
Abstract
Despite diagnostic and therapeutic advancements, mortality and morbidity rates in the patients diagnosed with oral cancer remain static. Hence, an understanding of the factors that predict the progression of oral cancer appears to be useful in deciding on the most appropriate therapy, thereby improving survival. To do so in practice, a critical knowledge of prognostic markers that have high sensitivity is essential. Though recent research has introduced newer molecular markers, challenging the conventional prognostic assessment methods their universal application is yet to be determined. In practice, clinical and histopathological parameters are widely used for the selection of treatment strategies and for the determination of prognosis in oral cancer patients. A literature search yielded a multitude of parameters to be involved in the determination of prognosis of a patient. Based on published evidence, factors of significance were pTNM, tumour volume, depth of invasion, surgical margin status, tumour budding, vascular and perineural invasion, medullary bone invasion, extracapsular spread and the presence of distant metastasis.
Introduction
Diverse malignant tumours of various cellular lineages originate in the oral cavity. Among these, squamous cell carcinoma (SCC) constitutes a significant proportion, comprising 95% of head and neck cancers. Oral squamous cell carcinoma (OSCC) has a striking global incidence and equally formidable mortality rates. 1 The worldwide mortality caused by cancer of the oral cavity and lip was estimated to be 128,000. 2 Despite enormous advancements in the field of diagnostics and therapeutics, the overall survival rate in most countries ranges between 45% and 50% and has not shown a significant improvement during the past few decades. 1 At present, the clinical and histopathological parameters are mostly employed for the planning of treatment strategies as well as determining the prognosis of oral cancer patients. The present narrative review aims to present the role of clinico-pathological parameters and their influence on the prognosis and survival rates of OSCC.
Method: A web-based search was performed via PubMed database, with keywords: oral cancer, OSCC, prognosis, survival, clinico-pathological, histopathology and molecular markers. Original research (2014–2017, studies involving 3–5 years overall, disease-specific, disease-free survival, disease progression and recurrence rates) and review articles published in English language were included for the appraisal of various prognosticators in OSCC. Based on the literature search, an overview of various prognostic factors was structured, as depicted in Figure 1.

Working classification of prognostic determinants of OSCC. OSCC: oral squamous cell carcinoma.
Clinical factors
Anatomic location
The anatomic sites within the oral cavity exhibit variations in histology, vascular supply and lymphatic network. In addition to these factors, accessibility to visual examination of the site may further influence the early diagnosis of OSCC. 3,4 The importance of the primary site of tumour and its role in survival has been emphasized in the literature. 5 –8 Various published studies have demonstrated the significance of anatomic location in the survival of OSCC, as depicted in Table 1. 9 –19 Cases which occurred on the buccal mucosa tend to be well differentiated, whereas cancers of palate, tongue and floor of the mouth are poorly differentiated. 20 In a case study (2311 patients, below 45 years of age) by Santos et al., an association between the primary location of tumour and advanced clinical stage showed that increased cases of advanced stages were found in the intraoral sites as compared to the lips. 21

OSCC: oral squamous cell carcinoma.
*70% without elective neck dissection, 77% with neck dissection.
TNM staging
Published studies have demonstrated a decisive role of TNM staging in the prognostic outcome of oral cancer cases (Table 2). 22 –25 Kreppel et al., in 392 oral cancer patients, showed that pTNM had a higher prognostic superiority than cTNM. 26 Other studies have also revealed a significant influence of TNM staging on prognosis and long-term survival. 27,28 A new staging system was proposed by Lee et al., which has shown better disease-free survival discrimination and ability to identify high-risk group patients with OSCC. The authors estimated the hazard ratios with 95% confidence intervals (CIs) for a range of selected prognostic variables. Those with statistical significance at p < 0.10 were further subjected to a multivariate proportional hazards regression model. Following which, an integer scoring system was developed. Individual scores were assigned which included perineural invasion, 1 point; lymph node ratio (LNR), 1 point; advanced pT (T3 + T4), 1 point; and advanced pN (N2), 3 points. The total scores were stratified for the new staging category, which were as follows: stage I, score of 0; stage II, score of 1; stage III, score of 2 or 3; and stage IV, score of 4–6. When compared with the American Joint Committee on Cancer (AJCC) staging system, the new staging categories showed a better discriminatory ability for a 5-year disease-specific survival. 29

OSCC: oral squamous cell carcinoma.
