
Abstract
Penetrating neck injury can have potentially devastating consequences due to the many vital structures contained within the neck. In patients who do not require immediate surgery, computed tomography angiography of the neck is the test of choice to characterize the injury. A systematic approach to assessment will ensure a thorough evaluation and give the reporting radiologist the best chance of identifying the significant findings, which can often be subtle. Clear communication with the trauma team at both the time of request and after the imaging has been evaluated to relay any significant findings is vital to ensure the best outcome for the patient.
Background
The number of offences in England and Wales involving a knife or sharp instrument has risen consistently over the last four years and is now at its highest recorded level, with 40,147 cases in the year ending March 2018 (1). This has been reflected by data extracted from the Trauma Audit and Research Network (TARN) database for this article, showing a 29% increase in cases of penetrating neck injury over the past five years. Clinicians and radiologists will be exposed to an increasing number of patients who have sustained penetrating neck injuries and this paper is aimed at providing a framework to approaching the imaging studies based on our experience at a level I trauma unit in London.
Penetrating neck injury is defined as an injury that breaches the platysma and is seen in approximately 10% of trauma patients (2–5). The neck contains many vital structures, including the upper aerodigestive tract, neck vessels, cervical spine, cervical spinal cord, peripheral nerves, and brachial plexus, all of which can be injured during penetrating trauma. The injury can be caused by a variety of different weapons including knives and sharp objects as well projectiles including bullets. Patients presenting with penetrating neck trauma have a relatively high mortality, with published data showing rates in the range of 2%–10% due to airway compromise, exsanguination, stroke, sepsis, or cervical spine injury (6–9).
Patients presenting with penetrating neck injury were traditionally assessed using a zonal approach, which involves dividing the neck into zone 1 (clavicles to cricoid cartilage), zone 2 (cricoid cartilage to angle of the mandible), and zone 3 (angle of the mandible to skull base). Neck exploration was advised for all patients who had a zone 2 injury (6), while zone 1 and 3 injuries were generally managed conservatively (10) unless they were unstable due to the difficulty in surgical access to these regions (3). A wide range of investigations including catheter angiography, endoscopy (nasolaryngoscopy, bronchoscopy, and esophagogastroduodenoscopy), and fluoroscopic evaluation of the esophagus was used to evaluate zone 1 and 3 injuries depending on the nature of the trauma and clinical suspicion of the structures are involved (7). Use of the zonal approach resulted in high rates of negative neck exploration (50%–60%) for zone 2 injuries (6,7). A further limitation is that internal injuries are often located in a different zone to the external wound and 16% of patients have an injury in more than one zone; therefore, important injuries could be overlooked (9,11).
Subsequently a more selective method was developed based on the zonal approach of injury, clinical findings, and investigations to select which patients required surgical exploration in an attempt to reduce the rate of negative neck exploration (5). Moreover, a “no zone” approach has been proposed that is associated with better patient outcomes and has reduced unnecessary neck exploration in certain studies (2,7). Using a “no zone” approach, patients demonstrating “hard” signs of a significant injury are taken directly to theatre for exploration of the wound. The exact definition of what constitutes a “hard” sign varies among different guidelines and institutions, but they typically include airway compromise, expanding hematoma, absent pulses, vascular thrill, shock, evidence of active bleeding, massive hematemesis/hemoptysis, neurological deficit including stroke, massive surgical emphysema, or air bubbling through the wound (5,7,10,12).
Patients who do not require immediate surgical management but have “soft” clinical signs of an injury—including minor bleeding, non-expanding hematoma, minor hemoptysis/hematemesis, dysphagia, or vocal changes—should be assessed with a multidetector computed tomography angiogram (MDCTA) of the neck (12,13). Imaging of asymptomatic patients has not been established, with recent publications proposing that completely asymptomatic patients do not require imaging (12,13). This decision requires a high level of clinical confidence and is subject to a number of factors including experience of managing patients with penetrating neck injury; therefore, MDCTA for all patients with a penetrating neck injury that do not require emergency surgery has been recommended (2).
MDCTA allows rapid, non-invasive assessment of both vascular and non-vascular injuries and can guide the need for further investigations such as endoscopy, catheter angiography, or magnetic resonance imaging (MRI) as well as identifying injuries that require surgical management (6). MDCTA has been shown to have a sensitivity and specificity of >97% for identification of significant injuries and use of a no zone approach can reduce the number of negative neck explorations (5,14).
Imaging protocol
MDCTA is the imaging modality of choice in our institution for assessment of traumatic neck injuries. The CT protocol utilized ideally requires an 18-gauge cannula in the antecubital fossa. It is preferable to cannulate the patient contralateral to a potential site of neck injury given the potential artefact created by the contrast within the supraclavicular fossa that can limit image interpretation. A pre-monitoring slice positioned with a region of interest (ROI) over the arch of the aorta and 50 mL of Omnipaque 300 and 50 mL saline are injected at a rate of 4.5 mL/s with an automatic trigger when the ROI reaches 100 HU; 120 kV and 110 mAs with both Care Dose and Care kV are used with 128 × 0.6 mm collimation. Multiplanar reformats are produced at the time of imaging and can be created and manipulated in PACS at the time of reporting.
