
Abstract
Evaluation of COVID-19 related complication is challenging in pregnancy, due to concerns about ionizing radiation risk to mother and the fetus. Although there are instances when diagnostic imaging is clinically warranted for COVID-19 evaluation despite the minimal risks of radiation exposure, often there are concerns raised by the patients and sometimes by the attending physicians. This article reviews the current recommendations on indications of chest imaging in pregnant patients with COVID-19, the dose optimization strategies, and the risks related to imaging exposure during pregnancy. In clinical practice, these imaging strategies are key in addressing the complex obstetrical complications associated with COVID-19 pneumonia.
Introduction
Corona virus disease of 2019 (COVID-19) is a viral disease caused by severe acute respiratory syndrome-Coronavirus-2 (SARS-COV-2). 1 The disease first originated in the Hubei province of China, later sweeping through the continents and evolving to become a global pandemic. The detailed insights into the disease manifestations, heterogeneity, and physiological behavior of the virus, including pulmonary and extra pulmonary manifestations of COVID-19, are being better understood with new research studies and clinical experiences.
There is a relative higher risk of COVID-19 infection during the time of pregnancy, 2 thereby creating constraints and clinical dilemma on proceeding with the use of an appropriate radiological investigation. 3 The clinical pathway for evaluating COVID-19 and its associated complications in pregnancy is highly variable, depending on the institutional preferences, availability of resources, practice pattern of referring clinicians, and interpreting radiologist. Imaging studies which involve radiation exposure like chest X-ray and chest CT scan are indispensable in the management of COVID-19 patients. Radiologists around the globe should be familiar with merits and limitations of various chest imaging modalities in evaluation of COVID-19 pneumonia and its complications during pregnancy. In this review, we aim to summarize the current recommendations on indications of chest imaging in pregnant COVID-19 patients including chest X-ray, CT chest, CT pulmonary angiogram, chest ultrasound, and cardiac MRI, with emphasis on imaging risks and dose optimization strategies.
Features of COVID-19 in pregnancy
Epidemiology
Recent surveillance data from the Centers for Disease Control and Prevention (CDC), in the women aged between 15 to 44 years, showed pregnant women were more likely to be hospitalized, requiring an intensive care unit (ICU) care or ventilation. 4 However, large cohort study from the United Kingdom observed that the rates of ICU admission or maternal mortality in severe disease were similar to non-pregnant women in the reproductive age group. 5 Pregnant women are more susceptible to infections owing to the immunity changes during the time of pregnancy. 6 There are guidelines from the CDC, the American College of Obstetricians and Gynaecologists (ACOG), the Society for Fetal-Medicine (SMFM), and the Royal College of Obstetrics and Gynaecologists (RCOG) related to the management of COVID-19 in pregnancy.7–13
Complications related to COVID-19 in pregnancy
Chest complications related to COVID-19 in general include a spectrum of findings related to airway, alveolar, vascular, and cardiac involvement. Recent studies have shown an increased incidence of complications in pregnancy due to COVID-19, especially preeclampsia, eclampsia, HELLP syndrome, and increased risk for maternal mortality. 14 Furthermore, the complications are augmented with pre-existing or underlying comorbidities like obesity, diabetes mellitus, systemic hypertension, and cardiac diseases. 15
Diagnosis and clinical severity classification in pregnancy with COVID-19
Clinical disease spectrum in patients with COVID-19.