Histopathological factors
Histopathological differentiation
Histopathological differentiation of the tumour does have an influence on prognosis. Severe grade (Figure 2) often indicates a poorer prognosis. 30 Kolokythas et al. showed that the grade of differentiation as well as degree of keratin expression in SCC of the tongue to be significantly associated with poor outcomes, that is, cases with grade 3 and 2 differentiation demonstrated acceleration in disease progression compared to those with grade 1 by a factor of 6.9 and 11.0, respectively, and cases with a keratin score of 3 (least) and 2 (intermediate) demonstrated acceleration in disease progression by a factor of 2.2 and 6.4 compared to those with a keratin score of 1 (most). 31

Pictomicrograph showing dysplastic cells with poor differentiation in the case of high-grade OSCC (400 original magnification, H&E stain). OSCC: oral squamous cell carcinoma; H&E: haematoxylin and eosin.
Histopathological grading systems
Different grading systems for OSCC vary in their prognostic significance. Broder’s was the first grading system proposed for the prognosis of OSCC. However, a lack of correlation between Broder’s grades and prognosis has been observed. 32 The main reason cited being, malignant squamous cells usually exhibit a heterogeneous population with differences in the degree of differentiation. Furthermore, tumour–host relationship is not considered in Broder’s grading and lastly, it is not a quantitative method (lacks a scoring system). 33,32 Bryne’s grading system was found to have a prognostic significance in a recent study by Dissanayake. 34 Calone et al. and Strieder et al. compared the prognostic significance of various grading systems and showed that the Almangush et al. grading system to be a simple and an effective tool for the prognostic evaluation of SCC. 35,36 In a further study involving SCC of the lower lip, the Brandwein-Gensler risk model was found to be a superior grading system. 37
Tumour volume
Tumour volume can be assessed by imaging scans or by macroscopically measuring the surgical specimen. Tumour volume significantly predicted the disease-free and overall survival of patients with already advanced (T4a) OSCC. 38 A study by Mücke et al., including 437 OSCC patients, showed similar results, that is, tumour volume was significantly associated with the overall survival of the patients. 39
Tumour thickness
Tumour thickness measured in pathology specimens (Figure 3) has been used as a prognostic factor. A tumour thickness of <8 mm and >8 mm was proven to be a better predictor of lymph node metastasis, including the cases of occult metastasis in SCC of the tongue. 40 Likewise, tumour thickness of >7 mm was found to be predictive of lymph node metastasis and a thickness of >10 mm showed poorer disease-free survival in the cases of early SCC of the tongue. 41 The tumour margin to tumour thickness ratio was found to be an independent predictor of local recurrence and disease-specific death. 42 The correlation between tumour thickness at two different mucosal sites (tongue and floor of the mouth) and their propensity for nodal metastasis showed that the critical tumour thickness value (which represents the thickness at which the probability of nodal metastases exceeds 20%) for SCC involving the floor of the mouth was 1–2 mm, whereas for SCC of the tongue was approximately 4 mm. 43

Estimation of DOI (red line) is achieved by measuring the distance perpendicularly from the level of adjacent normal epithelial basement membrane (green line) to the point of deepest invasion. TT (blue line) is a measure of entire dimension of the tumour from the surface to the point of deepest invasion. (a) in exophytic/superficial OSCC: TT > DOI and (b) in ulcerative OSCC: DOI > TT. Note: In this case, TT is deceivingly less than the actual DOI which would underestimate the true aggressive potential of the tumour. DOI: depth of invasion; TT: tumour thickness; OSCC: oral squamous cell carcinoma.
Depth of invasion
Depth of invasion (DOI) is measured from the basement membrane of the closest adjacent normal mucosa to the deepest point of tumour invasion. The correct method of measuring DOI and tumour thickness is depicted in Figure 3. 44 Kuan et al. showed that DOI significantly influenced the decision for neck dissection in the cases of SCC of the tongue. 45 DOI is one of the parameters of the Almangush et al. grading system, that is, tumour budding – DOI (BD grading system), which has been found to be a good prognosticator of the survival of OSCC patients. 46,47 DOI is now incorporated into the American Joint Committee on Cancer (eighth edition) Cancer Staging Manual. 44
Surgical margins