Approach to CT interpretation
When reporting cases of penetrating neck injury, it is important to have a structured approach to image interpretation in order to identify significant findings that will impact management in a time critical situation (Table 1). This is particularly important in mass casualty situations where there could be a high throughput of cases.
Penetrating neck trauma checklist.

UADT, upper aerodigestive tract.
Communication between the reporting radiologist and trauma team is vital. A clear description of the location and number of external wounds, as well as a description of the object that inflicted the injury, the trajectory of the wound, and presumed depth is crucial to aid interpretation. The cutaneous defect can be difficult to identify on CT, especially when the entry wound is small as it may seal; skin markers can be useful in this regard. The imaging should be carefully interrogated for small locules of subcutaneous gas (using lung windows), stranding of the subcutaneous fat and hematoma. In difficult cases, three-dimensional rendering with co-location on to the two-dimensional imaging can be useful. Deeper locules of gas and hematoma allow assessment of the wound trajectory and depth, as well as indicating which compartments have been breached. This is further complicated by penetrating trauma secondary to missiles (e.g. gunshot wounds) as tissue damage can occur secondary to a direct effect from the missile as well as dissipation of energy into the surrounding tissues with the potential for temporary cavitation (10). As such, radiological assessment extends beyond the wound trajectory to evaluate the surrounding soft tissues in these circumstances, which can be challenging given potential artefact from metallic foreign bodies.
