
Abstract
Background
Penetrating trauma is rarely encountered in Nordic trauma centers, yet the incidence is increasing. Typical imaging findings in penetrating trauma should thus be familiar to all radiologists.
Purpose
To evaluate incidence and imaging findings of penetrating chest trauma, gunshot wound (GSW) and stab wound (SW) injury spectrum, imaging protocols, and outcome in a large trauma center.
Material and Methods
Trauma registry data from 2013–2016 was retrieved, and imaging accessed through hospital PACS. Retrieved variables included age, gender, injury severity scores, mechanism of injury, time to CT, and 30-day mortality. Depth of thoracic, pulmonary, abdominal and skeletal injury, active bleeding, and use of chest tubes were evaluated.
Results
Of 636 patients with penetrating injuries, 443 (69.7%) underwent imaging. Of these, 161 (36.3%) had penetrating thoracic injuries. Of 161 patients with penetrating chest trauma in imaging, 151 (93.8%) were men (mean age = 34.9 years) and 10 (6.2%) were women (mean age = 40.7 years). The majority of patients had SWs (138 SW vs. 15 GSW). Patients with GSWs were more severely injured (mean ISS 17.00 vs. 8.84 [P=0.0014] and ISS≥16 in 53.3% vs. 16.7%) than SW patients. In CT, intrathoracic injuries were found in 49.4% (77/156) and active bleeding in 26.3% (41/156). Emergency surgery was performed in 6.2% (10/161) with postoperative CT imaging. Thirty-day mortality rate was 1.2% (2/161).
Conclusion
Penetrating thoracic trauma often violates intrathoracic structures and nearby compartments. Arterial phase whole-body CT is recommended as multiple injuries and active bleeding are common. CT after emergency surgery is warranted, especially to assess injuries outside the surgical field.
Keywords
Introduction
The majority of severe civilian trauma in Europe is due to blunt traumatic injury, whereas in the United States gunshot wounds (GSW) are often encountered (1). In Finland and Norway, for example, penetrating trauma is not very commonly seen—an estimate of 5%–10% of all injuries in large trauma centers (2–4). Stab injuries are relatively rare in most European countries, but are common in international conflicts, terrorist attacks, and in large city hospitals around the world (5–7). The encountered penetrating injuries in Scandinavian countries are mostly due to stab wounds (SW). Gunshot injuries are rare compared to countries that allow liberal access to firearms (e.g. the United States). However, in recent years, Sweden has encountered an increase in firearm-related trauma (8). Interpretation of imaging studies in penetrating trauma requires knowledge of the injury mechanism and experience of imaging characteristics in GSWs and SWs. The penetrating instrument and the force of impact differ greatly between firearm injuries and stabbings resulting in vast trauma energy variation. Extent of injury also depends on the affected tissue type (9–11).
Today, we face an increasing risk of terroristic acts. Terrorist stabbings are reported to result in more severe an injury pattern than civilian stabbings, due to the solid intent of injuring as many victims as severely as possible (5). In addition, improvised explosive devices lead to mass casualties with a preponderance of penetrating injuries. Explosion injury is a mixture of blast and penetrating injury that inflicts a large number of victims simultaneously and causes traumatic changes in multiple body regions (12). This imposes emergency care providers to a surge of patients and a sudden need of diagnostic and surgical resources that should be allocated in a premeditated manner. Radiology provides a tool for accurate triage assessment in revealing potential cases of over triage (falsely higher triage category) and under triage (falsely lower triage category). Over triage has been shown to increase mortality (13). Assessment of several potentially critically injured patients in a short timeframe and the rarity and unique patterns of these injuries pose a challenge to the radiologist on-call (13–15). Radiologists should also guide clinicians in choosing the right imaging method and in distinguishing when conventional angiography is needed instead of computed tomography angiography (CTA).
Unstable patients often undergo emergency surgery (damage control surgery) with no preoperative imaging. An increasing interest has been paid to those patients that would—after emergency thoracotomy or laparotomy—benefit from a postoperative chest–abdominopelvic CT. The purpose is to identify unexpected injuries and to confirm suspected injuries that were not fully explored in surgery. A recent study (16) showed a fair number (19/90; 21%) of such patients with additional injuries within the surgical field, that were not identified during laparotomy. Moreover, 8 (8.9%) patients had unexpected injuries at CT that were substantial enough to warrant additional surgery or angiography. These preliminary results emphasize the potential importance of routine postoperative CT in these patients. In another study from a large trauma center, 9% of patients with penetrating chest trauma underwent emergency surgery (17). The most common cause for emergency surgery was cardiac injury with < 25% of patients injured to the heart reaching the hospital alive. However, 90% of the acutely operated patients survived. Postoperative imaging was not reported (17).
