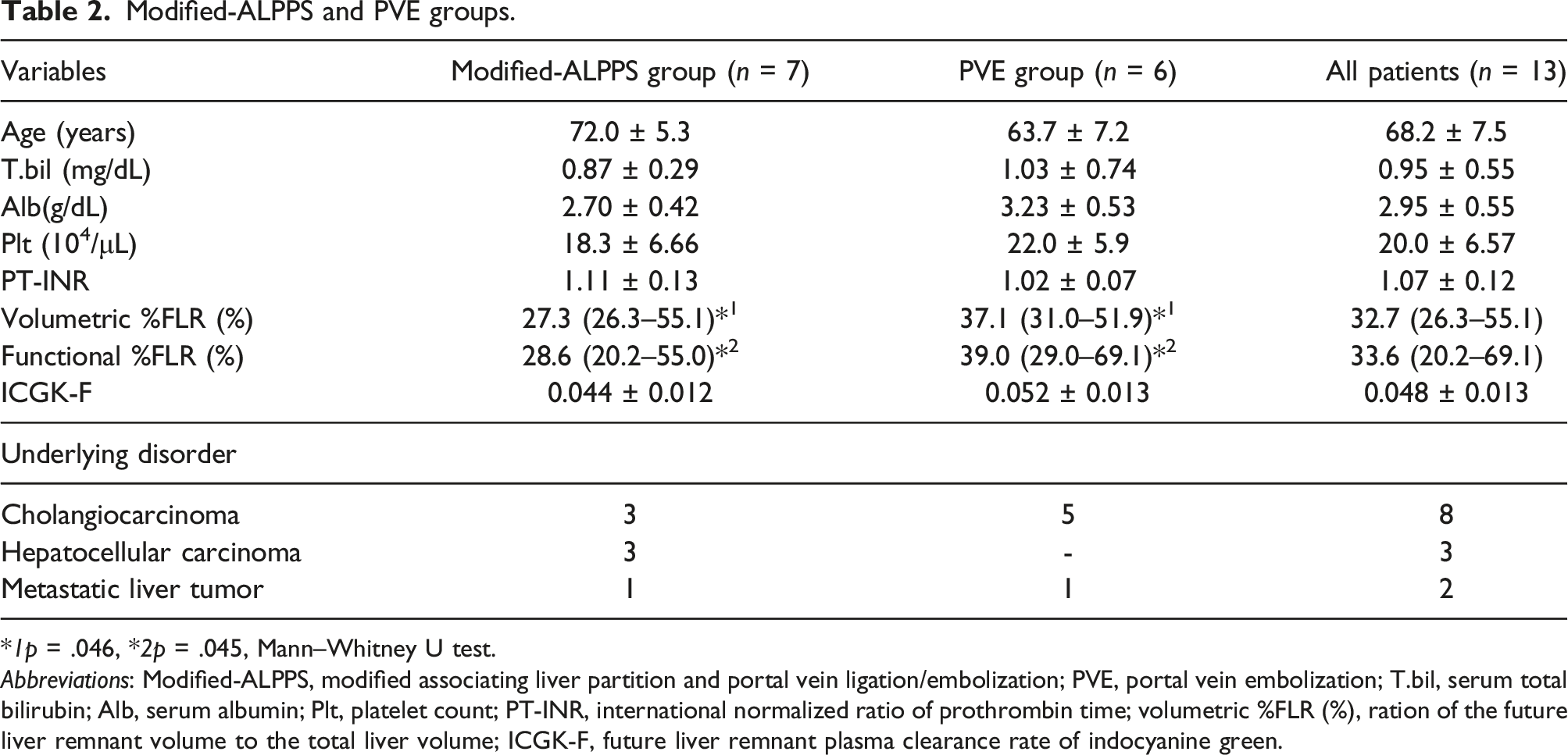
*1p = .046, *2p = .045, Mann–Whitney U test.
Abbreviations: Modified-ALPPS, modified associating liver partition and portal vein ligation/embolization; PVE, portal vein embolization; T.bil, serum total bilirubin; Alb, serum albumin; Plt, platelet count; PT-INR, international normalized ratio of prothrombin time; volumetric %FLR (%), ration of the future liver remnant volume to the total liver volume; ICGK-F, future liver remnant plasma clearance rate of indocyanine green.
This was a single-center study, and it was approved by the ethics committee of Shimane University Faculty of Medicine (study number: 3723). Informed consent was obtained from all participants.