The UK Royal College of Pathologists classifies the surgical margin as clear (when the distance of 5 mm or more is evident from the invasive tumour cells), close (1–5 mm) and positive or involved (<1 mm). 48 Buchakjian et al. reported that the surgical margins yielded significant prognostic data for the recurrence and survival of OSCC patients. 49 Likewise, a study by Ettl et al. showed that R0-resected head and neck carcinomas, with definite close margins, were associated with aggressive tumour features as well as adverse disease-specific survival. Further, the prognostic impact of an intraoperative frozen section analysis was questionable and of limited accuracy. 50 OSCC cases with free margins of ≤4 mm were related to an increased risk of local recurrence, while cases with free margins of ≥5 mm were not related to a significant risk of local recurrence. 51 According to El-Fol et al., a significant discrepancy was observed between intraoperative and histopathological margin assessment due to tissue shrinkage, and in addition such discrepancies were associated with the anatomic location of the tumour. For example, the buccal mucosa presented with a statistically significant mean discrepancy of 47.6% between the in situ and the histopathological margins of all close and positive margins. 52 In a study, comprising 20,602 patients with early oral cancer (stage I/II), it was observed that the margin status could serve as a useful quality measure for early oral cancer. 53 Similarly, other studies have also demonstrated the prognostic significance of inadequate surgical margins in OSCC. 54,55
Tumour invasion
Invasive front
The invasive front is of great importance, as the tumour cells at the invading end are relatively more proliferative, as compared to the superficial part. 30 As a consequence, when using Bryne’s method of malignancy grading, it is implemented at the invasive front of the tumour. The correlation between survival and invasive front revealed that a higher invasive front grading (tumour islands with >15 and <15 tumour cells) was associated with overall poor survival. 56 As noted in the above study, the invasive front was evaluated in resected/excised specimens, whereas often for initial diagnosis and prognosis determination, incisional biopsy specimens are submitted to a pathologist. Dhanda et al. conducted a study to determine the prognostic utility of biopsy specimens in OSCC. The biopsy depth was significantly under-represented than the actual tumour depth; hence, the evaluation of important histopathological prognosticators such as pattern of invasion and so on was limited in biopsy specimens. 57
Tumour budding
This represents a specific pattern of aggressive growth of carcinomas at the invasive front, comprising single or small clusters (<5 cells) of tumour cells (Figure 4). 58 This feature is observed to be significantly associated with the overall survival of the OSCC patients and is proposed to be an independent prognostic indicator. 59,60 Tumour budding is found to be a good predictor of clinically node-negative OSCC cases, further adding its utility as an important histopathological parameter. 61 Angadi et al. reported high-intensity tumour budding to be a strong independent prognostic factor for the prediction of lymph node metastasis. 62 The prognostic efficacy of tumour budding in early-stage tongue SCC has also been observed. 63,46

Pictomicrograph showing tumour budding (black arrows) observed at the invasive front of OSCC at (a) low and (b) higher magnification, respectively (100 and 400 original magnification, H&E stain). OSCC: oral squamous cell carcinoma; H&E: haematoxylin and eosin.
Perineural and vascular invasion
Vascular invasion is characterized by the presence of neoplastic cells within the lumen or in the wall of lymphatics and blood vessels (Figure 5), while perineural invasion (Figure 6) denotes a tropism of neoplastic cells for nerve bundles. Various studies have suggested that both perineural and vascular invasion are the known predictors of poor outcome in OSCC patients. 64,65 In a study (571 OSCC patients), it was observed that relative to vascular invasion, lymphatic invasion was significantly associated with poorer overall survival, disease-specific survival and disease-free survival. However, lymphatic invasion was not found to be an independent prognostic factor. 66

Pictomicrograph showing vascular invasion in OSCC (400 original magnification, H&E stain). OSCC: oral squamous cell carcinoma; H&E: haematoxylin and eosin.

Pictomicrograph showing perineural invasion by malignant squamous cells (400 original magnification, H&E stain). H&E: haematoxylin and eosin.
Sarcolemmal spread
Similar to vascular and perineural invasion, the neoplastic cells might spread along the sarcolemmal sheaths of muscle fibres (Figure 7). The involvement of the muscle tissue by the tumour cells is usually observed at late stages of cancer, probably due to their deeper location. 67 However, the literature search did not reveal any research papers related to the prognostic significance of sarcolemmal spread in OSCC cases.