The main aim of this retrospective study was to describe the spectrum of penetrating trauma that underwent imaging, as well as critically evaluate the current imaging practice and diagnostic performance in a large level 1 trauma center with a catchment area of about 2.5 million people. The second aim was to identify those patients that underwent a CT examination after emergency thoracotomy or laparotomy and to evaluate the potential benefit of postoperative CT imaging. Increased diagnostic accuracy and streamlined imaging protocols in penetrating injuries have a direct impact on patient care, eventually leading to improved outcome, quality of life, and substantially decreased healthcare costs. Third, this retrospective study of imaging penetrating trauma aims to strengthen the radiology department’s preparedness for the worst-case scenario: mass casualties.
Material and Methods
Approval from the Institutional Review Board (IRB) was obtained for this retrospective study. All patients with penetrating trauma during a four-year period (1 January 2013 to 31 December 2016) were identified from the trauma registry database of a large Nordic level 1 trauma center.
The following parameters were retrieved: age; gender; injury Severity Score (ISS); New Injury Severity Score (NISS); mechanism of injury; time from hospital arrival to CT; need for ventilation; and 30-day mortality.
Imaging was performed with two scanners: 16-cm detector Revolution™ multidetector CT (MDCT) scanner (GE Healthcare, Milwaukee, WI, USA) and 64-slice MDCT scanner (LightSpeed VCT, GE Healthcare, Milwaukee, WI, USA). Tube current (and voltage in parentheses) used was 150 mA (100 kV) in the arterial phase and 120 mA (120 kV) in the venous phase of the abdomen. For obese patients, the tube current used was 300 mA (100 kV) and 255 mA (120 kV) respectively. In the thorax + abdomen venous phase studies, the tube current used was 225 mA (120 kV), and for obese patients 300 mA (120 kV). The arterial phase was timed using SmartPrep™ software (GE Healthcare) to secure proper enhancement of the aorta. In studies including arterial phase (incl. time for Smart Prep), venous phase delay was 45 s from the end of arterial phase scanning totaling in a delay of 60–70 s. In venous phase studies, the delay was 65 s. Rotation time was 0.5 s (Revolution CT), 0.4 s (LightSpeed VCT), and pitch 0.992:1 in all protocols.
In the 150 patients imaged with contrast-enhanced imaging, the average amount of administered intravenous contrast material was 109.2 mL (range = 66–200 mL, median = 110 mL). Injection speed in studies including the arterial phase was 4.5–5 mL/s and venous phase 2.5–3.5 mL/s.
The images were retrieved from local picture archiving and communication systems (PACS; SECTRA v. 19.3.11, SECTRA AB, Linköping, Sweden) and reviewed independently by two radiologists (both with five years of experience in radiology) for the following: injured body part and organ; the imaging modality used; the use of oral and/or rectal contrast; mark-up of entry and exit wounds; and the use of vitamin E capsules in wound marking. In addition, the presence of metallic foreign bodies was noted from scout images. CT studies after emergency operations were identified from registry data. Additional information was obtained from exam referral texts and medical records. Diagnostic performance of imaging studies was assessed by accessing the medical records and surgical reports in particular as the reference standard. All injuries, deep and superficial, were included. Data of patients who died before hospital arrival were not available.
A subset of patients with penetrating thoracic injury were reviewed by a third radiologist (with eight years of experience) to evaluate depth of thoracic injury, lung injury, active bleeding, pneumothorax, osseous involvement, and the use and placement of chest tubes. The imaging and characteristics between SW and GSW injuries was compared. The patients with CT studies after emergency surgery were evaluated regarding injuries on both inside and outside the surgical field.
Data were analyzed to determine prevalence of different injury types and to compare imaging findings and characteristics between SWs and GSWs with t-test for parametric and Man–Whitney U test for non-parametric data, and with Fisher’s exact test and odds ratio (OR) with 95% confidence intervals (CI) for dichotomous data. SAS/STAT v.9.4 (SAS Institute Inc., Cary, NC, USA) was used for statistical analyses.
Results
Demographics
A total of 443 patients with imaging for penetrating injuries were found in the trauma registry data, and a subset of 161 (36.3%) patients with penetrating thoracic injuries identified. Of these, 151 (93.8%) of 161 patients were men (age range = 15–90 years, mean age = 34.9 years) and 10 (6.2%) were women (age range = 21–65 years, mean age = 40.7 years). The average ISS was 9.70 (range = 1.00–75.00, SD = 12.23), average NISS was 12.49 (range = 1.00–75.00, SD = 13.65), and mean age was 35.2 years (age range = 15–90 years, SD = 15.95). Comparison of demographic data between SW and GSW patient groups is shown in Table 1.
Comparison of SW and GSW patient groups (demographics).

*P < 0.05.
