
Abstract
Purpose:
To explore the clinical and dynamic computed tomography features of coronavirus disease 2019.
Methods:
We enrolled 24 patients with coronavirus disease 2019 treated at a regional center in Dezhou, China, from January 22 to February 5, 2020, and analyzed data retrospectively.
Results:
Nineteen cases had close contact with people with coronavirus disease 2019, and five patients denied a travel history in Wuhan City or contact with patients having coronavirus disease 2019. Symptoms were fever, cough, chest tightness, dyspnea, fatigue, and muscle pain. Chest computed tomography showed multiple ground-glass opacities distributed along peribronchial bundles and subpleural areas, often accompanied by bronchiectasis, vascular thickening, and interlobular septal thickening after coronavirus disease 2019 progression.
Conclusions:
Coronavirus disease 2019 has certain clinical characteristics and typical computed tomography features.
Introduction
The Director General of the World Health Organization, Tan Desai, announced on February 11, 2020, that the new coronavirus that was causing pneumonia (initially in China) was to be named coronavirus disease 2019 (“COVID-19”). Simultaneously, the International Virus Classification Commission named the new coronavirus “severe acute respiratory syndrome coronavirus 2”. 1
In humans, COVID-19 transmits by droplets and contact and is spreading rapidly. 2 -4 We wished to help to improve the early diagnosis, isolation, and treatment of COVID-19, and prevent pneumonia progression. We collected the data of 24 patients with COVID-19 treated at center in Dezhou, China, from January 22 to February 5, 2020. We summarized the clinical manifestations and computed tomography (CT) features. In this way, we wished to understand the disease fully and improve its diagnosis and treatment.
Methods
Ethical Approval of the Study Protocol
The study protocol was approved by the Picture Archiving and Communication Systems (PACS) center review board in De Zhou and its research ethics committees. Our analysis was in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and later amendments. Patients provided written consent for their data to be used in our study.
General Information
A retrospective analysis was conducted on 24 cases with COVID-19 confirmed by detection of virus specimens and hospitalization. The study group comprised 16 men and 8 women (18-83 [mean 48.80 ± 17.41] years). Complete data (clinical and CT) were available for all patients.
Computed Tomography Scanning