Procedure
Modified-ALPPS procedure
The first stage of modified associating liver partition preserving portal pedicle was performed by a surgeon (with 28 years of experience) along the resection line to the anterior surface of the inferior vena cava. 19 Parenchymal transection, preserving outflow via the hepatic vein, and sparring arterial and biliary branches to preserve arterial inflow, was conducted along either the falciform ligament for extended right hepatectomy or the median hepatic vein for right hepatectomy. Right portal vein ligation (PVL) was performed on patients with hepatic tumor (n = 4), and portal vein branch to segment 4 (P4) ligation was conducted for extended right hepatectomy. Otherwise, patients with perihilar and distal extrahepatic cholangiocarcinoma (n = 3) underwent PVE using the trans-ileocecal approach for the right portal vein to prevent adhesion in the perihilar site in staged hepatectomy. 20 The portal veins were embolized with absolute ethanol combined with detachable coils. Patients underwent the second stage of the surgery after 2 weeks, and major hepatectomy was then completed.
PVE procedure
The procedure was performed using the trans-ileocecal approach. The surgeons provided guidance for the ileocecal approach, and PVE was conducted by interventional radiologists (with 19 and 25 years of experience).
Occlusion of the portal vein was performed via the ileocecal vein using a 7-Fr sheath and a 6-Fr balloon catheter (9–20-mm Selecon MP catheter; Terumo, Tokyo, Japan). The balloon catheter was initially inserted, and digital subtraction portography was then conducted. The embolic materials comprised absolute ethanol (anhydrous ethanol; Mylan, Tokyo, Japan) combined with detachable coils. The volume of absolute ethyl alcohol required to perform embolization after the trial administration of contrast medium was determined while keeping the balloon inflated in the target branches. Occlusion of the target veins was the endpoint of embolization with absolute alcohol on direct portography 10 min after the procedure. Coil embolization was then performed on the right primary branches or the proximal part of the right anterior/posterior segmental branches. A two-marker microcatheter (Progreat β; Terumo Clinical Supply, Gifu, Japan) was inserted coaxially into the target vessel via the balloon catheter. The bare coil (Target 360; Stryker Japan K.K., Tokyo, Japan), a second-generation hydrocoil (AZUR CX; Terumo, Tokyo, Japan), was used for embolization. If there was no contrast flow distal to the coils after the administration of contrast medium on direct portography, coil embolization was achieved. Next, planned hepatectomy was performed after 4 weeks.
Assessments
Functional %FLR ratio
99 mTc-GSA SPECT/CT fusion imaging was performed using Discovery NM/CT 670 pro (GE Healthcare, WI, the USA) before and 1 week (modified-ALPPS group) and 3 weeks (PVE group) after the procedure. The patient received 185 MBq/3 mg of 99mTc-GSA (Nihon Medi-Physics, Tokyo, Japan) that was administered via the forearm vein after an overnight fast. Acquisition of SPECT data was initiated 20 min after injection using a low-energy, high-resolution collimator (90 steps at 15 s/step, 360°, 128 × 128 matrix). Then, SPECT images were reconstructed using a three-dimensional (3D) ordered subset expectation maximization algorithm with correction for both scatter and attenuation. Unenhanced CT scan images (120 kV, 10 mA, and slice thickness of 3.5 mm) were obtained, and images were reconstructed using a standard algorithm with a 500-mm field of view of the target sites. The SPECT slices were then transformed to CT-like data. Then, using Xeleris 3.1 (GE Healthcare), the SPECT and CT images were automatically fused.
Subsequently, resection lines were set on a composite display of the 99 mTc-GSA SPECT and CT images with a 3D image analysis system (SYNAPSE VINCENT; Fujifilm, Tokyo, Japan). 19 Next, the functional %FLR on 99 mTc-GSA SPECT/CT fusion imaging was calculated as follows:
Functional %FLR = future liver remnant count/ total liver count × 100.
Figure 1 shows the representative case. Functional future liver remnant (%FLR), future liver remnant volume (FLRV), and embolized liver volume (ELV) on the 3 dimensional (3D) image analysis system. 
The increasing ratio of functional %FLR ratio after the procedure was calculated as follows:
Functional %FLR ratio = post-functional %FLR/ pre-functional %FLR
Then, the functional %FLR ratio was compared between the modified-ALPPS and PVE groups.
FLRV and ELV ratio
All patients underwent four-phase 320-detector row computed CT scan (Aquilion One; Canon Medical Systems, Otawara, Japan) before and 1 week (modified-ALPPS group) and 3 weeks (PVE group) after the procedure. The patients received iodinated nonionic contrast medium (600 mgI/kg) within 30 s using a power injector. The iodinated nonionic contrast medium was iomeprol-350 (350 mgI/mL; Iomeron-350; Eisai Co., Ltd., Tokyo, Japan) or iopamidol-370 (370 mgI/mL; Iopamiron-370; Iopamiron; Bayer Yakuhin, Ltd., Osaka, Japan). One unenhanced and three enhanced images were acquired. For each phase, the scanning parameters were as follows: slice thickness: 0.5 mm, collimation: 0.5 mm, reconstruction interval: 0.3 mm, 120 kV, and auto-mA.