CI, confidence interval; CT, computed tomography; ED, emergency department; GSW, gunshot wound; ISS, Injury Severity Score; NISS, New Injury Severity Score; OR, odds ratio; SW, stab wound.Statistically significant values are written in bold.
CT was performed in 150 (93.2%) patients on arrival. Five patients (3.3%) had no imaging findings of thoracic trauma in CT examinations. The majority of patients suffered from SWs (138/161; 85.7%) (Figs. 1–5) and the minority from GSWs (15/161; 9.3%) (Figs. 6 and 7). In 8 (5.0%) patients, the mechanism of injury was penetrating foreign bodies (piece of glass, n = 1; pen, n = 1; explosives, n = 2; motor saw, n = 1; impalement, n = 2). A yearly increase in the number of patients with GSWs was detected during the four-year period (Table 2).
Patients per year.

Values are given as n (%).
GSW, gunshot wound; SW, stab wound.

A 53-year-old man. Stab wound posteriorly to right shoulder. Contrast media extravasation (arrow) from an intramuscular vessel in the posterolateral part of deltoid muscle indicates active bleeding.
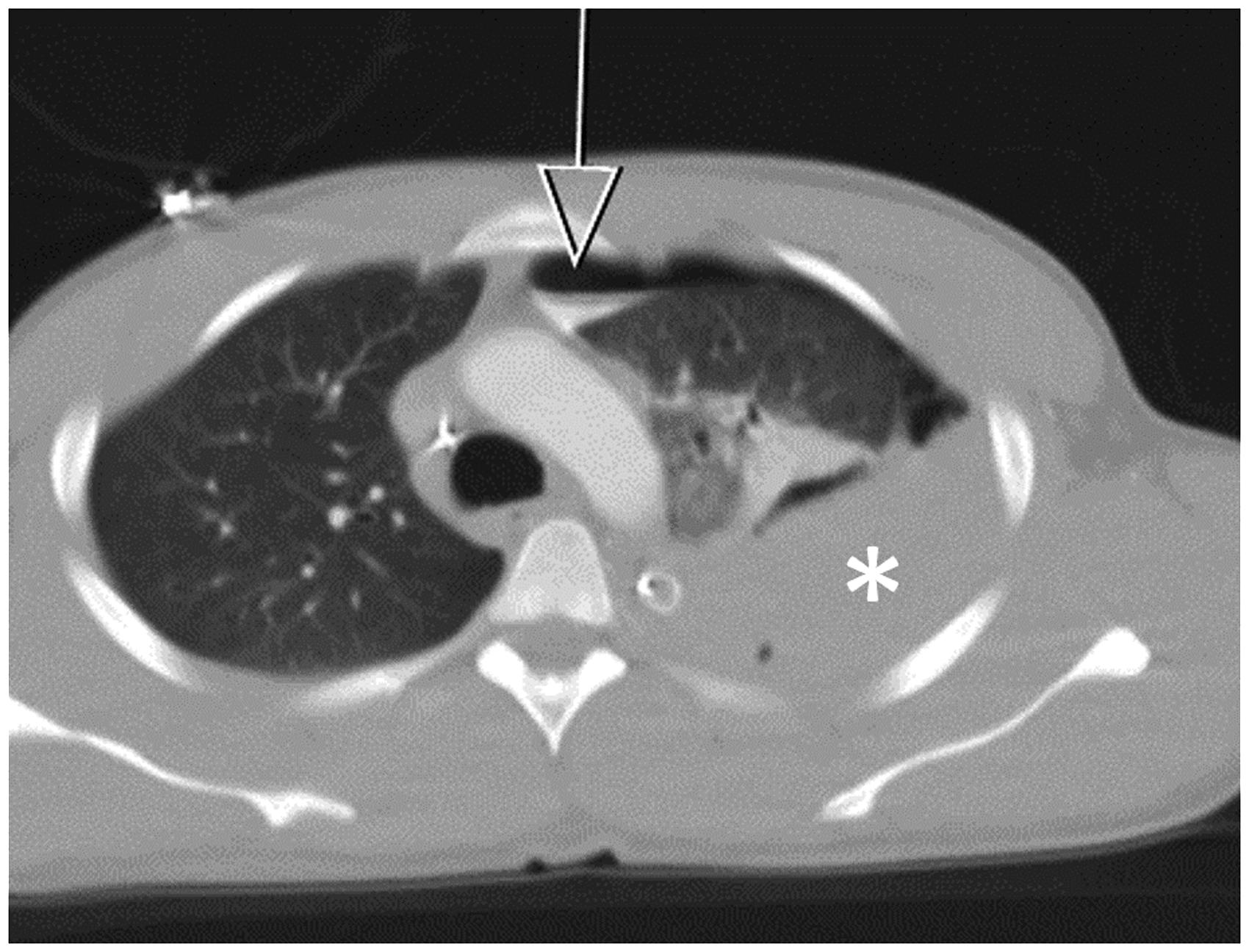
A 22-year-old man. Stab wound to the chest with subsequent hemothorax (asterisk) and pneumothorax with fluid/air interface (arrow). Extravasation of contrast media (arrow) indicates bleeding into pleural space. The bleed was subsequently embolized.

