
Abstract
Deep vein thrombosis affects approximately 1–2 per 1000 individuals each year. We present an alternative imaging option for detecting deep vein thrombosis in the lower legs using time-resolved dynamic computed tomography venography with ultra-low contrast medium dosage.
Introduction
Deep vein thrombosis (DVT) affects approximately 1–2 per 1000 individuals each year. DVT may lead to pulmonary embolism, a potentially fatal condition requiring prompt diagnosis and treatment. The underlying causes of DVT include surgery, immobilization, trauma, heart failure, smoking, and overweight (1).
Phlebography used to be the primary diagnostic method but has been replaced by Doppler ultrasonography (US) during the last decade. The main reasons for abandoning phlebography are its invasiveness, use of rather large amounts of contrast medium (CM; approximately 32 g), and radiation exposure. However, Doppler US is user-dependent and requires operator skill when evaluating the lower leg. The technique is especially difficult in patients with a history of previous thrombosis in whom the normal anatomy might have become distorted (2,3). An alternative diagnostic method is computed tomography venography (CTV), where the use of low kilovolt (kVp) scanning or dual-energy technology has resulted in high sensitivity for DVT (4). Typically, CTV technique requires 30 g of iodine. In patients with end-stage renal disease or in those at risk of acute kidney injury, an alternative method using less CM is called for. Ideally, magnetic resonance imaging (MRI) can be used (5), but availability and lack of experience often limit its use.
Improvements in CT technology have enabled the development of time-resolved perfusion CT angiography (P-CTA), in which multiple passages/sequences are acquired over the organ of interest. The high temporal resolution guarantees that even a short CM bolus can be detected with optimal arterial enhancement. Using image data, post-processing the rendered images can be shown as a movie and the inflow of the CM in the vessels can be visualized as high-resolution time-resolved images (6,7).
We present an alternative imaging option for detecting DVT in the lower legs using time-resolved dynamic CTV with a minimum amount of intravenous CM.
Case report
A 45-year-old man with a previous history of DVT in the lower left leg (18 years previously), after immobilization due to fever and sore throat, began to suffer from persistent pain and swelling in the left lower leg. Doppler US indicated outer compression of the common femoral vein, superficial femoral vein, and popliteal vein. Although Doppler US raised the suspicion of thrombosis in one of the posterior tibial veins, it could not be verified owing to suboptimal image quality. Being a radiologist, the patient requested dynamic CT imaging rather than undergoing a standard phlebography.
The dynamic CTV was performed using a dual-source multidetector (MDCT) Somatom Definition Flash® (Siemens Healthcare, Forchheim, Germany). A total of eight repeated scans over a range of 48 cm starting approximately 15 cm cranial of the left tibial plateau were performed at intervals of 3 s using 70 kVp and 60 mAs. A power injector (Medrad®, Stellant® Dual Head Injector, Bayer, Pittsburgh, PA, USA) was used to inject 105 mL of diluted contrast media (5 mL of iomeprol 400 mg iodine per mL [Iomeron®-400, Bracco Imaging SpA, Milan, Italy] mixed with 100 mL saline). The injection rate was 4 mL/s using an 18-G peripheral venous access inserted into a dorsal vein of the left forefoot. A stasis was applied proximal to the left knee to ensure CM opacification of the deep veins. Scan delay was set to 10 s after the media injection commenced. The dynamic time-resolved scan data were exported to a dedicated workstation (syngo.via, Siemens Healthcare, Forchheim, Germany) for motion correction. All three-dimensional (3D) volume rendering (VR) and post-processing were done at a separate workstation (Advantage work station 4.5, GE Healthcare, Milwaukee, WI, USA).
Dynamic CTV confirmed the finding of Doppler US that there was outer compression of the common femoral vein, superficial femoral vein, and popliteal vein, probably from surrounding fibrotic tissue after the previous DVT (Fig. 1). The collateral vein development post DVT was illustrated and a fresh thrombus surrounded by CM was visualized in one of the posterior tibial veins (Figs. 2 and 3; video).

Volume rendering images (VR) showing compression of the common femoral vein, superficial femoral vein, and popliteal vein (arrows).