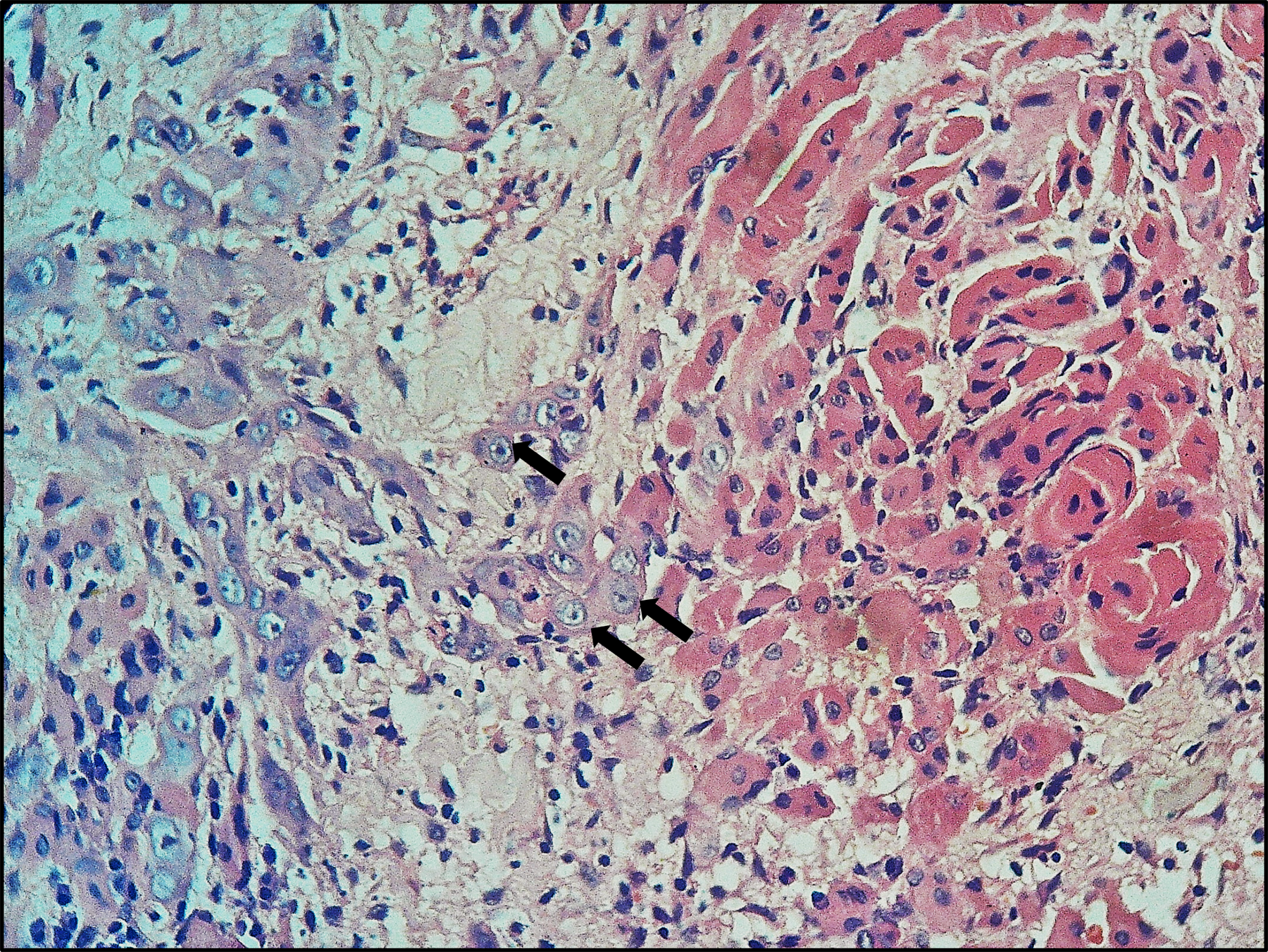
Pictomicrograph showing sarcolemmal spread (black arrows) in OSCC (100 original magnification, H&E stain). OSCC: oral squamous cell carcinoma; H&E: haematoxylin and eosin.
Spread to bone
According to the eighth edition AJCC Cancer Staging of lips and oral cavity, a tumour is to be categorized as T4 when it invades through the cortical bone and not merely causes superficial erosion alone of bone/tooth socket by the gingival primary. 44 This invasion is not specified as cortical or medullary. However, histopathological studies on its prognostic significance in OSCC have a grouped pattern of bone invasion into cortical/medullary or erosive/infiltrative patterns. 68,69 A systematic review by Li et al. showed that mandibular medullary invasion could be an independent prognostic factor rather than merely mandibular cortical invasion in OSCC patients. 70 A study of 96 OSCC cases (tumour ≤ 4 cm) by Fives et al. showed medullary bone invasion in mandible as a poor prognostic indicator regardless of the size of the primary tumour. 71 Kuk et al. concluded that bone invasion, in small-sized tumours (T1 <2 cm and T2 >2 cm to ≤4 cm), is not an independent prognostic factor. However, tumours presented with both buccal and lingual bone invasion had a significantly worse prognosis. 72 Okura et al. reviewed 345 patients with mandibular gingival OSCC and determined that mandibular canal invasion was an independent predictor of decreased survival rate, whereas medullary bone invasion was an insignificant prognostic indicator with respect to the survival of patients. However, medullary bone invasion was significantly associated with distant metastasis. 