A 21-year-old man. Stab wound to the left anterior chest wall with pneumothorax and pleural injury (arrow).
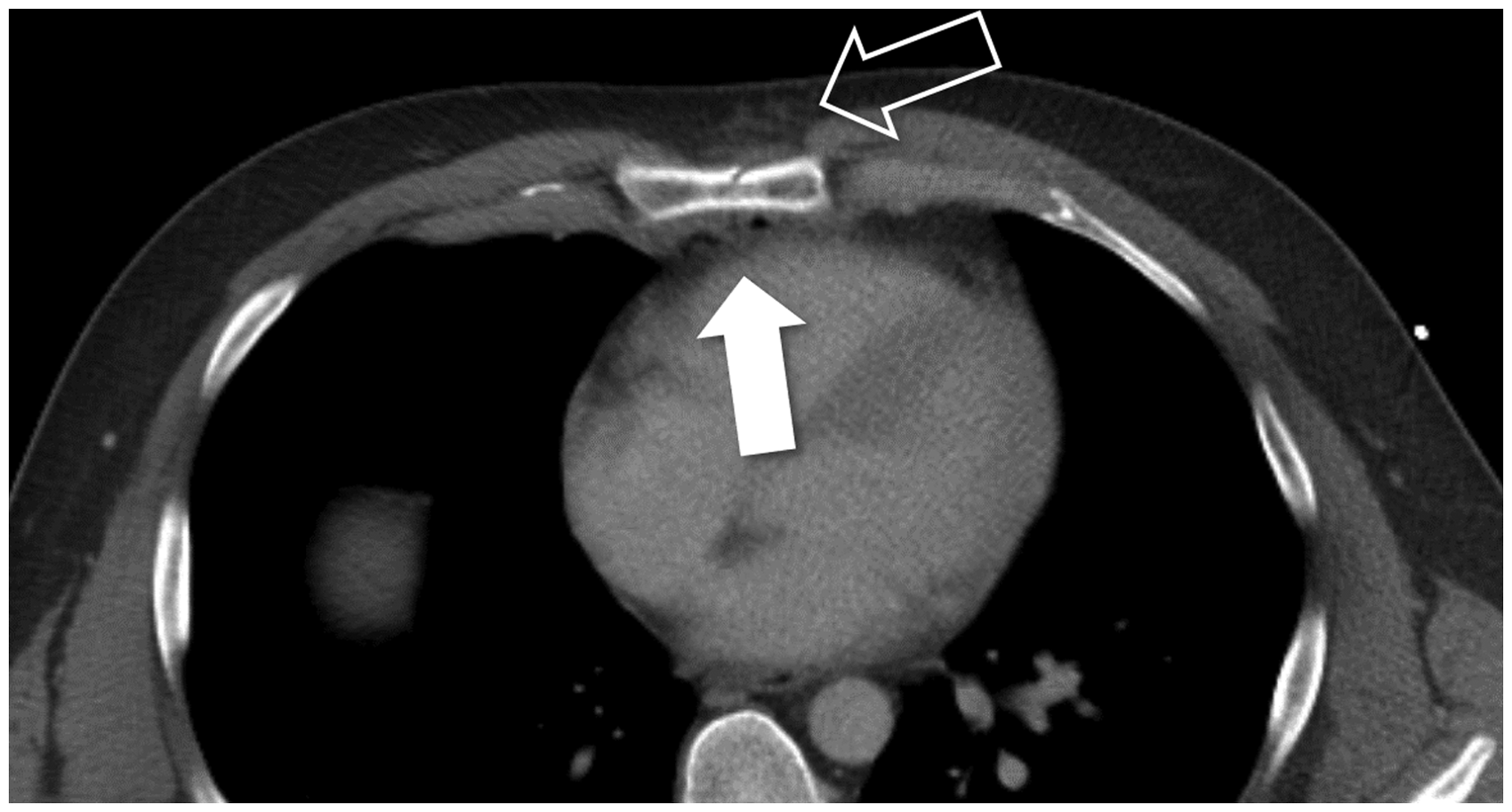
A 32-year-old man. Stab wound through the body of sternum with retrosternal hematoma and air outside the pericardium (white arrow). Wound tract can be followed in soft tissue (hollow arrow). No cardiac injury.