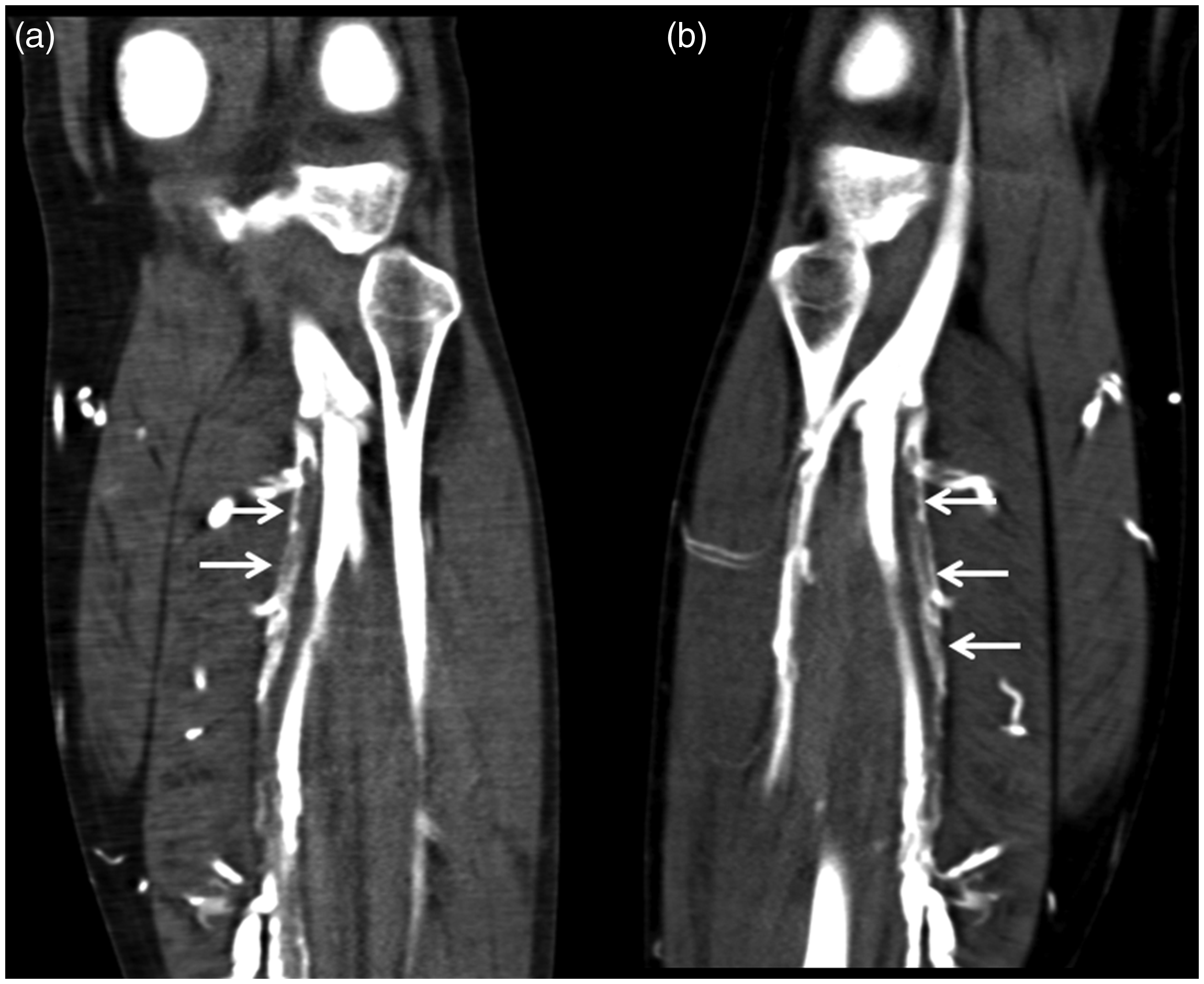
(a, b) Multiplanar reconstruction (MPR) images showing fresh CM-surrounded thrombi in one of two posterior tibial veins (arrows).

Axial image showing thrombi in one of two posterior tibial veins (arrow).
Discussion
In this study, an ultra-low CM dose of 2 g of iodine was sufficient to adequately visualize a DVT at dynamic CTV. The dilution of CM by saline decreased its viscosity, facilitating the injection, and is likely to reduce the risk of extravasation. Despite the very low dose of injected iodine, the CM attenuation in the veins was still high, about 600 Hounsfield units (HU). This indicates that an even lower iodine dose may be used. Theoretically, a CM dose as low as 1 g can be used. By applying external stasis, the blood was successfully shunted to the deep veins and the dynamic time-resolved scanning technique ensured visualization at the optimal timepoint. The total radiation dose corresponding to the eight-scan series was approximately 0.2 mSv, i.e. equivalent to a chest radiograph. By merging the different scan series, it was possible to visualize the contrast medium's filling of the lower leg veins in 4D (video). The dataset can also be rotated freely to visualize the anatomy and pathology in the most optimal projection. Moreover, the series can be motion-corrected; individual series with the highest CM enhancement can be merged into a single series to improve contrast-to-noise ratio. We believe that dynamic CTV with ultra-low CM dose is a versatile tool in the diagnostic arsenal of DVT in the lower legs, especially in patients with high risk of acute kidney injury with unequivocal ultrasound.
Footnotes
Declaration of conflicting interests
The authors declared no conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.