The 3D image analysis system, in its Liver Analysis Application, helped achieving preoperative simulation of the volume of the resection zone or the remnant liver volume. 19 Liver Analysis Application used multiple-phase images collected using dynamic CT scan to obtain the optimum contrast for each blood vessel. The volumes of interest were calculated from measurements made after outlining the liver segments and tumor contours on 0.5-mm-thick slices in the workstation. The resection lines were set using the 3D images, and both FLRV and embolized liver volume (ELV) were calculated. The middle hepatic vein, gallbladder, and portal vein branches were used as markers. Figure 1 shows the representative case.
The FLRV and total liver volume (TLV) were determined before and after the procedure. Then, the FLRV-to-TLV (volumetric %FLR) ratio was calculated using the following formula: Volumetric %FLR = FLRV (mL) / [TLV (mL) − tumor volume (mL)] × 100.
The tumor volume of patients with perihilar and distal extrahepatic cholangiocarcinoma was not calculated.
The hypertrophy ratio of FLRV after the procedure (FLRV ratio) was calculated as follows: FLRV ratio = post-FLRV (mL) / pre-FLRV (mL)
The atrophy ratio of ELV after the procedure (ELV ratio) was calculated as follows: ELV ratio = post-ELV (mL) / pre-ELV (mL)
Then, the FLRV and ELV ratio were compared between the modified-ALPPS and PVE groups.
Statistical analysis
Variables with a non-normal distribution were expressed as median (min–max), and those with a normal distribution as mean ± SD. The Shapiro–Wilk test was used to assess whether the variables had a normal distribution. If the variables had a non-normal distribution, the differences between the two groups were determined using the Mann–Whitney U test. If the variables had a normal distribution, the t-test was performed. Statistical analysis was performed using SPSS Statistics version 22.0 (IBM, New York, USA), and a p value of < .05 was considered statistically significant.
Results
All procedures were successfully performed, and 13 patients (n = 7, modified-ALPSS group; n = 6, PVE group) were analyzed. The mean functional %FLR ratio of the modified-ALPPS group (1.47 ± 0.15) was comparable to that of the PVE group (1.49 ± 0.20) (p = 0.939, Figure 2). The median functional %FLR increased from 28.6% to 46.2 (28.6 + 17.6) % in the modified-ALPPS group, from 39.0% to 61.09 (39.0 + 22.09) % in the PVE group. The median FLRV ratios were 1.48 (1.22–1.86) in the modified-ALPPS group and 1.16 (1.03–1.54) in the PVE group. Hence, the results significantly differed between the two groups (p = 0.045, Figure 3(a)). The median FLRV increased from 300 mL to 547 (300 + 247) mL in the modified-ALPPS group, from 457 to 567 (457 + 110) in the PVE group. The median ELV ratio of the PVE group (0.81 [0.71–0.84]) was significantly lower than that of the modified-ALPPS group (0.94 [0.78–1.44]) (p = 0.006, Figure 3(b)). The median ELV decreased from 802 mL to 798 (802 - 4) mL in the modified-ALPPS group, from 834 mL to 682 (834 - 152 ) mL in the PVE group. Then, all patients were performed a planned major hepatectomy, but the operation was discontinued for the local progression in one patient of the PVE group. PHLF was categorized according to the criteria of the International Study Group of Liver Surgery (ISGLS) (20). There were five patients with PHLF-Grade A, one patient with PHLF-Grade B and one patient with PHLF-Grade C in the modified-ALPPS group (n = 7). There were five patients with PHLF-Grade A in the PVE group (n = 6). Increasing ratio of functional future liver remnant (%FLR ratio). The mean function %FLR ratio was 1.47 ± 0.15 in the modified associating liver partition and portal vein ligation/embolization (modified-ALPPS) group and 1.49 ± 0.20 in the portal vein embolization (PVE) group. Hence, the results did not significantly differ (p = .939). Hypertrophy ratio of the future liver remnant volume (FLRV ratio) and atrophy ratio of the embolized liver volume (ELV ratio). 