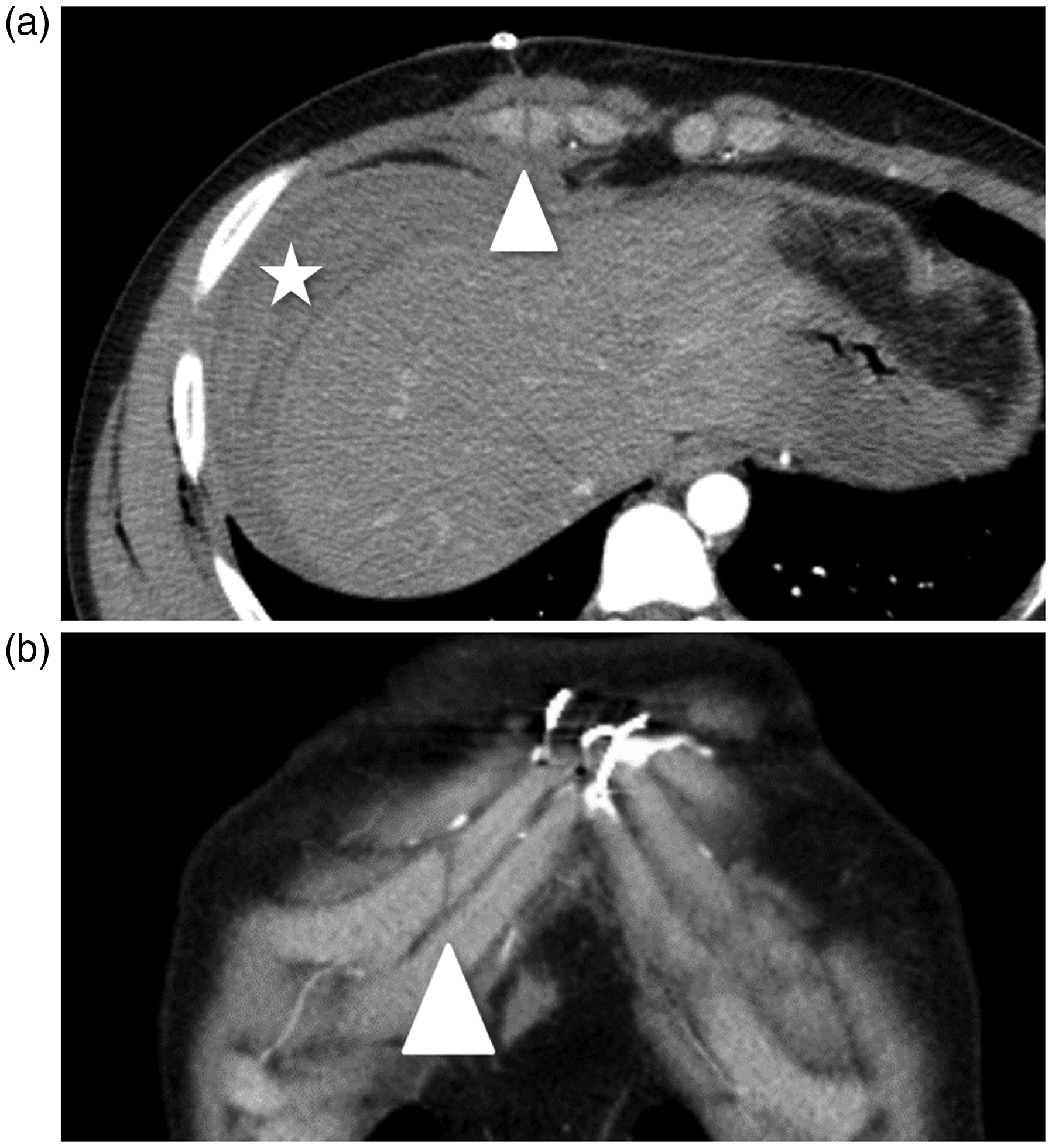
(a, b) A 19-year-old man with multiple stab wounds. Trajectory through the anterior chest wall and costal cartilage (arrowhead) can be seen in axial (a) and coronal (b) plane. Hematoma surrounding the liver (star).

(a–c) A 39-year-old man. Gunshot wound to the thorax with bullet fragment lodged in lung/pleura. No hemo- or pneumothorax. Entry wound is marked with vitamin E capsule (thick arrow) (a). Lateral radiograph shows the shrapnel (arrow) (b). Axial CT image shows the exact location of the shrapnel (c).

(a–c) A 34-year-old man. Gunshot wound, trajectory from jugulum through anterior mediastinum and pericardium (arrow) (a), diagonally through liver (b) and right kidney. Bullet (arrowhead) lodged posterior to right kidney (c). Trajectory through liver and kidney is marked with dashed white lines (b, c).