In our institution, we advocate an ABCDE approach to systematically evaluate the structures of the neck for injury. AB (airway and breathing) refers to assessment of the aerodigestive tract, C (circulation) refers to assessment of the vasculature, D (disability) involves assessment for neurological injury, and E (everything else) is a review of the other structures in the neck including the salivary glands, thyroid gland, and cervical esophagus.
Airway and breathing
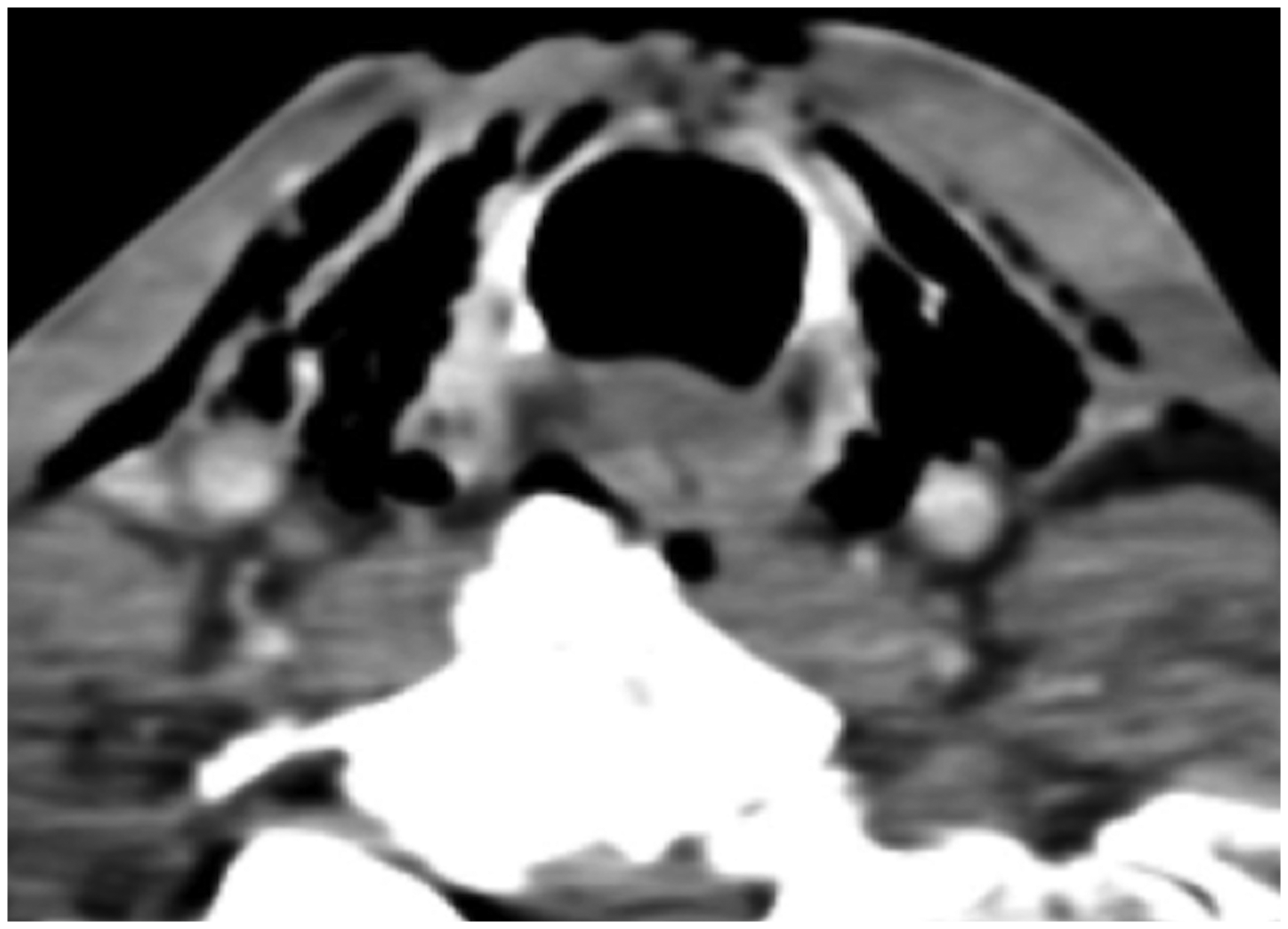
Aerodigestive tract injury occurs in 5%–7% of patients with penetrating neck injury (15). The upper aerodigestive tract should be assessed for any evidence of breach using both soft tissue and lung windows. In some patients, a defect in the wall can be identified, confirming aerodigestive tract injury (Fig. 1); however, if the defect is small, it may not be visualized on CT. Furthermore, with more extensive soft-tissue lacerations the defect may not be apparent on imaging if the injured tissue surfaces are apposed; therefore, the radiologist is reliant on accurate clinical information. If the trajectory of the wound breeches either the suprahyoid deep neck spaces or the infrahyoid visceral space (sensitivity = 97%, specificity = 55%), further investigation should take place with either endoscopy or targeted exploration (Fig. 2) (15). In some cases, deep surgical emphysema may be the only clue of a breach of the inner mucosal surface and should prompt further investigation. The absence of deep surgical emphysema has a high negative predictive value (98.9%) and therefore some authors argue its absence can be used to almost completely exclude a significant aerodigestive tract injury (16).

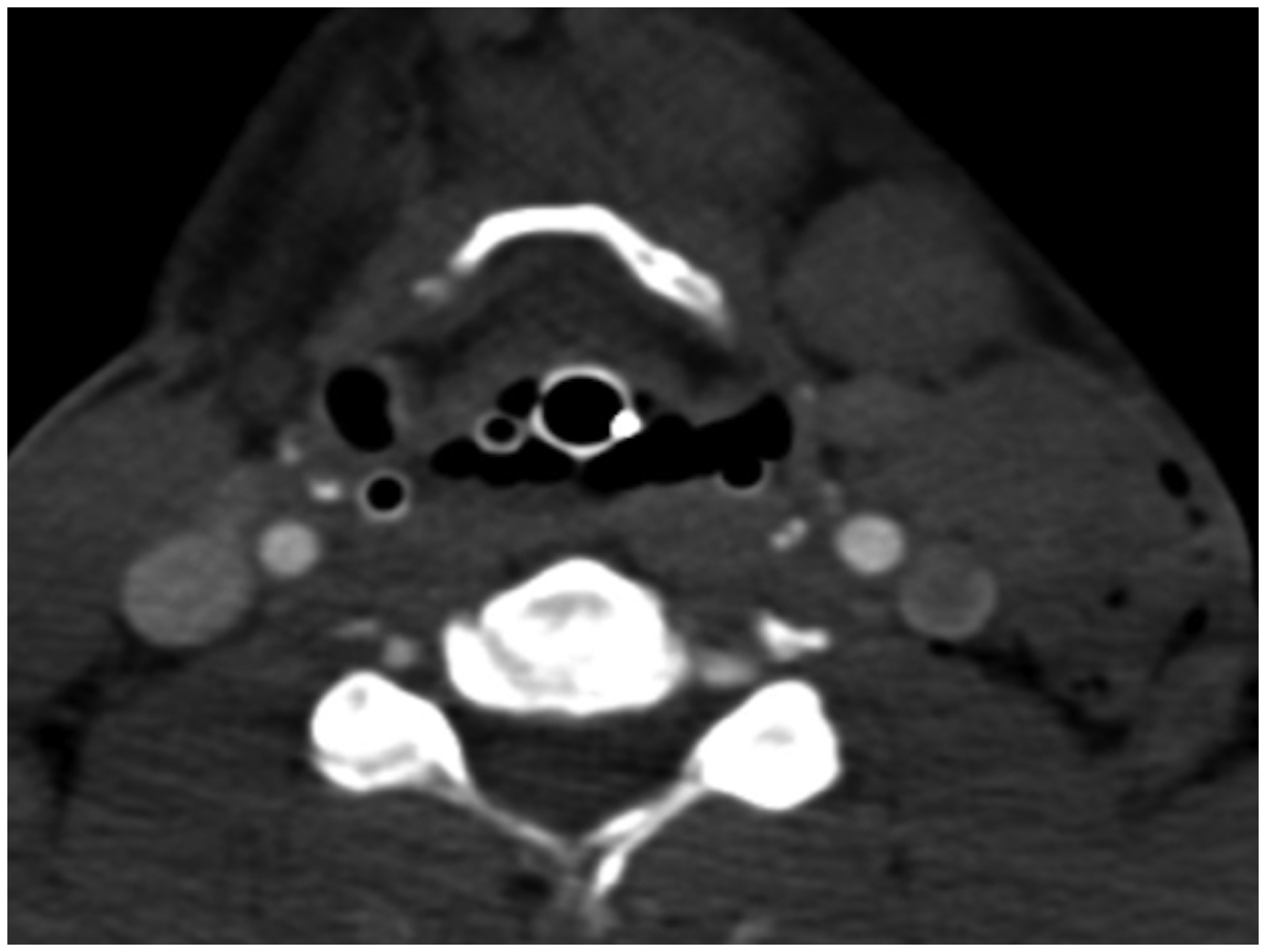
Axial computed tomography image of the inferior neck of a patient who presented with a penetrating wound to the anterior neck. There is defect in the trachea visible anterior to the endotracheal tube tip, deep surgical emphysema, and pneumomediastinum.