73 In a study by Namin et al., the efficacy of bone marrow margin cytological preparations in OSCC cases and its role in the detection of occult invasion and prognosis was assessed. The difference in the prognosis of positive as well as negative bone marrow margins was insignificant. 74
Sialadenotrophism
This refers to the dysplastic changes along the lumen of the salivary gland ducts (Figure 8). 67 A literature search revealed a study by Mohan et al., wherein changes in minor salivary glands were evaluated in 250 OSCC cases. The alterations observed in excretory ducts included simple hyperplasia (eight cases), squamous metaplasia (six cases), mucous metaplasia (one case), oncocytic metaplasia (one case), moderate dysplasia (five cases), severe dysplasia (one case) and malignant cell infiltration into the duct (seven cases). Within the gland, similar ductal changes were noted, which included ductal proliferation, ductal metaplasia, dysplastic changes and infiltration by malignant squamous cells. Presently, the prognostic role of these findings in OSCC is uncertain. Nevertheless, the glands that have undergone dysplastic changes/malignant cell infiltration should be excised, as there have been reports of recurrence of OSCC due to inadequate removal of such salivary gland tissues. 75
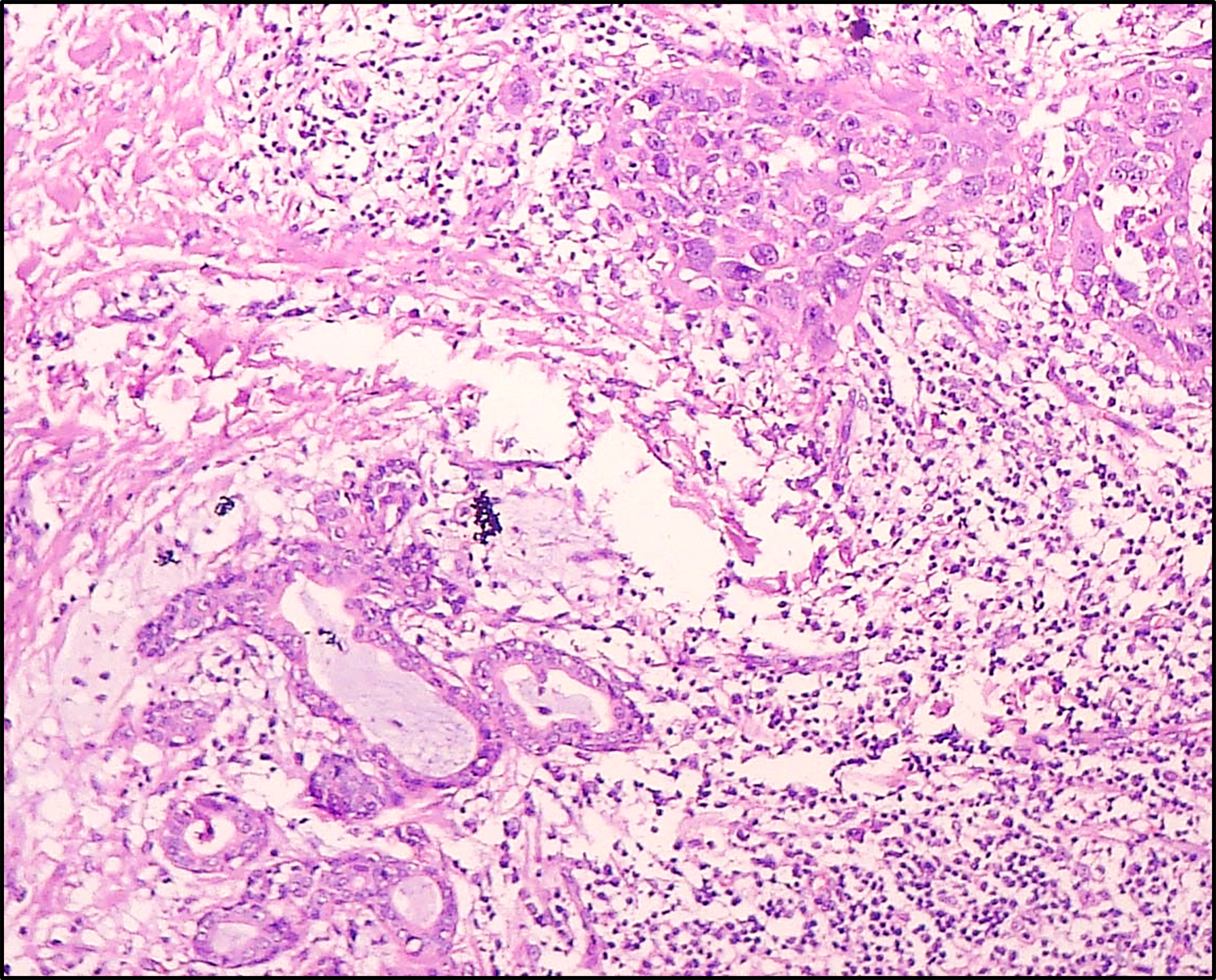
Pictomicrograph showing sialadenotrophism in OSCC (100 original magnification, H&E stain). OSCC: oral squamous cell carcinoma; H&E: haematoxylin and eosin.