Injuries
The depth of penetrating trauma ranged from superficial subcutaneous injuries to cardiac tamponade (Table 3). Superficial wounds that penetrated the subcutaneous tissues and muscle (Fig. 1) formed half of all injuries (72/161, 44.7%) and the other half consisted of intrathoracic injuries (77/161, 47.8%) (Figs. 2–7). Patients with GSWs were more severely injured than those with SWs with a mean ISS of 17.00 vs. 8.84 (P = 0.0014) and mean NISS of 22.87 vs. 11.38 (P = 0.0006). In addition, 53.3% GSW patients were classified as polytrauma patients (ISS > 16) compared to 16.7% SW patients (8/15 vs. 23/115).
Depth of penetrating injury to the thorax.
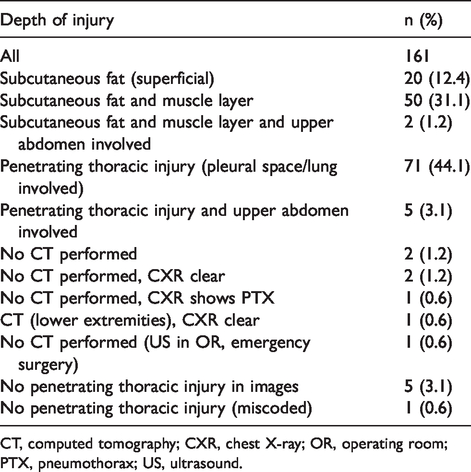
CT, computed tomography; CXR, chest X-ray; OR, operating room; PTX, pneumothorax; US, ultrasound.
Pneumothorax was frequently seen (70/161, 43.5%) (Figs. 2 and 3). Of those, 40 (57.1%) patients had chest tubes placed. Cardiac injuries were rare (1.2%, 2/161) and the mediastinum was violated in 5 (3.1%) cases: in three SWs, one GSW (Fig. 7), and one self-inflicted injury with a pen. Mediastinal injury was significantly more common in the GSW group than SW group (P = 0.0029, OR = 34.25, 95% CI = 3.30–355.14). Diaphragmatic injuries were found in 8 (5.0%) patients (SW 7, GSW 1). Active bleeding was found in 41 (25.5%) patients (Figs. 1 and 2). Of these 41 patients with active bleeding in CT images, 2 (4.9%) were treated with interventional radiology (coiling of cervical branch of thyreocervical trunk by a vascular surgeon and coiling of the left inferior mamillary artery [LIMA] by an interventional radiologist). Operative treatment was warranted in 6 (14.6%) cases; 3 (7.3%) patients had diaphragmatic rupture sutured and 2 (4.9%) patients had intercostal arteries ligated. One of the intercostal artery bleeds was most evident in late phase images (delay of 15 min) and was almost hidden by artifacts in the arterial phase. One patient had a brachial artery injury from a motor saw accident, which was operatively treated. Dermal sutures or staples were used in 10 (24.4%) patients and diathermia in 1 (2.4%) patient. Nineteen patients (46.3%) with active extravasation in CT images (e.g. minor intramuscular extravasation) were conservatively treated.
Osseous injuries were found in 24 (14.9%) of 161 patients (Table 4, Figs. 4 and 5), 19 in SW patients and four related to GSWs. Ribs were most commonly affected (17/161, 10.6%). Active bleeding (33.3% vs. 23.2%), osseous injuries (26.7% vs. 13.8%), and subcutaneous emphysema (93.3% vs. 73.9%) were more common in GSWs than SWs, and pneumothorax was more common in SWs than GSWs (45.7% vs. 33.3%). There was no statistically significant difference in these variables between the two groups (Table 4).
Comparison of imaging findings in SW and GSW patient groups.

*P < 0.05.
CI, confidence interval; GSW, gunshot wound; OR, odds ratio; SW, stab wound.Statistically significant values are written in bold.
Abdominal injuries were found in 54 (33.5%) of 161 patients, 45 (32.4%) in SW patients and 6 (40.0%) in GSWs. Of these, 17 were superficial injuries. Nineteen (11.8%) of 161 had combined chest and intra-abdominal injuries in this cohort (Figs. 5a, 7b and c). Small bowel injury was significantly more common in GSW group than SW group (P = 0.0034, OR = 12.18, 95% CI = 2.67–55.48). In 38 (70.4%) of the 54 abdominally injured patients, the entry wounds were only in the thoracoabdominal area or flanks. Thirteen patients suffered from solid organ injuries: 10 had liver injuries, two had kidney injuries, and one had a splenic injury. Based on evaluation of entry wounds and wound tracks, combined chest and intra-abdominal injuries were seen in 13 (8.1%) of 161 patients with other than evident abdominal entry wounds.
Time to CT
Of the 161 thoracic trauma patients, 150 (93.2%) were initially imaged with CT. Seven patients were examined with chest radiograph and ultrasound and four were taken directly to the operating room. Entry and exit wounds were marked with vitamin E capsules that are easy to distinguish in images and do not generate artifacts in CT (Fig. 6a). Wounds were marked in 110 (73.3%) of 150 patients.