Discussion
In the current study, the increasing ratio of functional %FLR was similar in the modified-ALPPS group at 1 week and PVE group at 3 weeks. Whether a high FLRV reflects a greater future liver remnant function was questioned based on a recent review of data in the ALPPS registry, which showed that most cases of mortality after the second stage of surgery was attributed to PHLF despite an increased FLRV. 21 The increase in FLRV exceeded the future liver remnant function at day 6 after the first stage of ALPPS. However, the functional growth rate was higher after the second stage. This resulted in comparable values between FLRV and future liver remnant function on day 28 after the second stage of ALPPS. 16 Compared with PVE, the modified-ALPPS procedure resulted in a comparable increasing ratio of functional %FLR only after 1 week. However, a greater functional growth could be expected according to that report. ALPPS has several possible advantages, which include the comparable increase in functional %FLR within a short period and the reduced risk of disease progression such as metastasis and dissemination by shortening the waiting period before the second stage of hepatectomy. A randomized, controlled study showed that ALPPS improved resection rates compared with the traditional two-stage hepatectomy with PVL or embolization. Moreover, the 90-day mortality rate, incidence of severe complications, and rate of negative surgical margins in the liver were low. 22
The FLRV ratio of modified-ALPPS was higher than that of PVE. However, atrophy of the embolized liver was less severe in modified-ALPPS than in PVE in the current study. The modified-ALPPS group had significantly lower both functional and volumetric FLRs than the PVE group. These are crucial factors influencing liver hypertrophy. 23 It might be more advantageous for liver hypertrophy in the modified-ALPPS group than the PVE group. Also, Schlegel et al. performed a rodent study that showed increased interleukin-6 (IL-6) levels in the plasma and IL-6 and tumor necrosis factor alpha levels in liver tissues 1 h after the first stage of ALPPS compared with PVL in both mice and humans. 24 Atrophy of the embolized liver was less severe in the modified-ALPPS group than in the PVE group. In addition, the systemic increase in circulating growth factor levels might have affected the ELV.
In this research, partial associating liver partition, which can preserve portal pedicles, was performed. Tanaka et al. proposed a modified-ALPPS in which the portal pedicles along the transection lines are preserved to prevent ischemic areas along the transection line. These ischemic segments act as a nidus for infection, and they increase the risk of sepsis, which is the main cause of mortality. 25 Petrowsky H et al. revealed that partial ALPPS, which can spare some branches of the portal pedicles, is associated with a low risk of serious complications (0%) (Clavien–Dindo IIIb) 11 days after surgery. 26 In patients who underwent modified-ALPPS, the FLRV increased (63.8% ± 38.4%) 1 week after the first stage of surgery. This result was comparable to that of classical ALPPS. 27 Previous PVE studies showed that FLRV increased by 10%–46% within a 3- to 7-week interval between PVE and hepatectomy.28–31 Sakamoto et al. revealed that associating liver partial partition and trans-ileocecal PVE for staged hepatectomy facilitated the first stage of surgery without causing bile leakage or infectious complications. 32 The second stage of major hepatectomy was easier to perform due to the no-touch policy on the hepatoduodenal ligament because there is less adhesion in the hepatoduodenal ligament.
The current study had several limitations. First, it was a retrospective investigation conducted at a single center, and only few participants were included. Thus, the current findings should be considered as preliminary, and future studies must be conducted to validate such results. Second, functional %FLR, FLRV, and ELV were not evaluated at a similar interval after the procedures between the modified-ALPPS and PVE groups. Third, the indications and tumor entities for modified-ALPPS and PVE differed. Fourth, other embolic materials for PVE were not evaluated, and the liver condition of each patient differed, which might have influenced the FLRV ratio. Furthermore, 99 mTc-GSA SPECT/CT fusion imaging cannot be used in clinical settings in several countries, even though there have been several reports about the use of this radiopharmaceutical method in Japan and elsewhere.
In conclusion, the increasing ratio of functional %FLR was comparable between modified-ALPPS and PVE, while it was a retrospective investigation with only few participants. Compared with PVE, modified-ALPPS was associated with a higher hypertrophy rate of the remnant liver but a lower atrophy rate of the embolized liver.
Footnotes
Author contributions
Mitsunari Maruyama performed manuscript writing and contributed to critical revision of the manuscript for important intellectual content. Mitsunari Maruyama,Takeshi Yoshizako, Rika Yoshida and Megumi Nakamura contributed to surgical resection and data collection of all cases and performed data collection. Yoshitsugu Tajima and Hajime Kitagaki gave final approval of the manuscript. All authors were involved in the manuscript and have agreed to the content.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship,and/or publication of this article.
Ethical approval
The study was approved by the ethics committee of Shimane University Faculty of Medicine (study number: 3723) and conducted in compliance with the Declaration of Helsinki guidelines.