Cancer-associated inflammation
Cancer-associated inflammation (Figure 9) is known to play an important part in the progression of many neoplasms. In addition, current evidence suggests that the various components of the inflammatory response might also be noteworthy prognostic indicators. It is observed that SCC cases with a high number of tumour-infiltrating lymphocytes have a better prognosis and might serve as an independent predictor of recurrence. 76 An elevated neutrophil to lymphocyte ratio statistically correlated with an advanced stage of OSCC and poor response to chemoradiotherapy. 77 Kindt et al. demonstrated that a high number of Langerhans cells in both intratumoural and stromal compartments of head and neck squamous cell carcinoma (HNSCC) cases are associated with longer recurrence-free survival. 78 Other studies have revealed that B regulatory cells in tongue SCC; micro-localization of CD68+ tumour–associated macrophages in tumour stroma; systemic inflammation scores including the modified Glasgow Prognostic Score in patients undergoing potentially curative resection for OSCC; expression of Fas ligand in tumour lymphoid cells; tumour-infiltrating neutrophils; expression of HIF-1α in tumour and peri-tumoural inflammatory cells; tumour-infiltrating lymphocytes and T regulatory cells; CD8+/CD4+ cell ratio; may predict clinical outcome and survival of the patients. 79 –88 On the contrary to the above observations, a study by Affonso et al. showed that peri-tumoural inflammation has no prognostic implications in OSCC. 89

Pictomicrograph showing marked inflammatory response at the invading tumour front in OSCC (400 original magnification, H&E stain). OSCC: oral squamous cell carcinoma; H&E: haematoxylin and eosin.
Tumour-associated tissue eosinophilia
Tumour-associated tissue eosinophilia (TATE; Figure 10) count is proposed as a prognosticator and has been correlated with nodal metastasis in OSCC cases. 90 TATE count has also been correlated with tumour differentiation and found to be lower in poorly differentiated SCC. 91 In addition, TATE count was found to be significantly higher at the invasive front than at other parts of the tumour stroma. 92 In a study, TATE count was correlated with pattern of invasion. The findings revealed a progressive decrease in TATE count with an increase in the grading of pattern of invasion, suggesting its possible protective role in tumour cell cytotoxicity and progression. 93

Pictomicrograph showing tumour-associated eosinophils interspersed among the invading squamous cells (400 original magnification, H&E stain). H&E: haematoxylin and eosin.
Cellular cannibalism
Several authors have emphasized that the number of cannibalistic cells (Figures 11 and 12) can be correlated with the aggressive and metastatic behaviour in systemic malignancies. Towers and Melamed have stated that an increased number of cannibalism may be useful in the grading of breast carcinoma. 94 OSCC consists of a diverse cell population with probable differences in invasiveness and metastasis behaviour. Hence, clinical behaviour depends on whether a tumour consists of highly aggressive cells or not. In our previously reported studies, the differences in the mean cannibalistic cells for well versus moderately, moderately versus poorly and well versus poorly differentiated OSCC were statistically significant. It is concluded that poorer the differentiation in cancer cells, more is the cannibalistic activity. The poorly differentiated OSCC is more aggressive with high proliferative rate. We speculated that nutritional supply to tumour cells is not in pace with the high proliferation–related tumour load. This may lead to an increase in the nutritional demand in tumour mass, which could probably initiate cannibalism in tumour cells. Cellular cannibalism in OSCC has also shown good correlation with TNM stages and lymph node metastasis, making it an ideal histopathological prognosticator. However, some earlier authors did not report statistically significant correlation of cell cannibalism with the histopathological grades. 95,96

Photomicrograph showing classical morphological features of cannibalism phenomenon in various stages (arrows). (Photomicrograph is from Sarode et al. Complex cannibalism: an unusual finding in oral squamous cell carcinoma. Reference no. (Reprinted with permission from Elsevier’s Rights Department, Philadelphia, PA, USA). (H&E stain, original magnification 400)). H&E: haematoxylin and eosin.
