
Abstract
Objectives:
Lip, oral cavity and oropharyngeal cancer (OCC-OPC) represents a significant global health burden. The epidemiology and prediction of future burden of these cancers in Oceania is reported along with a critical description of cancer registries in the region.
Methods:
Data are extracted from GLOBOCAN 2012 and from published literature, as well as from local cancer registries, where available.
Results:
In Oceania in 2012, GLOBOCAN estimates the age-standardized incidence rates per 100,000 per annum for OCC-OPC to be 12.6 and 5.9 for males and females, respectively. Age-standardized mortality rates are predicted to have been 4.0 per 100,000 for males and 2.2 per 100,000 for females. Papua New Guinea is recorded as having the highest incidence rate of OCC-OPC in the world. It is predicted that 6500 new cases of OCC-OPC will be diagnosed in Oceania overall by 2030, an almost 45% increase compared to the 2012 incidence.
Conclusion:
Future research and resource allocation is needed to establish or improve the quality of cancer registries in the island nations of Oceania. Prevention as a primary intervention should be promoted by local authorities to control the increasing burden of lip plus OCC-OPC in this region.
Introduction
The inaugural Global Oral Cancer Forum met in 2016, with the mission to build awareness of gaps and innovations across the oral cancer continuum by facilitating international partnerships. 1 A strong understanding of the epidemiology of oral cancer is essential to prevention and to improving access to services in the regions that need it most, and implementing programmes that close the gaps in appropriate healthcare provision between different regions.
Cancers of the lip, oral cavity and oropharynx (OCC-OPC) present a significant global health burden. It is estimated that in 2012, these cancers accounted for 442,000 new cases of cancer worldwide, with 242,000 deaths worldwide. 2,3 OCC-OPC is more common in men than women, with the majority of deaths attributable to this cancer occurring in less developed regions of the world. 2,4 The prognosis of OCC-OPC remains poor, especially when diagnosed late in the course of the disease.
Oceania is a heterogeneous region comprised of 10 countries, extending from Guam in the north to New Zealand in the south, the American coastline in the east and Australia in the west (Figure 1). According to the World Bank, half of the countries lie in the middle-income category, with the remainder in the high income. 5 Here, we report the burden of OCC-OPC in the Oceania region by examining the incidence of new diagnoses, mortality secondary to OCC-OPC and future predictions of OCC-OPC incidence and mortality in the region. The state of cancer registries in the region is also reported.

Map of Oceania (not to scale).
Materials and methods
Geographical definition and data sources
Data have been accessed from the GLOBOCAN 2012 database which is managed by the International Agency for Research on Cancer. 6 Included in the Oceania region (Figure 1) are Australia, Fiji, Guam, French Polynesia, New Caledonia, New Zealand, Papua New Guinea (PNG), Samoa, the Solomon Islands and Vanuatu. This definition includes all countries of ‘Oceania’ as defined by the World Health Organisation, 7 excluding countries with a population of less than 150,000 in 2015. 8
Where available, individual data have been ascertained from the published literature or respective national cancer registry (Table 1), where a registry exists.
Cancer registry data in countries of Oceania (GLOBOCAN 2012).

aDiffers from GLOBOCAN.
Anatomic sites
The Global Oral Cancer Forum focused on OCCs, including those arising from the lip (International Classification of Diseases (ICD) version-10 code C00), tongue (C01 and C02), gum (C03), floor of mouth (C04), palate (C05) and other/unspecified parts of the mouth. Where available, data were also included for the oropharynx (base of tongue (C01), soft palate (C05.1 and 5.2), tonsil (C09) and other parts of the oropharynx (C10)), salivary glands (C07 and C08) and other parts of the pharynx (C12 and C13). 1 This article presents the incidence of lip and oral cancer (C00-C08) and oropharyngeal cancers as defined by GLOBOCAN (C09-C10, tonsil and oropharyngeal cancer, and C12-C14, piriform fossa, hypopharyngeal and other and unspecified oral, lip and pharyngeal cancers). This grouping of lip, oral and oropharyngeal cancers excluding nasopharyngeal cancers and facial sinuses are herein termed OCC-OPC.