All patients in the present study underwent CT of the lung. A 128-slice spiral CT system (LianYing, Shanghai, China) was employed. Computed tomography was done on automatic-exposure, dose-adjustment mode at 80 to 120 kVp, and automatic milliampere-second. The scanning range covered the whole lung tissue. Conventional layer thickness was 5 mm using lung-algorithm and standard-algorithm double-window technology. Data were reconstructed at intervals of 1.1 or 1.25 mm using the Sharp algorithm.
Image Analyses
Two experienced chest radiologists in this regional PACS center read the CT images without prior knowledge of the diagnosis of COVID-19. At the early stage of COVID-19, CT showed a ground-glass opacity (GGO) around the bronchial tract. The progression stage was characterized by an increased GGO density with small grid shadows, as well as solid marginal GGO, which was often accompanied by intraluminal bronchiectasis and thickening of adjacent vessels. In the severe stage, CT showed a “white lung.” In the resolution stage, CT showed the lesions becoming smaller and being absorbed completely. 5
Results
Residence and Travel History of Patients
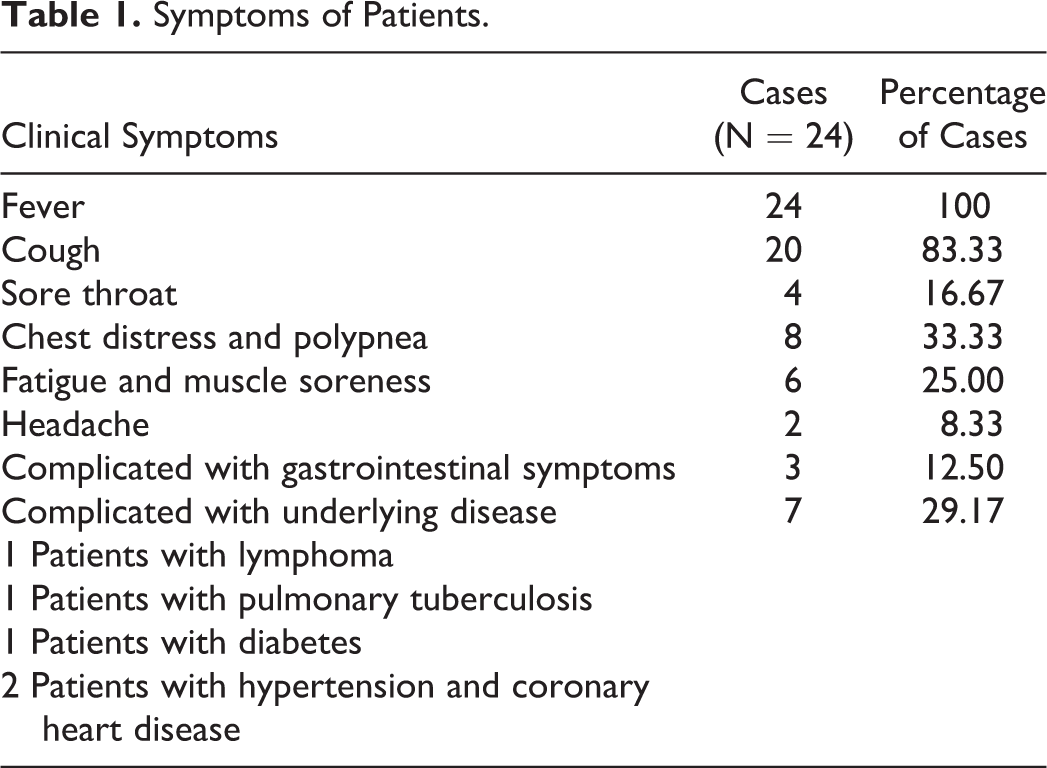
Among the 24 patients, 9 patients had a history of travel or residence in Wuhan City (Hubei Province, China). Ten patients demonstrated clustered spread between married couples, parents, and friends. Five patients denied a travel history in Wuhan City or contact with patients confirmed to have COVID-19. The first symptom was fever in all cases. The clinical manifestations of patients are shown in Table 1.
Symptoms of Patients.
Laboratory Examination
The white blood cell (WBC) count was within normal range in 14 cases but decreased in 10 cases. The neutrophil count was within normal range in 15 patients and decreased in 9 cases. The lymphocyte count was within normal range in 6 cases and decreased in 18 cases. The C-reactive protein level was normal in 2 patients and increased in 22 patients; in patients with severe disease, it was increased obviously. The seropositive protein A level was increased in all patients, especially in 5 patients with severe COVID-19 (≥200 mg/L). Specimens from the respiratory tract from all patients tested positive for COVID-19 according to reverse transcription-polymerase chain reaction.
Computed Tomography Features
Computed tomography of the chest of all patients showed lesions at the first visit. Multiple lesions were distributed in the extrapulmonary subpleural area. In 15 cases (66.7%), lesions were present in all lung lobes and showed a diffuse distribution, In 5 (20.8%) patients, lesions were involved 2 to 3 lung lobes. In 4 (16.7%) cases, focal lesions were involved a single lobe. Computed tomography features are shown in Table 2.
Computed Tomography Features of Patients.
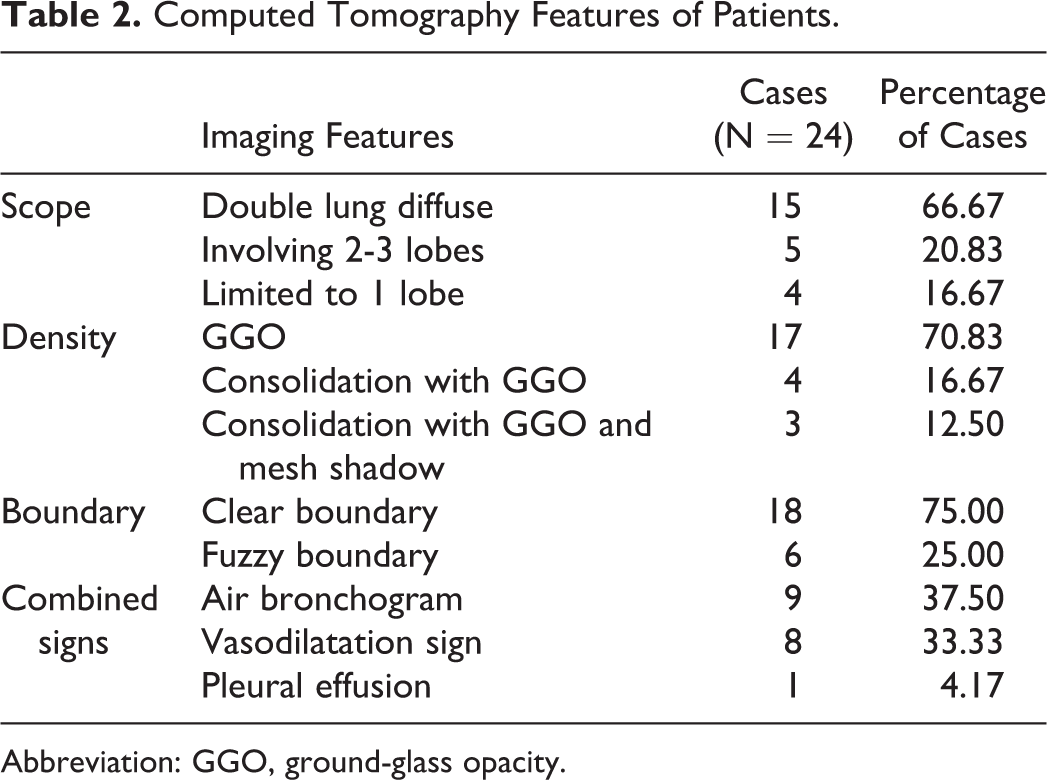
Abbreviation: GGO, ground-glass opacity.