COVID-19-corona virus disease 2019; NAAT- nucleic acid amplification test, RT-PCR- reverse transcriptase polymerase chain reaction.* Disease severity that might require an imaging with chest X-ray, CT chest, or CT pulmonary angiogram depending on the clinical assessment and disease status
Evaluation of COVID-19 pneumonia in pregnancy
(1) Utility of chest X-ray
Recommendations
The position statement by Fleischner society and ACOG recommends that routine imaging should not be used in asymptomatic or mild illness severity patients and also in intubated stable patients with COVID-19.8,23 The ACOG and SMFM recommends chest X-ray in patients with moderate clinical risk based on illness severity and underlying comorbidities in all trimesters, 10 while the RCOG recommends that the radiographic investigations such as chest radiograph and CT chest should be performed in pregnant patient with COVID-19 as for the non-pregnant adult and chest imaging should be performed when indicated and should not be delayed over concerns of fetal radiation exposure, as the maternal well-being is paramount. 13 In practice, chest X-ray should not be used for arriving at a diagnosis of COVID-19 in pregnant patients, instead it is recommended to rely on RT-PCR confirmation of the disease status. Follow-up chest X-ray should be judiciously considered only when there is further clinical deterioration and situations that would impact patient care.
Optimization strategies in chest x-ray
In routine chest X-ray, the pelvis or gravid uterus is generally not exposed to direct X-ray beam, and can be safely performed with optimization strategies. 24 However, in third trimester due to gravid uterus reaching the upper abdomen, parts of fetus can get exposed to a direct X-ray beam, and this needs to be taken care of using an appropriate technique. Dose optimization strategies to reduce the maternal and fetal dose include collimating on the lungs and avoiding upper abdomen as much as possible with an abdominal lead shield 25 placed over the abdomen or back depending on Antero-Posterior (AP) or Postero-Anterior (PA) radiographs, respectively, and also to limit the chest radiograph to frontal view and avoiding a lateral radiograph. 24