Statistical analysis
Key metrics include age-standardized (world standard population) rates (ASR) of incidence of new diagnoses and mortality rates per 100,000 population per annum (pa).
Results and discussion
Epidemiology of oral cancer
OCC-OPC was in the top 10 most diagnosed cancers in Oceania in 2012 (Table 2).
Estimated cancer incidence in Oceania (2012), all ages.

ASR: age-standardized rates; OCC-OPC: oral cavity and oropharyngeal cancer.
GLOBOCAN estimated new diagnoses of OCC-OPC in Oceania in 2012 at 4506 cases (Table 3). OCC-OPC presented more of a burden to males, the ASR per 100,000 pa for new diagnoses of OCC-OPC was 12.7 for males and 5.9 for females, representing a male:female ratio of 2.15:1.
Prevalence, incidence and mortality rates of lip, OCC-OPCs in Oceania (GLOBOCAN 2012).

OCC-OPC: oral cavity and oropharyngeal cancer; ASR: age-standardized rates.
In 2012, 1553 patients (3.0 per 100,000 ASR) are estimated to have died from OCC-OPC in Oceania (Table 3). The ASR for mortality secondary to OCC-OPC was 4 and 2.1 per 100,000 pa for males and females, respectively. The male:female ratio for ASR mortality due to OCC-OPC was 1.9:1, similar to the pattern observed for the incidence ratio.
The Oceania region is defined geographically, but culturally and economically it is a heterogeneous group of countries. Australia and New Zealand are not only close geographic neighbours but have similar cultural diversity and health systems. The ASR mortality for OCC-OPC in 2012 in Australia and New Zealand was 1.7 and 1.6 per 100,000 pa, respectively. This is in stark contrast to the mortality of 12.2 per 100,000 pa ASR for the remaining countries of Oceania. PNG is reported as having the highest ASR mortality rate attributable to OCC-OPC in the world in 2012, of 17.7 per 100,000.
In Oceania, the ASR incidence and mortality of lip and OCC is highest in the 75 and over age group, while oropharyngeal cancer was diagnosed most commonly and had the highest mortality in the 70–74 age group. The shift over the past decade or so to younger males developing OPC, largely due to HPV infections, is apparent in Australia and New Zealand, but not (yet) across the smaller nations of the region.
Projected burden of OCC-OPC by the year 2030
The number of new cases of OCC-OPC predicted to be diagnosed in Oceania by 2030 is 6500, an almost 45% increase compared to the 2012 incidence (Figure 2). This is similar to the projected worldwide increase. This is partly attributable to population growth.

Projected number of new cases of OCC-OPC in Oceania by 2030 compared to 2012.
PNG is reported as having the highest incidence of OCC-OPC in the Oceania region and in the world. Lip and OCC was the most commonly diagnosed cancer in PNG in 2012. It is predicted that by 2030, 1836 new cases of lip and OCCs and 141 cases of OPC will be diagnosed, almost doubling the burden of OCC-OPC in PNG compared to 2012.