Axial computed tomography image of the neck of a patient who presented with a slash wound. There is a large soft-tissue defect anteriorly with the impression of a tracheal defect and deep surgical emphysema. No pneumothorax is visible and therefore even in the absence of a definite tracheal defect the features are highly suspicious of aerodigestive tract injury. A tracheal injury was confirmed in theatre.
The lung apices will be included and should be assessed for pneumothorax. This can be a confounding factor for identification of aerodigestive tract injury as gas tracking superiorly along fascial planes from a pneumothorax causes an appearance that is often indistinguishable from deep surgical emphysema due to an injury of the aerodigestive tract.
If a tracheal injury is identified the level should be given in the report with regard to the corresponding cartilaginous ring. The larynx should be assessed for any evidence of a laryngeal fracture and if one is identified, there should be a comment as to whether it is displaced. Hematomas should be evaluated for evidence of active bleeding as well as compressive effect and if there is any evidence of airway compression or distortion the clinical team should be urgently contacted and warned of possible airway compromise (Fig. 3).

Axial and sagittal computed tomography images of a patient who was stabbed in the neck demonstrate a large suprahyoid hematoma extending to the tongue base and completely effacing the airway.
Circulation
Arterial injury is identified in approximately 25% of cases and carotid artery involvement is twice as common as vertebral artery injury (2,7). MDCTA has been shown to be both sensitive (94.4%) and specific (96.7%) in identification of vascular injury (16). Assessment for arterial injury should be performed in a systematic manner beginning with the aortic arch followed by close interrogation of the carotid and vertebral arteries and their branches. Findings of arterial injury include extraluminal blush of contrast in active bleeding (Figs. 4 and 5), pseudoaneurysm formation, arteriovenous fistula formation, evidence of dissection including direct visualization of a dissection flap (Fig. 6), vessel wall irregularity, and vessel occlusion (Fig. 7). Given the imaging acquisition within the arterial phase in our institution, abnormal early venous enhancement can identify arteriovenous fistula formation that can present both as an early or late complication. It is important to report any evidence of carotid sheath breach, even when an underlying vascular injury is not demonstrated.

Axial computed tomography image of a patient presenting with a single right supraclavicular stab wound and significant blood loss demonstrates active extravasation from the right common carotid artery and a large hematoma causing shift of the trachea to the left.
Axial computed tomography image of a patient who presented with a self-inflicted neck laceration demonstrates a large anterior neck wound with deep extension. There is active extravasation from the right lingual artery, which is pooling in the airway, which therefore must also be breeched.
Axial computed tomography imaging of a patient after an industrial accident demonstrates a left-sided laceration, fracture of the left mandible, and traumatic dissection of the left internal carotid artery.
Axial and sagittal computed tomography imaging of a patient with a single left lateral wound demonstrates a left lateral penetrating injury with a subcutaneous hematoma which contains the subjacent left vertebral artery tapers and is occluded as it passes through the left C1 foramen transversarium consistent with vertebral artery dissection.
MDCTA is optimized for arterial opacification and therefore venous opacification is not reliable. Findings suggesting a venous injury include locules of gas within or in close proximity to a vein (Fig. 8), venous thrombosis (Fig 9), perivenous hematoma or fat stranding, and the trajectory of the injury passing through or in close proximity to a vein (Fig. 10).

Axial computed tomography imaging demonstrates subcutaneous locules of gas in the left supraclavicular region with gas in the venous system including the left internal jugular vein. This is contralateral to the injection site and suggests venous breech.
Axial computed tomography imaging of a patient who was stabbed in the left side of the neck shows the left internal jugular vein is poorly opacified adjacent to the injury raising the suspicion of a venous injury. There is a nasogastric tube is incorrectly sited as it is coiled next to the endotracheal tube.

Axial soft tissue and lung window computed tomography images demonstrate a wood density foreign body (a chopstick) in situ with the tip in the region of the retropharynx. The foreign body lies in the expected path of the right internal jugular vein. There is no hematoma implying compression rather than penetration of the vein; however, this requires surgical exploration.