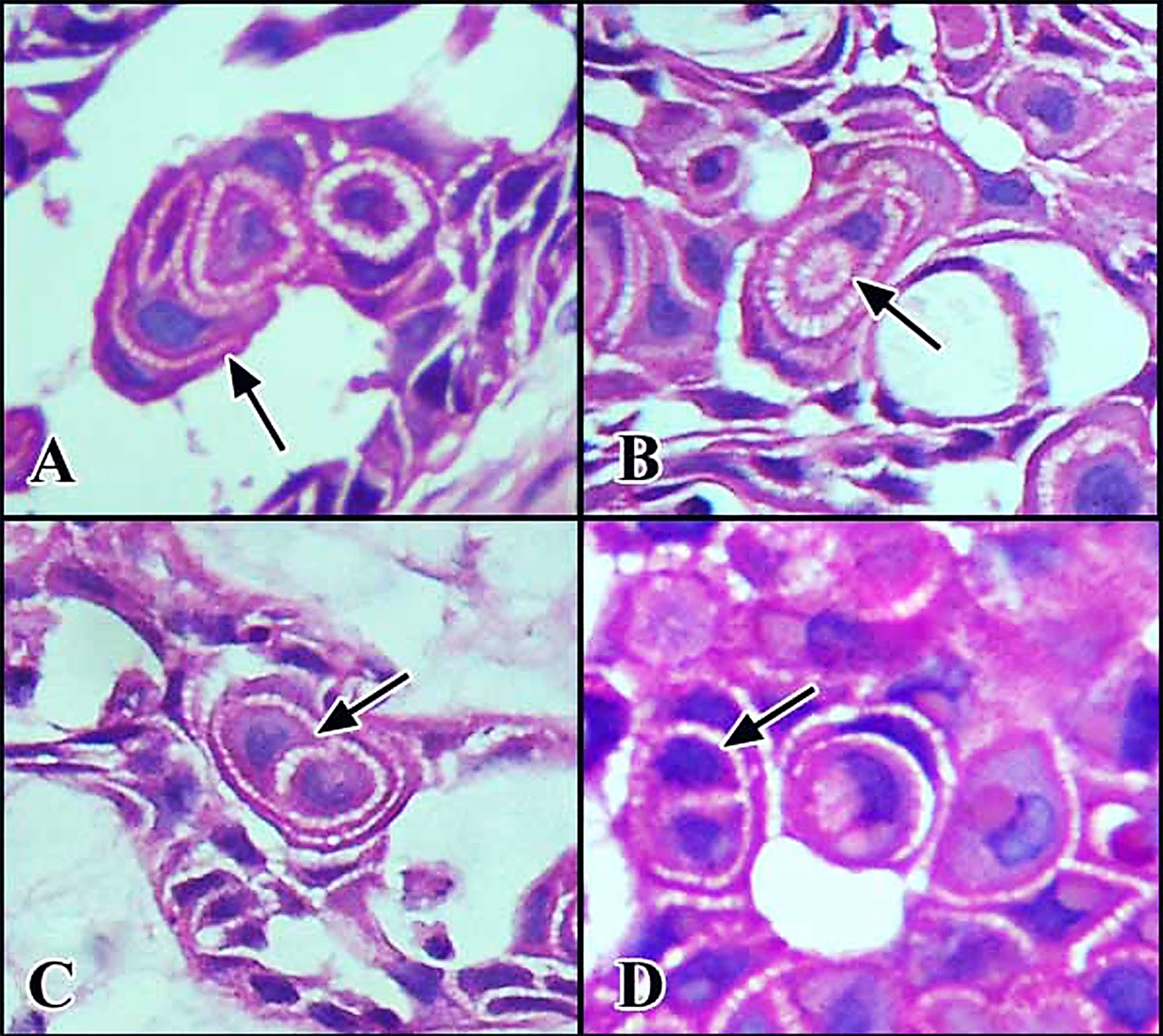
Photomicrograph showing ‘Complex Cannibalism’. (a) One malignant cell is engulfing another cell and this complex is engulfed by another cell. (b), (c) Cannibalism phenomenon showing difficulty in describing morphological features. (d) One malignant cell is engulfing two cells. (Photomicrograph is from Sarode et al. Complex cannibalism: an unusual finding in oral squamous cell carcinoma. Reference no. (Reprinted with permission of Elsevier’s Rights Department, Philadelphia, PA, USA). (H&E stain, original magnification 400)). H&E: haematoxylin and eosin.