Australia
Australian cancer incidence and mortality data are available for 2013 and 2014, respectively. 9 These cancer registry data are readily available online. There were 3644 incidences of OCC-OPC in 2013, with 766 deaths due to OCC-OPC in 2014. The highest incidence of OCC-OPC was for lip cancer, ASR 4.2 per 100,000 followed by tongue cancer, ASR 3.2 per 100,000 population (Table 4). Tongue cancer was responsible for the greatest mortality, at 0.8 per 100,000 population. Men are more likely than women to be diagnosed with head and neck cancer in Australia. 9
The number and ASR of incidence of lip, mouth and tongue cancers in Australia (2013), adopted from Australian Institute of Health and Welfare database. 9
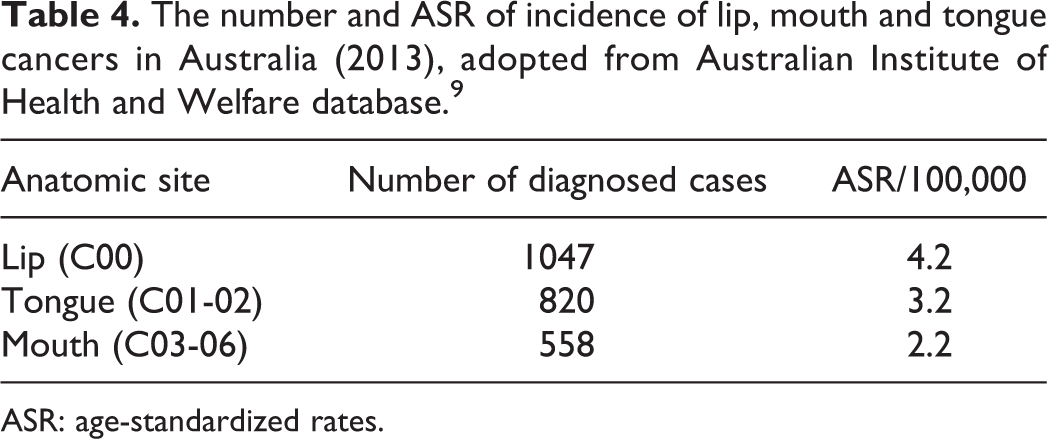
ASR: age-standardized rates.
The oral cancer mortality rate in Australia remains relatively unchanged over the last three decades, despite a drop in the incidence of new diagnoses. 10 This decline is a direct function of the drop in the incidence of lip cancers, which is thought to be secondary to individuals employing increased sun protection. 10,11 The incidence of tongue and oropharyngeal cancers is increasing as exposure to oral human papilloma virus (HPV) increases. 10,11 A meta-analysis reviewing HPV in the Asia-Pacific region noted 49.2% of included cases of oropharyngeal squamous cell carcinoma (SCC) were associated with HPV. 12 The rate of association of HPV with oropharyngeal SCC in the Oceania region as a whole was similar to Australia. 12 Interestingly, the incidence of tongue and oropharyngeal cancers increased while tobacco smoking in Australia continues to decline, as it has over the last two decades. 13 The number of OCC-OPC cancers diagnosed at a late stage has declined in Australia, with a 2016 study reporting 70% of patients presented with either T1 or T2 tumours, compared with 49% reported in a 1992 study. 14 There remain significant gaps in the understanding of oral cancer in Aboriginal Australians. The incidence of head and neck cancer is significantly higher in Aboriginal Australian men and women in the Northern Territory, and men only in Western Australia and Queensland. 15 In Queensland, the standardized incidence ratio for the period 1997–2012 for Aboriginal Australians for base of tongue, tonsil and oropharyngeal cancers was 2.16 (n = 81), and for mouth/OCCs was 1.53 (n = 74). 16
New Zealand
New Zealand Cancer Registry data are available online for 2013. 17 In 2013, there were 258 new diagnoses of OCC-OPC, with 80 deaths attributed to OCC-OPC. The highest rate of diagnosis was 1.6 per 100,000 for tonsil, followed by tongue (excluding base of tongue) at 1.5 per 100,000. Like Australia, oral tongue cancer was responsible for the greatest number of deaths attributable to OCC-OPC.
Chelimo and Elwood report that during the period 1981–2010, rates of OPCs-OCCs plus nasopharynx had risen. 18 Overall, Māori had higher oropharyngeal cancer rates than European/other ethnicities, but lower lip and oral cavity rates. 18 A marked increase was noted in oropharyngeal SCC occurring primarily in men aged ≥40 years. 18 Oral HPV infection has been implicated as a risk factor for oropharyngeal SCC. Since 2008, girls have been vaccinated against HPV in New Zealand. 19 The opportunity exists to extend this programme to include boys, as Australia has done.