(2) Utility of CT
Pattern of lung involvement in COVID-19 includes ground glass opacities (GGO), GGO with consolidation, and only consolidation are similar to non-pregnant patients.26–29 However, the imaging findings have close overlap with other viral lung infections like influenza virus, MERS-COV, SARS, H1N1, H5N1, and H7N9.26,27
Recommendations
The position statement by the American College of radiology (ACR) 30 recommends against the use of CT scan as a first-line investigation or for follow-up to assess progression of COVID-19. The Fleischner Society advocates CT scan only in patients with functional impairment, hypoxemia, or after recovery from infection. The SMFM, ACOG, and RCOG recommend that CT chest should not be withheld in pregnant patients when clinically indicated.10,13 Thus, in pregnant patients the CT chest should be undertaken only in instances where there is functional impairment, hypoxemia, or both.
Unlike other lower respiratory tract viral infections, respiratory decompensation in COVID-19 pneumonia happens later in the disease. 31 Hypoxemia related to acute respiratory failure in pregnancy manifests with partial pressure of oxygen (PaO2) <60 mmHg on room air, that corresponds to oxygen saturation (SpO2) <90 mmhg on room air or sea level.32,33
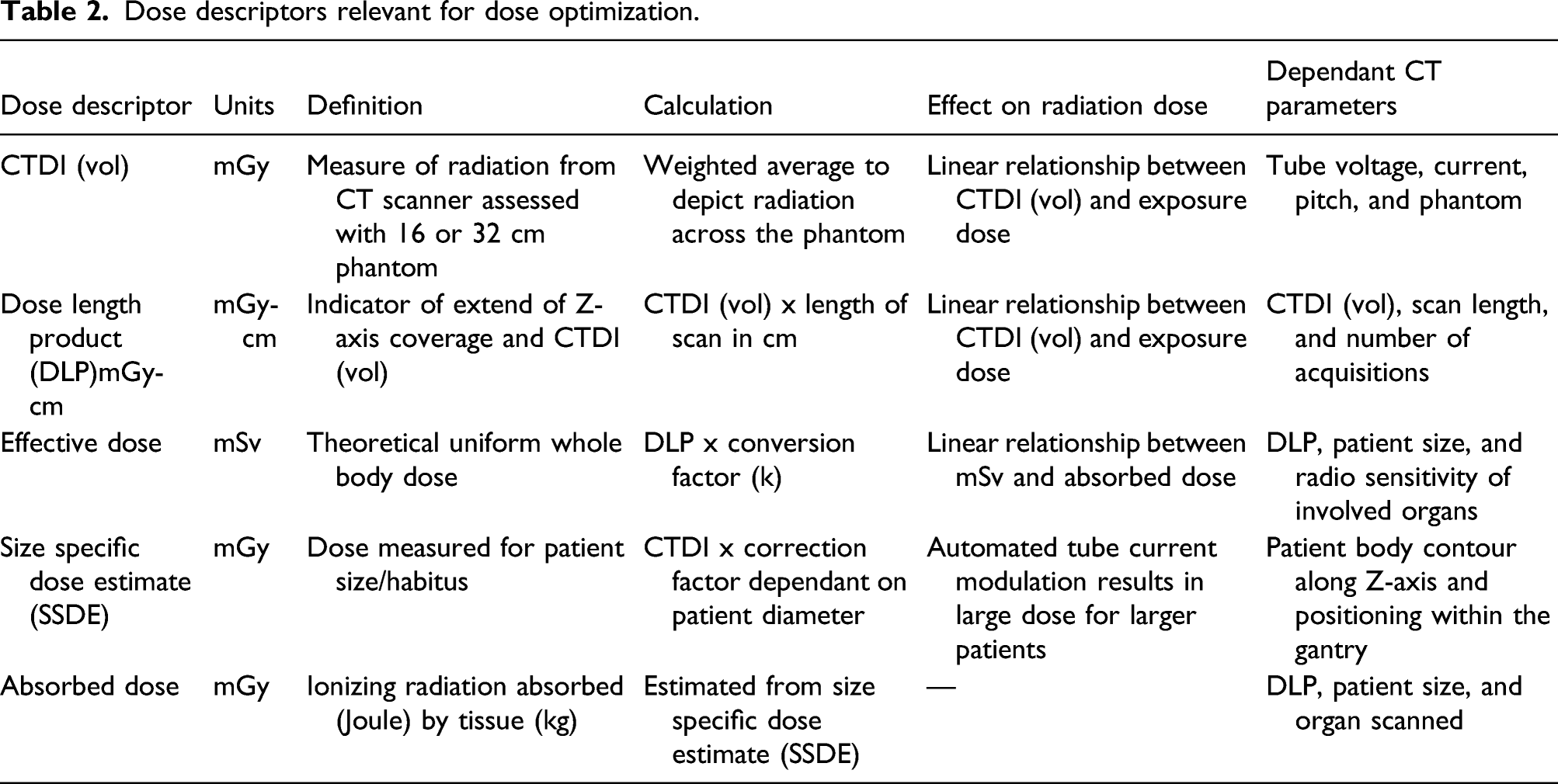
Optimization and dose reduction strategies in CT
Dose descriptors relevant for dose optimization.
Dose optimization strategies.
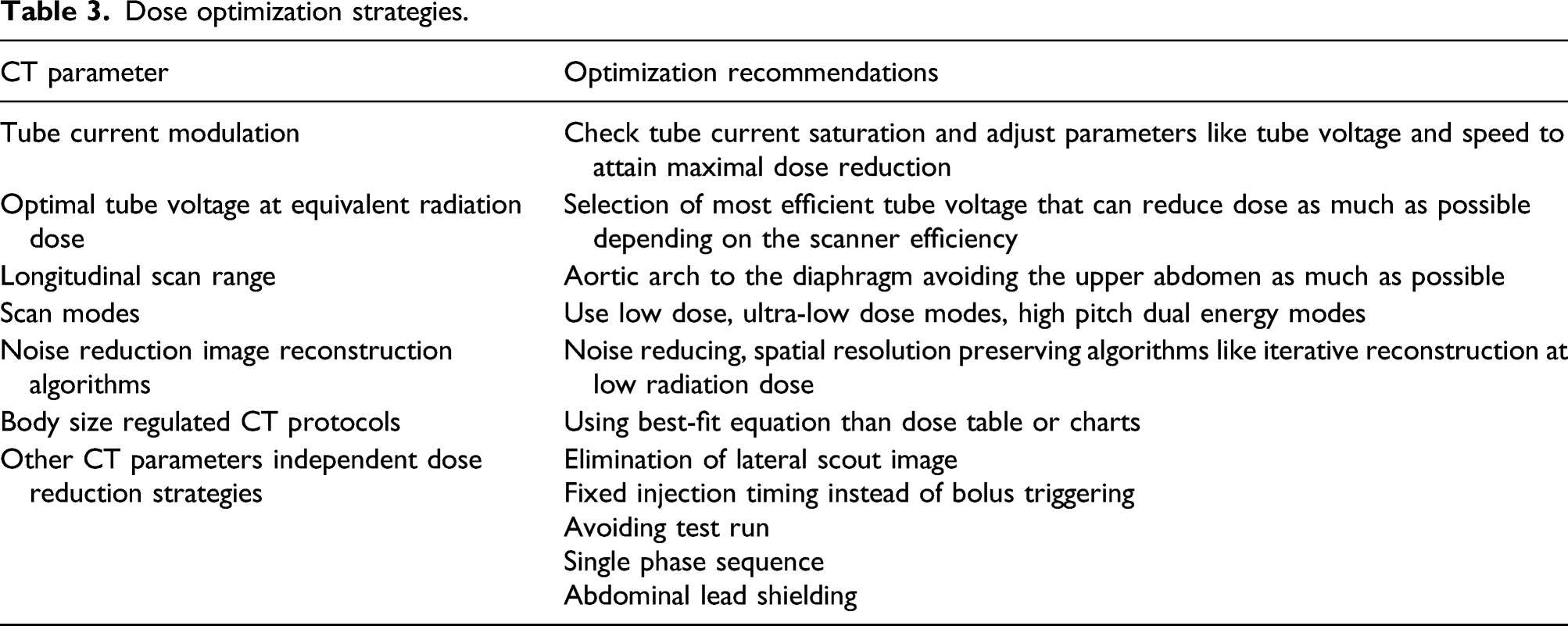
Overall, the dose reduction strategies should be tailored depending on the resources available with the institution, and the focus should be on implementing a low dose or ultra-low dose strategies for CT imaging in pregnant patients with COVID-19 and to bring down the effective dose below 3 mSv. 41
(3) Utility of chest USG