Features of Dynamic CT
According to the diagnostic guidelines for COVID-19 (2020, first edition), 6 17 patients had “mild” COVID-19 and 7 cases had “severe” COVID-19 at the first visit. The 17 cases of “mild COVID-19” presented with single-lobe or multi-lobe GGO at the early stage of COVID-19.
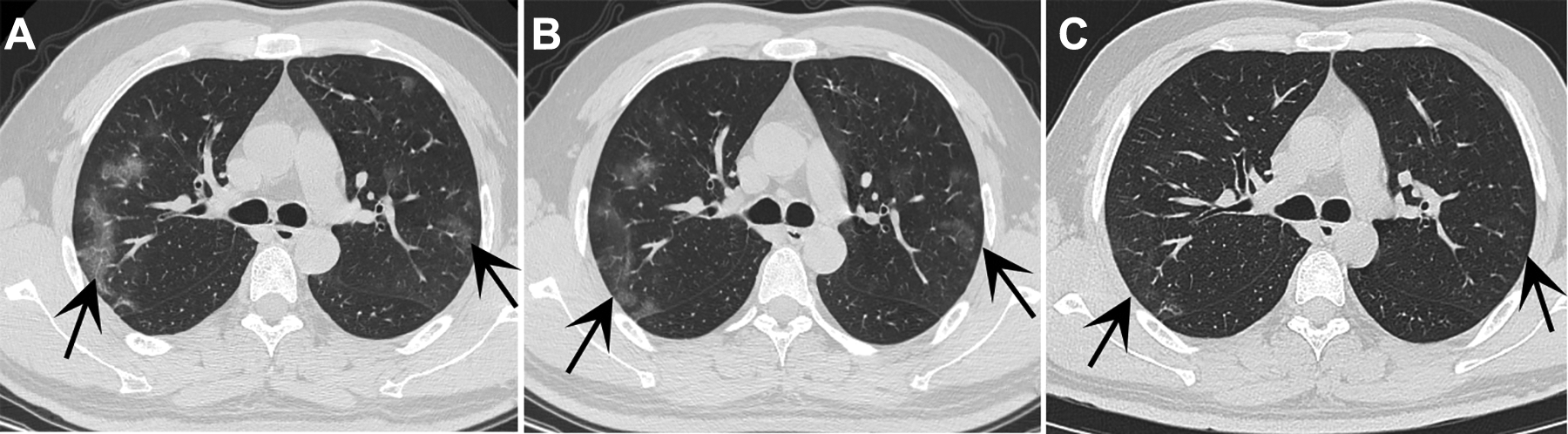
In the progression stage, the range and density of lesions were increased (Figure 1). Small grid shadows were seen in 8 cases, solid lesions with GGO were observed in 7 cases, and 2 patients progressed to severe COVID-19 (Figure 2).