Papua New Guinea
A cancer registry was established in PNG in 1958, originally the ‘Territory Tumour Registry’. 20 Initially, there were published cancer reports but this is no longer occurring. In 2010, Crouch-Chivers reported the existence of a cancer registry in PNG, describing it as a ‘cumbersome, paper-based system’ and ‘the prospects of any meaningful epidemiological research on these data, in its current form, seem slim’. 20 Attempts by one of the authors (CSF) to access data from the registry were unsuccessful, as were attempts to assist with computerization of the existing paper records by another author (NWJ). The Union for International Cancer Control reports the Papua New Guinea Cancer Centre is developing a cancer registry. 21 The GLOBOCAN database clearly states that the PNG data are extrapolated from rates in Fiji and the Solomon Islands, an ethnic mix quite different from PNG. Further, the remoteness of much of PNG means that cases may never be recorded, or even detected, making many cases unrecorded, even on paper. Mortality rates are likely to be even less complete because deaths in remote communities may not be registered accurately.
Oral cancer is reported to be the most prevalent neoplasm in PNG. 22 The high incidence of oral cancer in PNG has been reported for over half a decade, with 18.1% of all cancers registered and reported in 1958–1962, the most common cancer reported in the time frame being oral cancers. 23 According to GLOBOCAN, PNG had the world’s highest incidence and mortality related to OCC-OPC in 2012. The incidence and mortality will nearly double by 2030 with high associated mortality. This burden is very high compared to the other small island nations of Oceania.
In an early report from the Tumour Cancer Registry reporting from 1970 through 1978, the relationship between a chewing substance (areca nut, the inflorescence of the Piper betel vine and added slaked lime) and oral cancer in PNG was reported as ‘controversial’. 24 In 2012, the International Agency for Research on Cancer declared areca (betel nut), with or without tobacco, to be a ‘group 1’ human carcinogen. 25 There are regional differences in the prevalence of betel nut chewing, ranging from 26.8% in the highlands population to 95.4% on the north coast of PNG. 26 Betel quid without tobacco has been demonstrated to be associated with the development of oral cancer in PNG, both in a case-control study and systematic review. 27
Small island nations of Oceania
There is generally a low incidence of OCC-OPC in the small island nations of Oceania. Given limited available data, it is hard to read significance into this.
The Fiji Cancer Registry was established in 1965 28 and has utilized electronic data storage since the mid-1980s. 29 Beginning in 2002, the Fiji Ministry of Health has worked closely with the Centre for Public Health Research of Massey University New Zealand to systematically update the registry, with the use of CanReg4. 30 The age-standardized cancer incidence per 100,000 persons per year from 2002 to 2005 for all cancers in Fiji was 126.3 (95% CI 125.7–126.9). 31
The General Cancer Registry of French Polynesia was established in 1985. 32 The most recent cancer report from the registry examined the cancer burden for the period 1990–1995. 33 In this report, ICD-9 codes were used, inclusive of cancers of the nasopharynx. During this period, the annual incidence of OCC-OPC plus nasopharynx per 100,000 (world standardized) among native females was 7.3, compared to 14.4 per 100,000 for native male French Polynesians. Female immigrants were less likely to have a diagnosis of OCC-OPC plus nasopharynx with an annual incidence of 1.8 per 100,000, whereas the incidence among immigrant men was higher than native male French Polynesians, at 20.7 cases per 100,000. GLOBOCAN incidence rates were projected based on incidence rates from 1998 to 2002 and mortality rates from 2003 to 2005 were projected to the 2012 population.
In 1999, legislature was passed that saw the Guam Cancer Registry (GCR) established. This was further aided via a partnership between the University of Hawaii Cancer Center and the University of Guam which attracted funding and enhanced the ability of the GCR to collect and record accurate data. The most recent report, available online, details cancer incidence and mortality between 2008 and 2012. 34 Both the cancer incidence and mortality rates have increased over the three reported time periods since 1998. Oral cancer was the ninth most commonly diagnosed cancer and the seventh most common cause of death in males during the period. The crude incidence compared to the 2010 population was 4.14 new diagnoses per 100,000 persons pa, adjusted to WHO standardized population of 3.09 per 100,000. The Chamorro ethnic group are more likely than any other ethnic group in Guam to die from cancers of the mouth and pharynx.