The International Society of Ultrasound in Obstetrics and Gynecology (ISUOG) recommends using an ultrasound for lung examinations in pregnant patients with COVID-19 as it has the advantage of being radiation free and can be performed at the same time along with obstetric ultrasound which in turn saves time and improves the clinical workflow. Also it can be considered as an alternate when chest radiograph or CT scan is not available. 42 On ultrasound, the normal horizontal “A-lines” (A-lines refers to horizontal echogenic reverberation artefacts that occur in normal lungs, beneath the pleural line at multiples of distance between the ultrasound probe and visceral-parietal pleural interface) are replaced by abnormal “B-Lines” when there is early loss of aeration but not completely consolidated (B-Lines refers to artefact in ultrasound caused as a result of loss of aeration in alveolar-interstitial space). While a consolidation results in absence of A- and B-lines, with a hyperechoic “white lungs”.
Evaluation of pulmonary embolism in pregnancy with COVID-19
Utility of CT pulmonary angiogram
Pulmonary embolism is reported to occur commonly in patients with COVID-19 with a reported incidence ranging from 0.7–57%, more often associated with severe disease. 43 Pregnancy is associated with a five-fold increased risk for developing pulmonary embolism, due to decreased fibrinolysis, hypercoagulability status, venous stasis, and prolonged bed rest. Pulmonary embolism is also a leading cause of maternal death during pregnancy, and the diagnosis during pregnancy has significant implications in planning of delivery and anticoagulation therapy.44,45 In planning an imaging for COVID-19 to rule out pulmonary embolism, all patients should have been thoroughly evaluated on the pre-test probability of pulmonary embolism using Pulmonary embolism rule out criteria, 46 Wells score, 47 Geneva score, 48 and D-Dimer when indicated. The role of D-dimer assay is limited in pregnant patients as the value can arise above the reference levels as the pregnancy progresses. 49 However, normal D-dimer levels have a high negative predictive value in ruling out pulmonary embolism.