Disability
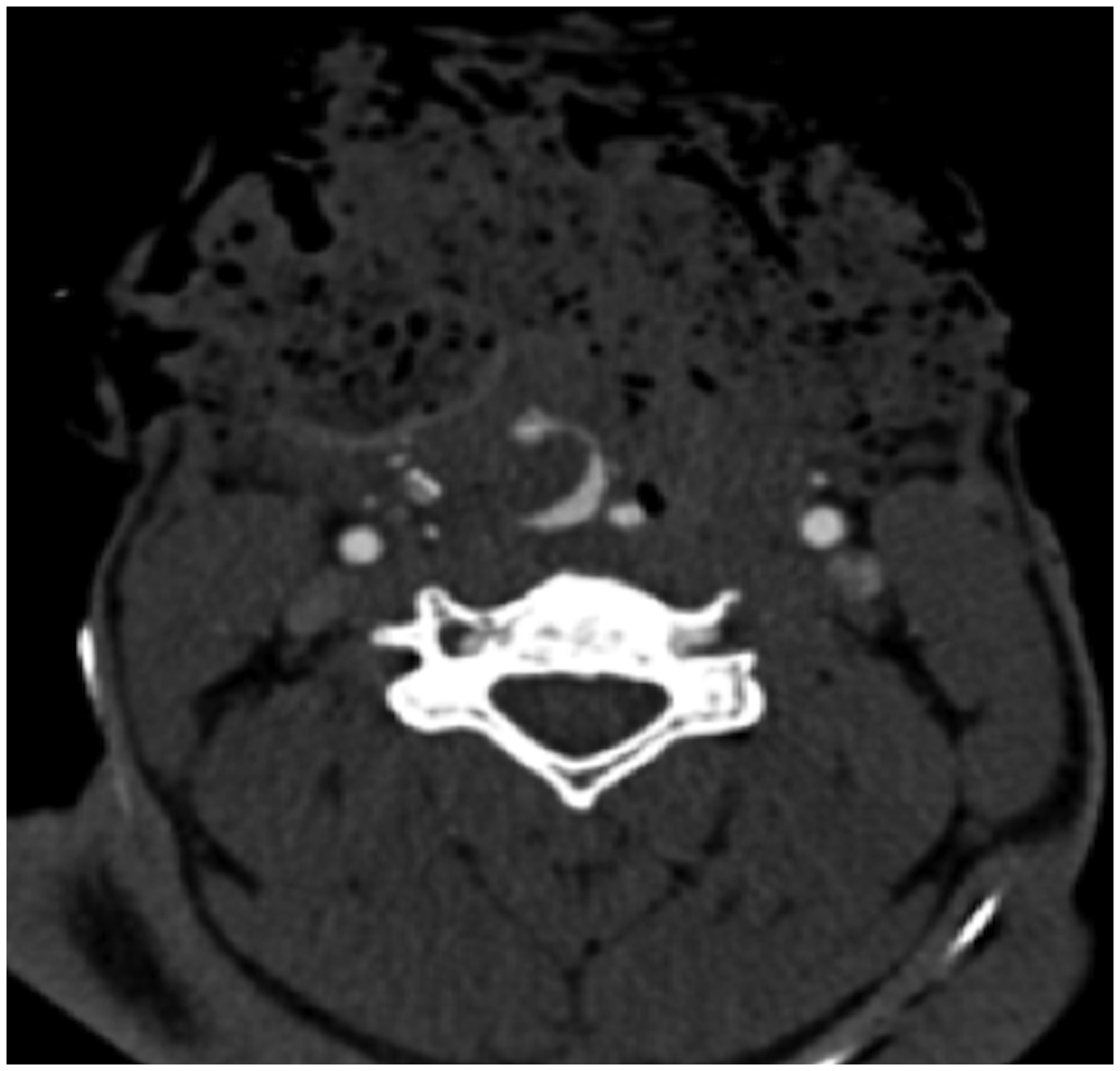
Penetrating neck injuries can potentially cause central or peripheral neurological injury, although spinal cord injuries are rare and seen in <1% of cases (13). The spinal canal should be assessed for gas or hematoma which would suggest dural breach (Fig. 11). The perivertebral space and course of the brachial plexus should be closely interrogated to assess for potential peripheral nerve injury. If a neurological injury is suspected, this should be correlated clinically and MRI can be performed for further characterization.