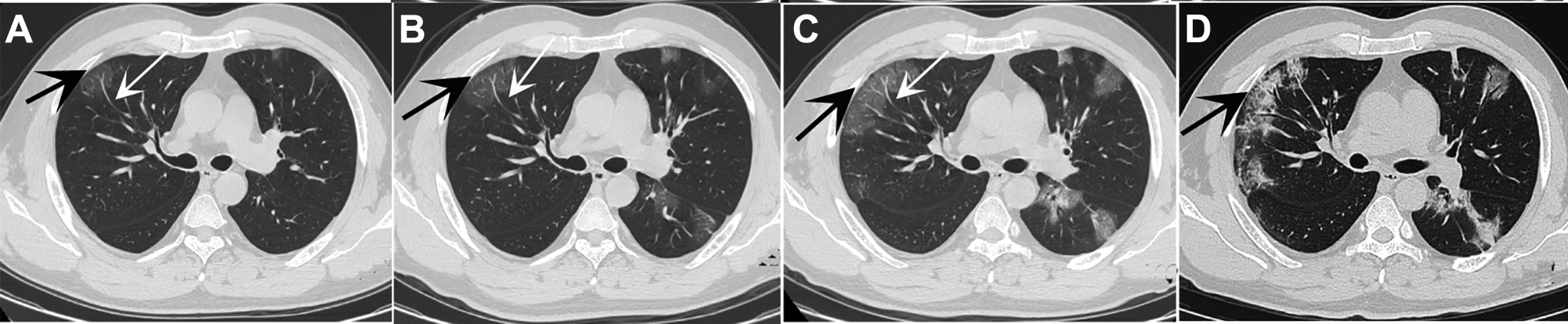
A 47-year-old man with COVID-19. He was living in Wuhan City and had fever for 3 days. Computed tomography showed diffuse GGO in both lungs. Upon his first visit on January 25, 2020, lesions were distributed around bronchial and vascular bundles and subpleural areas around the periphery of the lung (A). The black arrows are pointing to the lesion. The GGO increased gradually and lesion density had increased upon review on January 27 (B), January 29 (C), and February 4 (D). As pneumonia progressed, visible lesions and bronchiectasis, vascular enlargement (A-C, white arrows), and partial chordae (D) were observed. COVID-19 indicates coronavirus disease 2019; GGO, ground-glass opacity.
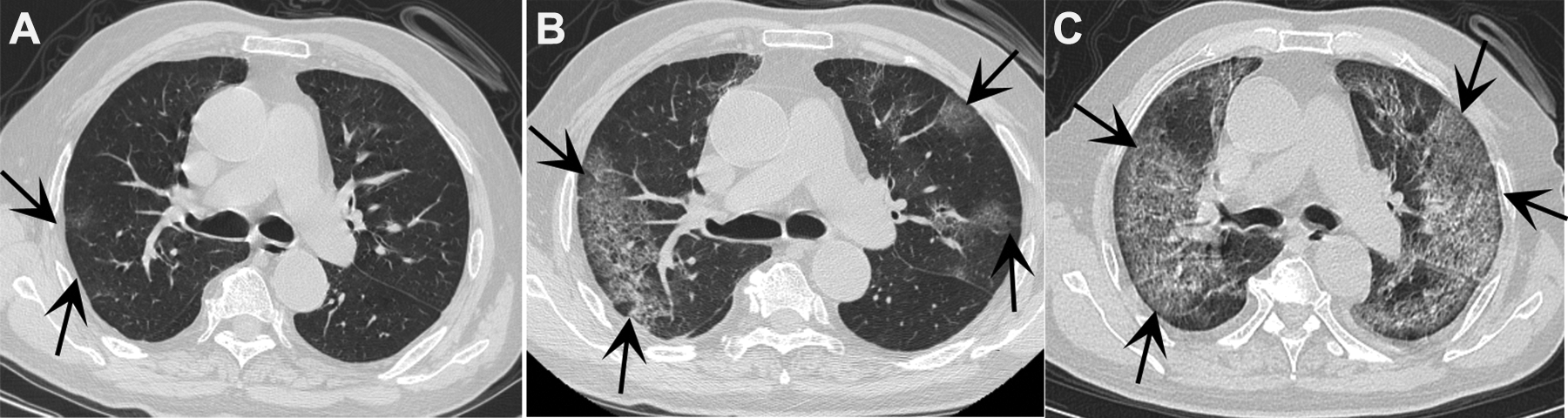
A 79-year-old man with COVID-19. He had a history of high blood pressure. He had contact with his son, who had returned from Wuhan City, and been diagnosed with COVID-19. He had fever of 2-day duration. Fever was accompanied by chest tightness, dyspnea, palpitation, fatigue, and muscle pain. Upon his first visit on January 30, 2020, CT showed patchy GGO in subpleural regions of the upper lobe (A). The black arrows are pointing to the lesion. Increased GGO, increased density of lesions, and fusion into large areas, with small grid-like changes in the lesion, were noted on February 2 (B) and February 5, 2020 (C). CT indicates computed tomography; COVID-19, coronavirus disease 2019; GGO, ground-glass opacity.