Diagnostic imaging with CT pulmonary angiography is considered a clinically warranted investigation in pregnant patients suspected of pulmonary embolism with COVID-19.
13
However, the initial workup should focus on non-ionizing imaging techniques like lower extremity color Doppler ultrasound. Although the prevalence of lower limb deep vein thrombosis with clinically suspected pulmonary embolism in COVID-19 is uncertain, the advantage of getting a positive deep vein thrombosis on duplex ultrasound is considered sufficient to justify the use of anticoagulation therapy, thereby eliminating the need for further CT pulmonary angiography.
50
If the initial tests are non-diagnostic, CT pulmonary angiography should be performed as a second line investigation. Figure 1 summarizes a practical diagnostic algorithm for evaluating a pregnant patient with suspected pulmonary embolism in COVID-19.
51
In a setting of COVID-19, the CT pulmonary angiography is preferred over V/Q scintigraphy as it can be used to assess the severity of lung changes for COVID-19 as well. Diagnostic algorithm for evaluation of pregnant patients with COVID-19 suspected of pulmonary embolism.
If there is a positive pulmonary embolism, deep vein thrombosis, or when there is maternal hypoxemia, an obstetric ultrasound for fetal growth, amniotic fluid, and color Doppler imaging should be performed when necessary to assess the extent of fetal hypoxemia. 52
Risks related to contrast media
The risks related to iodinated contrast material include the possibility of nephrotoxicity and allergic reactions, with similar relative risks for pregnant and general population. The contrast should not be administered when there is prior major allergic reaction to iodinated contrast material or an underlying impaired renal function. Although, the iodinated contrast crosses the placenta to reach the fetus, there are no reported risks for the fetus. There is a theoretical risk of contrast-induced thyroid dysfunction and hence thyroid function screening should be performed in neonates although there is no convincing evidence to support the same.53,54
The use of gadolinium should be restricted in pregnancy as few studies have shown association between gadolinium exposure in utero to still births and neonatal deaths. The US Food and Drug Administration (FDA) has categorized gadolinium as pregnancy class 3 drug. 55
Evaluation of myocarditis in pregnancy with COVID-19
Utility of Cardiac MRI
There is evidence of varying manifestation of myocardial injury associated with ongoing or recently recovered COVID-19 patients, with myocarditis being the most common pattern (in 40% cases) while other complications include myocardial ischemia, right ventricular strain, cardiac thromboembolism etc. 56 Few studies have indicated that the mapping abnormalities and cardiac involvement can be picked up early in the disease with cardiac MRI. 57 Cardiac MRI has shown to be a safe imaging in pregnancy with no risk to the mother. Theoretical concerns of teratogenesis, acoustic damage, and tissue heating have not been sufficiently proven in humans. Moreover in cardiac MRI, field of view is away from the fetus, thereby further reducing the potential harm. 58 There is no different risk in relation to different trimesters as per the American College of Radiology (ACR). 59 The information related to utility of cardiac MRI in pregnant patients with COVID-19 is limited, and with the absence of specific recommendations, the use of cardiac MRI can be considered in pregnancy on a case-to-case basis, and also on the resource availability.
Evaluation of fetal hypoxemia due to maternal pulmonary compromise
Hypoxemia due to maternal respiratory failure in COVID-19 leading to poor oxygenation to placenta and fetus can result in fetal distress.60,61 Although the emerging evidence suggests vertical transmission is probable, the significance of the same to the neonate is yet to be ascertained. There are emerging data that indicate that this viral infection causes inflammation, villitis, and arteriopathy in placenta.62,63 Fetal distress and preterm pregnancy are common obstetrical complications of COVID-19. 64 Assessment for acute placental insufficiency and fetal hypoxia can be easily assessed with obstetric Doppler ultrasound.65,66 The placental and fetal consequences of COVID-19 including the utility of functional MRI in fetal hypoxemia related to COVID-19 remain to be explored.