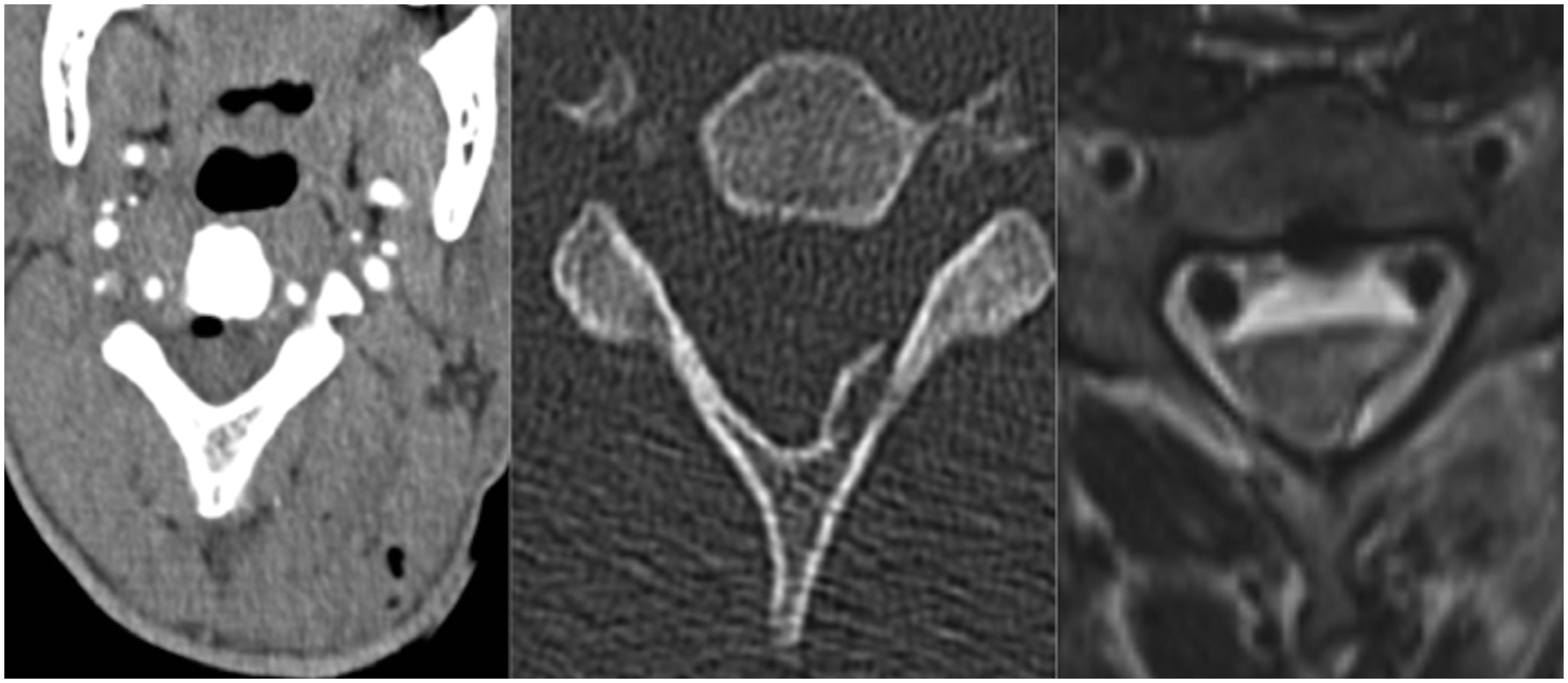
Axial CT images of a patient who was stabbed in the left posterior neck demonstrate subcutaneous and intramusclular locules of gas along the trajectory of the wound which is in the direction of the cervical spine. There are locules of gas in the spinal canal consistent with extension of the wound into the spinal canal and raise the possibility of a cord injury (left). A fracture of the left C4 lamina is demonstrated on the bone reconstructions (middle). T2-weighted MRI (right) shows high signal in the left cord consistent with a cord injury, shallow anterior epidural hematoma and paraspinal hematoma. There is also susceptibility artefact at the posterior margin of the vertebral body in keeping with a retained metallic foreign body which could not be appreciated on CT. CT, computed tomography; MRI, magnetic resonance imaging.
Certain injuries should prompt clinical assessment for a nerve injury, particularly the extracranial course of the lower cranial nerves. The facial nerve can be injured in soft-tissue injuries and lacerations involving the parotid and submandibular glands. The glossopharyngeal, vagus, and accessory nerves can be compromised by hematomas causing compression at the jugular foramen and below the skull base. The vagus nerve can also be compromised in carotid sheath injury and the accessory nerve can be injured by lacerations in the posterior triangle. The hypoglossal nerve can be compromised by fractures involving the hypoglossal foramen or hyoid bone.
Everything else
Esophageal injuries are associated with a high mortality of 20%, which is thought to be partly related to delayed diagnosis (10). They can be difficult to identify on CT and often the only finding is the presence of pneumomediastinum. There should be a high index of suspicion if esophageal injury is suspected based on the wound location and suspected trajectory with a low threshold for further imaging with either a CT with oral contrast (on the table directly before acquisition) or fluoroscopy. Furthermore, potential fistula formation between the trachea and esophagus or vessels and esophagus are rare but easily overlooked. In the case of carotid-esophageal fistula this can be identified if there is abnormal luminal contrast extravasation whereas trachea-esophageal fistula formation can be identified on contrast-based examinations as described although are more readily identified with direct visualization (17). These can present acutely but delayed presentations are also recognized (18).