In the resolution stage, the lesions shrank in 5 cases, 2 patients had local “residual strips” (Figure 3) and in 3 cases the lesions had been resolved completely. Among 7 patients with severe COVID-19 (Figure 4), the lesions progressed in 3 cases, narrowed and became deformed in 3 patients, and were resolved in 1 case.
A 35-year-old man with COVID-19. He had been transferred from Wuhan City on January 17, 2020. He had a fever on January 23, 2020. Computed tomography showed multiple flaky GGO in the subpleural area of both lungs on his first visit on January 27, 2020 (A). The black arrows are pointing to the lesion. The range and density of lesions decreased on January 30, 2020 (B). Lesions were improved considerably and had mostly disappeared by February 2, 2020 (C). COVID-19 indicates coronavirus disease 2019; GGO, ground-glass opacity.
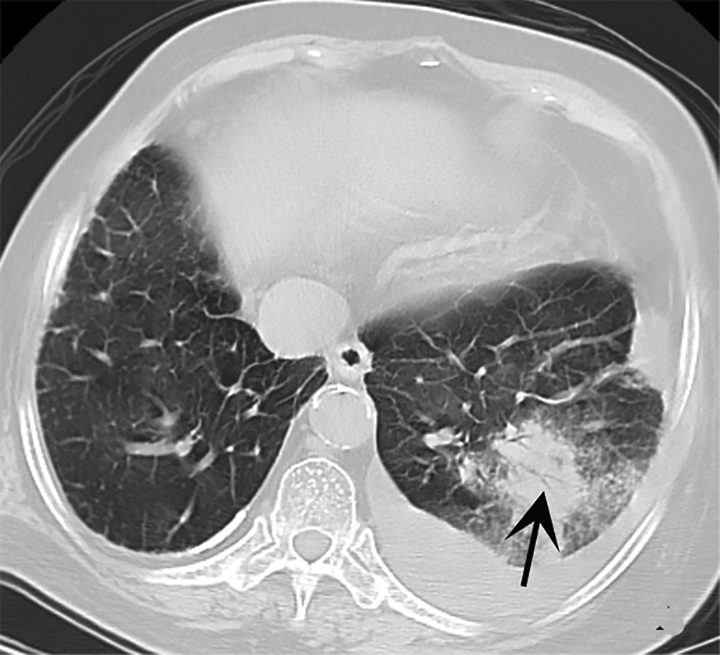
An 82-year-old woman with COVID-19. She had a history of tuberculosis. She had contact with her son, who had returned from Wuhan City and had been diagnosed with COVID-19. She had a fever for 3 days accompanied by fatigue, loss of appetite, and muscle pain. Computed tomography showed large patchy consolidation of the lower lobe of the left lung, air bronchogram, GGO at most edges of the lesion, and left pleural effusion. The black arrows are pointing to the lesion. COVID-19 indicates coronavirus disease 2019; GGO, ground-glass opacity.
Treatment and Prognosis
During hospitalization, all patients received symptomatic supportive treatment to combat viral/bacterial infection and interstitial fibrosis. Up until now, 4 cases recovered and were discharged from hospital, 15 patients are stable, and 5 cases had serious COVID-19 complicated by acute respiratory distress syndrome. Among those 5 patients, 3 cases were aged >80 years; 1 had a history of lymphoma, 1 had a history of tuberculosis, 1 was suffering from diabetes mellitus, and 2 had a history of hypertension and coronary heart disease.
Discussion
Coronavirus disease 2019 has spread rapidly to several provinces and cities in China since the outbreak in Wuhan City in December 2020. Due to a general lack of immunity to COVID-19, a widespread epidemic in China has occurred. 7 -9
Coronavirus disease 2019 is characterized by being highly infectious with rapid speed of transmission. It can infect children and adults with normal or abnormal immune function and poses a significant threat to human health. Coronavirus disease 2019 progresses slowly within 7 days, and often the symptoms are not obvious. After 7 days, disease tends to worsen and change rapidly, and the risk of death is higher if comorbidity is present. 10,11 In our study, the 5 patients with severe COVID-19 were elders or had a comorbidity: This population carried a poor prognosis.