When calculating the time to CT, one patient was excluded as an obvious outlier with time to CT of 1340 min (i.e. 22 h). With this in mind, the mean time to CT was 44.0 min (median = 29.5 min). No significant difference in mean time to CT was found between the SW and GSW groups (Table 1). However, a significant difference (P = 0.0106) was found in mean time to CT between polytrauma patients (ISS > 16) and non-polytrauma patients (ISS ≤ 16): 73.2 min vs. 36.8 min.
Imaging protocols
The arterial phase was included in 42 (28.0%) of 150 studies: SW 32/129 (24.8%); GSW 7/13 (53.8%); and other 3/8 (37.5%). Standard trauma CT-imaging protocol—including arterial phase of the neck, thorax, and abdomen and venous phase of the torso—was used in 14 (9.3%) of 150 patients. In 28 (18.6%) of 150 studies, the imaging included the arterial phase of the thorax. Active bleeding was found in 41/150 (27.3%). Of these, 12 were imaged in both the arterial and venous phases and 29 in the venous phase. Detection of active bleeding was aided by multiphase imaging in showing the increased amount of contrast media extravasation (Figs. 1 and 2). Only five patients were imaged with per oral contrast: two GSW; two SW; and one self-inflicted injury with a pen. However, 28 (18.7%) of 150 patients were administered per rectum contrast (three GSW, 25 SW) reflecting the multiple wound sites in these patients. Metallic foreign bodies visible in scout images were found in 17 (10.4%) of 163 studies. These included bullets (n = 6), bullet fragments (n = 5), shotgun pellets (n = 1), knife blade (n = 1), and staples or clips from wound suturing (n = 4).
Emergency surgery, postoperative imaging and mortality
Emergency surgery was performed in 10 (6.2%) patients. Of those 10 patients, 4 (40.0%) had emergency thoracotomy, 5 (50.0%) had laparotomy, and 1 (10%) patient had both body cavities (thorax and abdomen) explored. Patients with GSW were more likely to undergo emergency surgery, 3/15 vs. 6/138 with SW (P = 0.0450). One patient died perioperatively due to SW-induced cardiac injury.
The remaining nine patients underwent postoperative CT imaging. One patient had additional findings in the surgical field, liver laceration after laparotomy for suspected small bowel injury. Findings outside the surgical field included kidney injuries (n = 2), location of bullet fragments (n = 1), suboptimal positioning of chest tubes (n = 5), gunshot injuries in other locations than the operative field (n = 1), and major skeletal injuries (pelvic, spinal, and extremity fractures; n = 2). CT findings altered further treatment in 5 (55.6%) patients (Table 5). The 30-day mortality rate was low at 1.2% (2/161).
Summary of postoperative CT imaging after ES.

ABD, abdominal cavity; CM, contrast media; CT, computed tomography; ES, emergency surgery; F, female; fx, fracture; GSW, gunshot wound; HTX, hemothorax; ISS, Injury Severity Score; M, male; MOI, mechanism of injury; NISS, New Injury Severity Score; OR, operating room; PTX, pneumothorax; SW, stab wound; THX, thoracic cavity; US, ultrasound.
Discussion
Most of the penetrating injuries encountered in the Stockholm area are due to stabbing and significantly fewer due to GSW. However, a yearly increase of patients with GSW was detected in this study. Although blunt trauma is more common, the on-call radiologist must be familiar with radiological signs of penetrating trauma as well. Blunt traumatic injury can be predicted, to some extent, by detecting classical patterns of injury. Penetrating injury, however, is random depending on the type of weapon and violent force used.
Patients sustaining penetrating injuries are fairly young and more often male compared to patients with blunt chest trauma. The mean age of men in this cohort was 34.9 years (93.8% men); in a recent study of 547 blunt chest trauma patients the mean age was 46.6 years (74.0% men) (18). Predominance of young men is in concurrence with previous studies on penetrating trauma (4,19,20).
Early CT scanning and availability of a CT scanner in the emergency department has been shown to result in more goal-directed treatment and improve outcomes (21). In this cohort, mean time to CT was 44 min (median time = 29.5 min; starting from 13 min) reflecting the rapid logistics in the emergency department. However, in polytrauma patients (ISS > 16), time to CT was significantly prolonged compared to non-polytrauma patients (ISS ≤ 16). Stabilization of severely injured patients before imaging might explain this difference.
The pattern of injury in GSW is characteristically complex with ricochet injuries from bullets and shrapnel. In addition, the patient may have a mixture of blunt and penetrating trauma, as a result of fall or assault coinciding with penetrating injury. Wound marking facilitates in reconstruction of trajectories and is easily executed with vitamin E capsules (22). This marking does not deteriorate diagnostic performance, contrary to the use of paper clips in wounds that generate metal artifacts in CT images and may mimic metallic foreign bodies.