Metastasis
Lymph node metastasis
It is one of the most consistent prognosticators of the head and neck carcinoma. The outcome of nodal involvement and the level of distribution on the survival of OSCC patients (8281) revealed that the 5-year, disease-specific survival was 42.0% for patients with only level I, II or III involvement, whereas for level IV group, it was 30.6% and for level V group it was 26.4%. The results of level IV and V were statistically significant and indicated worse prognosis. 97 Similar findings have been demonstrated by several others. 98 –101 In another interesting study, the impact of the involvement of facial lymph node on survival was assessed. Of 641 OSCC patients, 103 presented with metastasis to facial lymph nodes and were strongly associated with poor disease control and lower survival rates. 102 Studies have also shown that the number, size as well as occult node metastasis have a significant impact on the survival rates. 103 –105
Lymph node ratio
LNR has been used as a prognostic factor in various carcinomas and is defined as the ratio of the number of tumour-positive lymph nodes to the total number of lymph nodes removed. 106 A study revealed that cases with >0.092 LNR had an overall survival rate of 24.2%, whereas cases with <0.092 LNR revealed an overall survival rate of 45.8%. 107 However, a previous study proposed the LNR value to be in the range of 0.05–0.07, dividing the patients above this range as high-risk and below as low-risk group. 108 LNR stratification value for high-risk patients has been suggested to be higher than 6%. It was found to be a good prognostic tool in patients with pN0–pN2b lymph node status. 109 In another study, patients with LNR value <0.1 had better 3-year overall survival and local failure–free survival, which was also found to be an independent prognostic factor for overall survival. 106 Contrary to the above studies, de Ridder et al. suggested that the number of tumour-positive lymph nodes appears to be a more dependable parameter than LNR, provided a minimum number of lymph nodes were examined. 110
Extracapsular spread
The presence and extent of extracapsular spread (ECS) is considered to be important in prognosis determination (Figure 13). Previously, most of the studies reported ECS as present or absent as there was no clear macroscopic or histologic criteria. It was Lewis Jr et al. who attempted to provide a prognostically significant grading system for ECS. 111 However, the results of a meta-analysis by Mermod et al. revealed that ECS has a negative impact on locoregional recurrence as well as distant metastasis in HNSCC patients. 112 The prognostic cut-off value of ECS has been suggested to be 1.7 mm, and the disease-specific survival was significantly lower for patients with more than 1.7 mm involvement beyond the capsule. 113 Patients with macroscopic tumour invasion had a higher recurrence rate (69.8%) with a 3-year disease-specific survival of 49.0% and a relatively poorer prognosis. 114 ECS has recently been introduced to pTNM staging in the American Joint Committee on Cancer (eighth edition) Cancer Staging Manual.

Pictomicrograph showing the presence of islands of malignant squamous cells (black arrows) at the extracapsular region of a lymph node (100 original magnification, H&E stain). H&E: haematoxylin and eosin.
Distant metastasis
Although the incidence of distant metastasis has decreased with the advent of advanced and combined therapies, it is considered as an important parameter for prognosis in the patients. A clinico-pathological study by Takahashi et al., comprising 502 OSCC cases, revealed 54 cases were positive for distant metastasis. The survival period of the patients ranged from 1 to 21 months with a median of 3 months, after confirmation of metastasis. In addition, locoregional recurrence was also noted in 29 of 54 cases. 115 In another study, the overall survival rates were found to be 72.0% (95% CI, 53.4–89.6) at the end of 1 year and 40.8% (95% CI, 20.6–61.0) after 2 years of development of distant metastasis in the cases of oropharyngeal SCC. 116
Molecular markers
A number of markers have demonstrated their prognostic utility in OSCC; however, due to lack of proper trials and validations, the practical application of these markers is debatable. A working classification along with some of the markers with prognostic significance is listed in Table 3. 117 –123

PCNA: Proliferating cell nuclear antigen; EGFR :Epithelial growth factor receptor; PTEN :Phosphatase and tensin homolog; RB1 :Retinoblastoma-1; VEGF: Vascular endothelial growth factor; VCAN :Versican.
It is observed that site-wise distribution of OSCC is responsible for intra and inter-tumoural heterogeneity. In this regard, some authors studied buccal mucosa and tongue OSCC for possible heterogeneity in the cell cycle regulatory mechanism by comparing major cell cycle regulatory proteins. On comparison, tongue carcinoma showed a significant down-expression of p16 and p21. In combined analysis, simultaneous down-regulation of p16 and p21 was seen in 47% of tongue cancer cases as against 28% in buccal carcinoma (p = 0.004). It was concluded that tongue and buccal mucosa cancers represent divergent biological sub-entities with prognostic and therapeutic significance. Similarly, some authors compared telomerase expression in OSCC of the tongue and buccal mucosa. The majority (13 of 16, i.e. 81%) of tongue cancers exhibited weak or negative telomerase activity, irrespective of the stage of disease. Conversely, in OSCC of buccal mucosa, the majority (27 of 31) of tumours expressed various levels of telomerase activity (χ2 = 4.24; p < 0.05). 124
Conclusion
The current research and published data suggest that pTNM, tumour volume, DOI, surgical margin status, tumour budding, vascular and perineural invasion, medullary bone invasion, lymph node and distant metastasis to be the consistent, easy-to-assess and reliable core prognosticators in OSCC. The other parameters such as histopathological grading systems and LNR are lacking in their prognostic efficacy due to dearth of universal evaluation criteria. Hence, as evidenced in this review, a multitude of parameters are involved in the determination of prognosis of a patient, based on which apt management should be planned to reduce the patient morbidity and mortality rates. To conclude, it is of paramount importance to include the aforementioned prognosticators in histopathological reports for the prediction of clinical outcome and archiving of valued data for future analysis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.