Nine patients had a history of travel to or residence in Wuhan City, and 10 patients demonstrated clustered spread between married couples, parents, and friends. Hence, close contact was one of the main modes of transmission of COVID-19. 12 -14 Five patients denied a history of travel in Wuhan City or contact with other infected people, so other transmission routes may be possible, which merits further epidemiologic investigation. 15,16
The symptoms of COVID-19 are mainly fever, cough, and dry cough; some patients produce a small amount of mucus and sputum. All patients in our study had a fever, 83.33% had cough symptoms, 33.33% had chest tightness and dyspnea, and 25% had fatigue and muscle pain; but sore throats, headaches, and diarrhea were relatively uncommon. These data align with results reported by Nanshan et al 17 except for fatigue and muscle pain (which may be related to case selection). In general, the viremia elicited by viral pneumonia can cause fatigue and muscle pains. The laboratory tests in our study showed normal/low counts for WBCs and neutrophils and a decreased number of lymphocytes, which is consistent with the general features of viral infections. 18
Computed tomography can be used to evaluate the manifestations, extent, and complications of COVID-19. 19 At the first visit, patients were at a different disease stage, had different comorbidities, immunologic status, and imaging findings. 20 We analyzed the CT findings and dynamic changes in CT images and noted 3 main features.
First, COVID-19 led to multiple lesions in multiple lobes; it was rarely involved in a single lesion or single lobe. These findings are different from the manifestations of bacterial pneumonia, which affects the lower and middle lung lobes. In the early and progressive stages of COVID-19, lesions were distributed mainly along the peribronchovascular bundle and subpleural region. These features may have been due to the invasive nature of COVID-19, which was involved directly with the terminal bronchioles and surrounding alveolar structures after inhalation through the upper respiratory tract. As pneumonia progressed, the lesion spread from the periphery to the hilum. Lesion distribution and trend of spread are important characteristics of COVID-19.
Second, CT of the chest revealed COVID-19 to manifest typically as diffuse, patchy GGO with a clear boundary. Ground-glass opacity formation was due mainly to congestive edema and swelling of interstitial alveolar walls at the early stage of COVID-19. There was no/slight exudation in alveoli, which was related to incomplete alveolar filling. As COVID-19 progressed, the density of the ground-glass shadow increased, and small grid-like changes were seen in the lesion, which was related to thickening of the interlobular space caused by interstitial edema. Ground-glass opacity with a small grid within the lesion could be used as a characteristic manifestation of COVID-19 in the early and progressive stages of COVID-19. With further development of pneumonia, CT showed partial consolidation with surrounding GGO, and the edges of the surrounding GGO were usually blurred, which may have been related to an increase of serous cellulose exudates in alveoli.
Third, CT showed thickening and dilatation of the endobronchial wall of the lesion. We postulate that this feature was related to the inflammatory response caused by COVID-19 invading the bronchus and inflammatory fibrosis in the lesion. Computed tomography also showed widening of pulmonary-vessel diameters in the lesion area, which was considered to be due to the increased oxygen exchange in blood caused by virus damage to the stroma and parenchyma of the lung. During recovery, cord-like shadows were seen in some patients, which suggested lesions infiltrating along lung interstices. Pleural thickening/adhesion was not observed. In 1 patient with severe COVID-19, pleural effusions may have been related to inflammation involving the pleura and causing inflammatory exudation. Mediastinal or hilar lymphadenopathy was not observed in any patient.
The CT findings of COVID-19 overlapped with those of other types of viral pneumonia, organic pneumonia, and eosinophilic pneumonia, so distinguishing between them was difficult. Combining the CT findings with the place of residence, contact history, first symptoms, and laboratory examination is helpful for the differential diagnosis. 21
Because of the small sample size, the correlation between clinical manifestations, laboratory examinations, and CT findings could not be analyzed statistically. Also, the short course of COVID-19-induced pneumonia meant that the prognosis could not be analyzed further.
Conclusions
Coronavirus disease 2019 has certain clinical characteristics and typical CT features, with the latter being particularly important.
Footnotes
Authors’ Note
Both Bingkun Jie and Xiaojin Liu contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was granted from Shandong Medical and Health Science Technology Development Project (2018WSA14002), ShanDong health science and technology association science and technology project (no.SDBJKT20180086), and ShanDong province traditional Chinese medicine science and technology development plan project (no.2019-0872).