On-call radiologists and trauma surgeons are challenged by the complexity of penetrating trauma ranging from superficial benign lacerations to deep, potentially fatal vascular injuries. GSW victims were more severely injured than patients with SW in this cohort; GSW victims had higher ISS scores and increased tendency to undergo emergency surgery.
Active bleeding, tension pneumothorax, and airway obstruction should be promptly managed to improve outcome. The wound trajectory can be determined by following free air bubbles in soft tissues (23). SW to the back and shoulders often remain superficial due to the thick muscle layers. Low-energy stab injury is limited to subcutaneous tissue and muscles or is limited by anatomical boundaries as the knife reaches the ribs or scapula.
Nearly half of the injuries encountered in this cohort extended to pleural space. Also, more than one-fourth of patients suffered from injuries with active bleeding, thus requiring supervision and control of hemodynamics. Arterial and venous phase imaging eased the recognition of these bleeds, even though most of them were treated conservatively. The use of intravenous contrast media is crucial to evaluate vessel and organ injury and active bleeding. CTA is the imaging method of choice in all penetrating trauma to rule out vascular injury (7,9,10,24). In this cohort, the standard protocol including arterial phase was rarely used. Including modified protocols, arterial phase was included in 28.0% of studies. Cardiac injuries were rare, but penetrating trauma extending to intrapericardial space carries a high mortality rate and patients often die before arrival to the hospital. (25).
The amount of diaphragmatic injuries was fairly high—in previous reports, diaphragmatic injury has been suggested to be more common in penetrating than blunt trauma (26,27). The size of diaphragmatic injury is usually significantly smaller in penetrating than blunt trauma and, as such, it may be more difficult to detect (27). In addition, one-third of patients had abdominal injuries in addition to thoracic trauma. Tailoring the scan to a specific body region increases the risk of leaving additional injuries uncovered and delaying proper diagnosis. Therefore, it is recommended that in cases of penetrating injury, scanning should be extended to the nearby compartment and preferably scan the whole body (9).
Postoperative imaging after emergency surgery is highly recommendable (16). Bleeding to the retroperitoneal cavity, active bleeding, and injuries in abdominal or retroperitoneal solid organs might remain hidden during emergency laparotomy. Additional skeletal injuries in the pelvis, spine, and extremities are essential to assess, particularly in patients with coinciding blunt and penetrating trauma. In addition, the posterior part of the hepatic vessels and inferior vena cava are hard to reach during surgery (16). In this cohort, additional findings in the field of surgery were scarce, but additional GSW injuries, skeletal fractures, and bullet fragments were seen outside the field of surgery. Detection of lodged bullet fragments (Figs. 6b and c, 7c) is crucial to ensure the safety of subsequent magnetic resonance imaging studies in the acute phase or after recuperation (28). In the acute setting, chest tubes are often inserted in a limited time window. Any chest tube malposition is easier to evaluate in CT than in supine radiographs (29).
Limitations of this study include the retrospective design. However, the trauma registry data were essential in forming a comprehensive cohort of penetrating trauma patients. In severely injured patients, analysis of trauma registry data is a feasible method to adjust and modify current practices in diagnostics and treatment and to evaluate outcome (30,31). A relatively small sample size reflects the low incidence of penetrating trauma in the Nordic countries.
The overall incidence of penetrating trauma is increasing (8). In particular, mass casualty incidents can result in a sudden influx of severely injured patients to any large hospital. Imaging protocols must be optimized to secure rapid but accurate diagnostics according to triage to reduce mortality and morbidity related to these incidents. A standard whole-body CT protocol including arterial phase imaging is recommended to rule out vascular injury that is commonly seen in these patients, as shown in our study. In everyday practice, these injuries are infrequently encountered, thus posing a challenge for the on-call radiologist.
In conclusion, penetrating thoracic trauma often violates intrathoracic structures and nearby compartments. Arterial phase whole-body CT imaging is recommended as multiple injuries and active bleeding are common. CT imaging after emergency surgery is warranted, especially to assess injuries outside the surgical field.
Supplemental Material
ARR895485 Supplemental Material - Supplemental material for Imaging of penetrating thoracic trauma in a large Nordic trauma center
Supplemental material, ARR895485 Supplemental Material for Imaging of penetrating thoracic trauma in a large Nordic trauma center by Mari T Nummela, Sigurveig Thorisdottir, Gudrun L Oladottir and Seppo K Koskinen in Acta Radiologica Open
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no specific financial support for the research, authorship, and/or publication of this article. MN received two “Travel Grants for International Research Visits for Doctoral Candidates in the Doctoral Programme in Clinical Research” from University of Helsinki for research visits to Karolinska University Hospital, Stockholm.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.