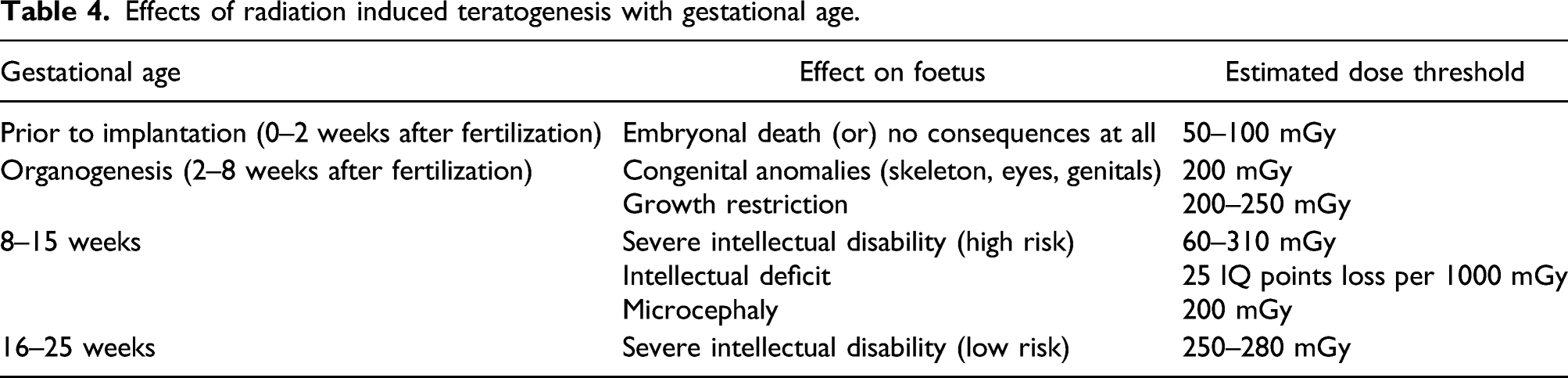
Radiation exposure thresholds during pregnancy
Effects of radiation induced teratogenesis with gestational age.
Informed Consent and patient counseling
Informed consent and patient counseling are important to alleviate the anxiety of patients, while undergoing imaging modalities with radiation exposure like the chest X-ray or CT scan. The attending physician should convey the outweighed benefits of doing an imaging to assess the disease status or to evaluate the complications of COVID-19, as opposed to the risk on the fetus leading to congenital anomalies, birth defects, and miscarriage although negligible for the radiation dose received by the patient. The attending physician and the radiologist should confirm the patients understanding of the estimated risk to mother and fetus. In practice, patient can be explained about the imaging-related radiation exposure by comparing it with background population risk which is approximately 4%, 10%, 10%, and 20% for malformations, genetic diseases, growth retardation, and pregnancy loss, respectively. 71
Conclusion
Chest radiograph and CT examinations for COVID-19 evaluation deliver minimal radiation dose to the mother and fetus, and rarely exceed the permissible limit of 50mGy. Although this knowledge should reassure pregnant women and attending physician on the greater benefits of undergoing an imaging for COVID-19 evaluation, over the minimal radiation risks, the management strategy should focus on keeping the radiation exposure to both mother and fetus as low as reasonably achievable according to ALARA principles. Radiologists should be aware of the lack of understanding about the radiation risk among the non-radiologist physician who would be requesting an imaging during the care of a pregnant COVID-19 patient, and it’s the responsibility of radiologist to counsel the treating physician with regard to various options available for chest imaging including radiation-free modalities like chest USG and cardiac MRI when appropriate for evaluation of COVID-19 related chest complications in pregnancy and to improve patient care.
Footnotes
Author contributions
Article concept, design, manuscript drafting/editing/revision for important intellectual content and Literature research all authors. Final version of manuscript is approved by all authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The publication of this article was funded by the Qatar National Library.
Informed consent
Informed consent was waived by IRB (Institutional Review Board) for this review article.
Guarantor
AN