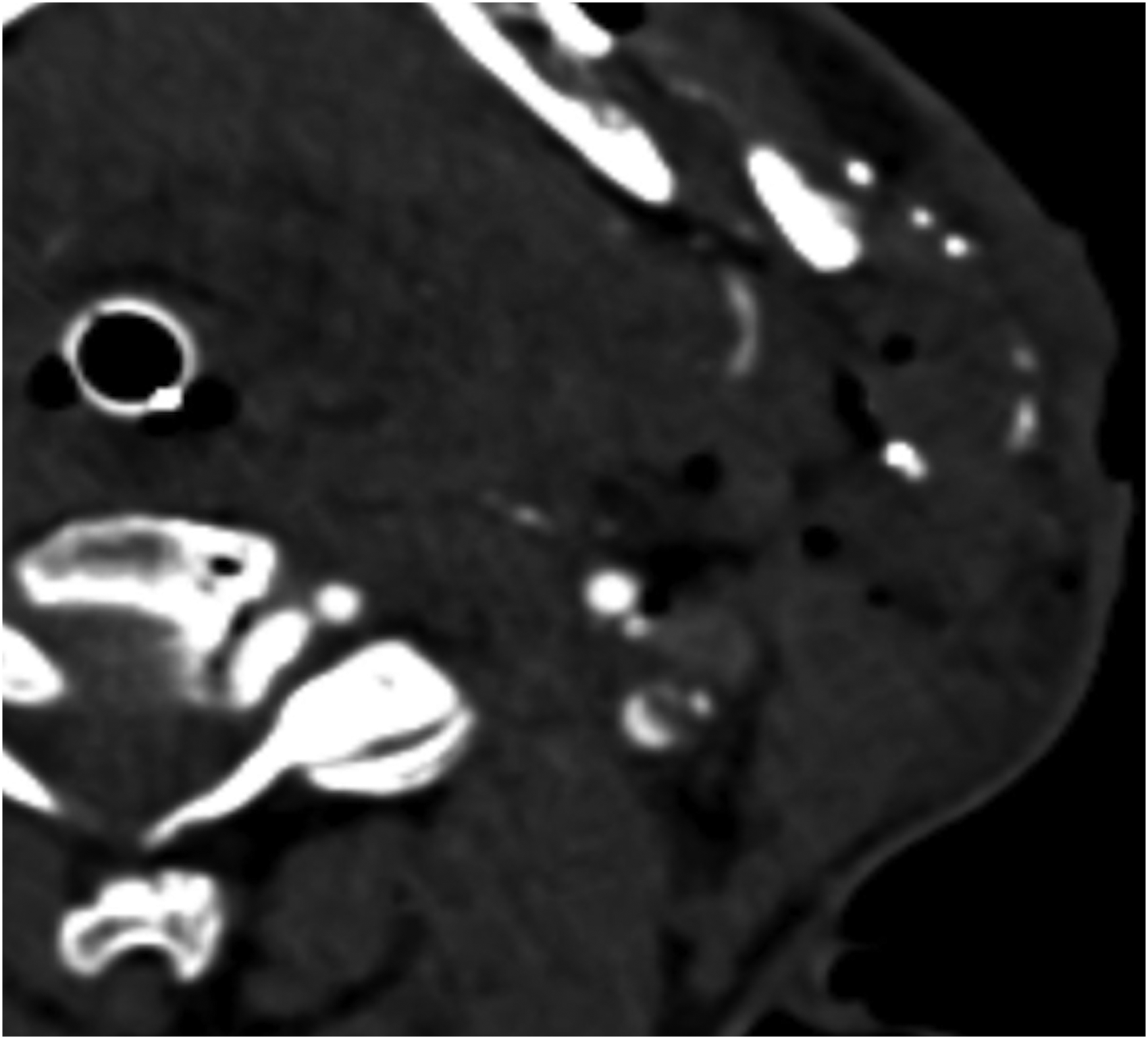
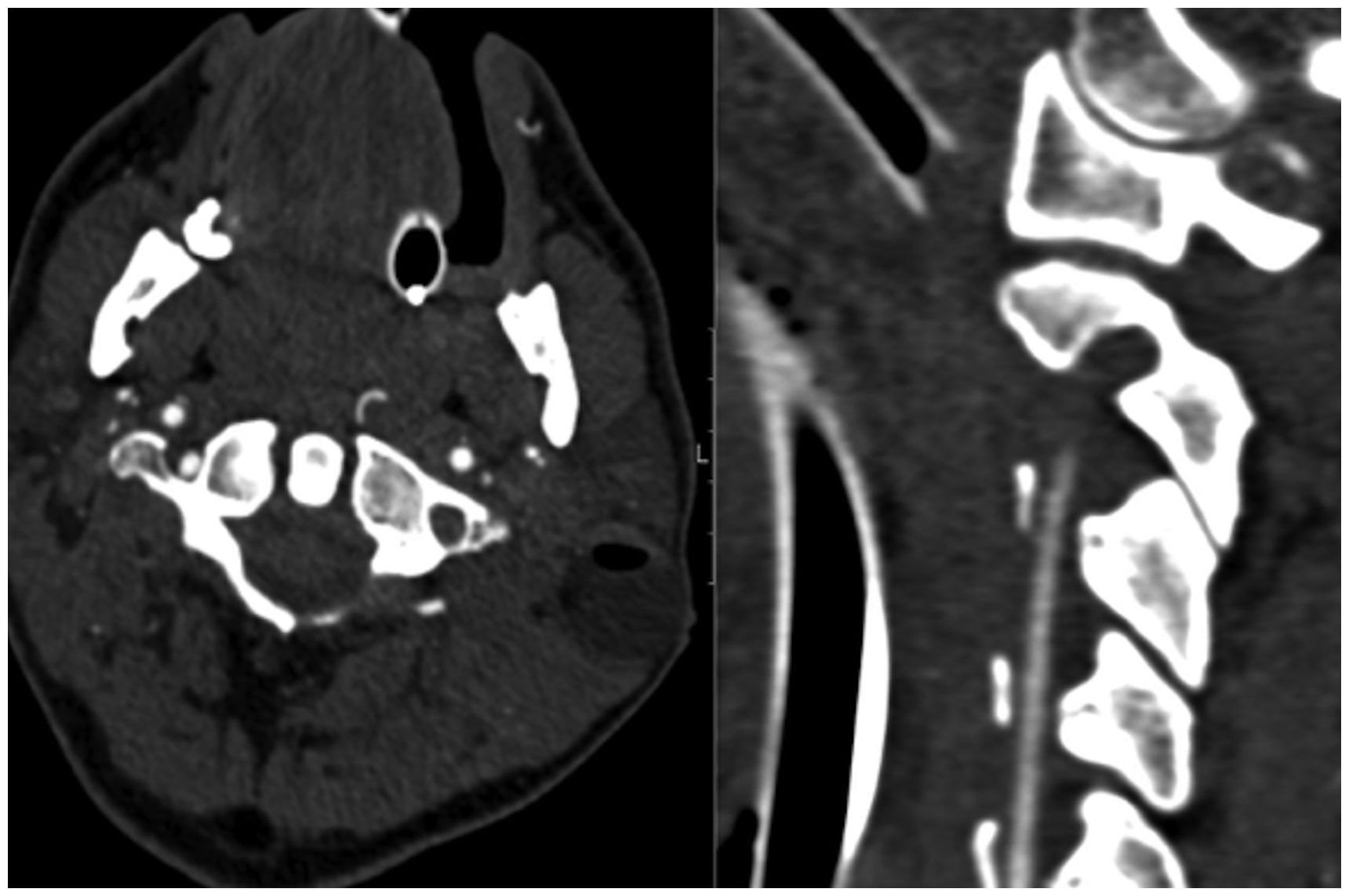
The salivary glands and thyroid should be assessed for evidence of injury, which can include laceration and hematoma (Figs. 12 and 13). The skull base, facial bones, cervical and upper thoracic spine, and some of the shoulder girdle will be included on the study and should be interrogated for any fractures. Spinal injuries are identified in 11%–14% of cases (Fig. 14) (7). Finally, the neck muscles should be reviewed for any evidence of injury (Fig. 15) with a particular focus on the scalene musculature given their important anatomical relationships. The brachial plexus and subclavian artery pass between the anterior and middle scalenes, while the phrenic nerve pass anteriorly to the anterior scalene muscle as the muscle crosses over the first rib. If radiopaque foreign bodies are identified, their location should be described in the report.

Axial computed tomography image of a patient who presented with a neck stab wound demonstrates transection of the left lobe of the thyroid. There is extensive surgical emphysema including gas within the carotid sheath.

Serial computed tomography images after a left parotid injury. Images from the index scan (bone window top left, soft tissue window top right) show a fracture of the left mandibular ramus and soft tissue injury. Due to increased swelling a repeat study (bottom left) was performed which shows hematoma in the left parotid gland. A second repeat study five days after the index scan (bottom right) shows development of a pseudoaneurysm.

Axial computed tomography soft-tissue window and sagittal bone window images of a patient who was stabbed in the neck demonstrates a significant anterior midline neck wound with extensive surgical emphysema. There is a fracture of the anterior T4 vertebral body showing the wound extended inferiorly into the mediastinum.

Axial computed tomography image of a patient who has been stabbed in the neck demonstrates a hematoma in the left sternocleidomastoid is compressing the left internal jugular vein.
Conclusion
Penetrating neck injury can have potentially devastating consequences due to the many vital structures contained within the neck. In patients who do not require immediate surgery, CTA of the neck is the test of choice to characterize the injury. A systematic approach to assessment will ensure a thorough evaluation and give the reporting radiologist the best chance of identifying the significant findings, which can often be subtle. Clear communication with the trauma team at both the time of request and after the imaging has been evaluated to relay any significant findings is vital to ensure the best outcome for the patient.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.