New Caledonia’s Cancer Registry was established in 1977. 35 GLOBOCAN incidence and mortality figures were projected based on 2008–2010 rates.
The most recent known cancer data for Samoa were recorded in 1988. 29 A single pathologist collected all available data for patients treated 1963–1988, with only 1980–1988 included in the analysis given the incompleteness of the earlier years’ data. Histological confirmation of recorded cases of cancer was performed in 62.5% of cases. The age-standardized incidence rate of tongue cancer was 0.8 per 100,000 pa, mouth (gum, floor of mouth, other parts of mouth) 1.4 per 100,000 pa and oropharynx 0.4 per 100,000 pa. We believe this underestimates incidence rates given the likely incomplete registration of cases and deems mortality data ‘useless’ given incomplete death certificates. Cancer secondary to tobacco smoking was lower than surrounding nations, but in 1988 was predicted to change due to the recent establishment of a cigarette factory on the island.
In 1982, an analysis of pathology reports from 1970 to 1982 at the Central Hospital, Honiara in the Solomon Islands notes oral cancer to be one of the most common cancers in males, with OCC-OPC (including nasopharyngeal tumours) accounting for 9% of all cancers in males over the time period. 36 The most common OCC-OPC in the population was tongue cancer, with 25 cases reported. 36 Forty-two OCC-OPC cancers were recorded in the time period; 10 lip cancers, 25 cancers of the tongue, gum, floor of mouth and other/unspecified parts of the mouth and 7 cancers of the salivary glands.
A retrospective analysis of hospital separations, death certificates and data collected from community health facilities in Vanuatu revealed ‘neoplasms’ accounted for 13% of deaths in males aged 15–59, and 13% in females aged 15–59 over the period 2000–2007. 37 GLOBOCAN incidence rates were estimated based on 1999–2003 rates, while mortality rates were estimated from estimated national incidence for 2012.
Limitations and future efforts
Australia, New Zealand, Fiji, French Polynesia, Guam and New Caledonia have active cancer registries, with Australia and New Zealand registry data available online. Australian, New Zealand and Fiji Cancer Registries are coded in accordance with ICD-10 codes (see Table 1).
Australia and New Zealand have very high-quality data available on both the incidence and mortality of OCC-OPC. There are very high rates of case confirmation, including histopathologic confirmation of cancers. The data are representative of the population and there is 100% coverage of the population for mortality data.
This is in stark contrast to the rest of Oceania. The Solomon Islands and PNG have no incidence data available, whereas the remaining countries of Oceania only have cancer incidence rates available. Aside from Australia and New Zealand, mortality data are at best low quality (as defined by Mathers et al. 38 ), with no mortality data available for PNG, Samoa, the Solomon Islands or Vanuatu.
The nature of epidemiological studies relies on grouping of data in published sources, for example, GLOBOCAN. Ideally, lip, OCC and OPC would be examined together. Given the aforementioned GLOBOCAN groupings, tongue and salivary gland cancers have been considered with lip and OCCs, which is not a traditional or pathophysiological grouping. Hypopharyngeal cancers have been reported along with tonsil and OPC, cancers of the piriform fossa and other and unspecified oral, lip and pharyngeal cancers, again this has been done in accordance with the GLOBOCAN groupings but does not lend itself to a natural grouping according to the behaviour of these heterogeneous entities.
Data derived from GLOBOCAN are estimates, and the accuracy of derived figures will never reach that of a robust cancer registry. Given the limitations of the existence and quality of cancer registries in some countries of Oceania, GLOBOCAN provides a useful epidemiological snapshot of the burden of OCC-OPC.
Future implications
Primary prevention through cessation of tobacco use, areca nut (betel) use and HPV vaccination holds the greatest potential for OCC-OPC prevention in Oceania. In addition, improved methods for secondary prevention by screening and early detection have the potential for improving outcomes for patients with oral cavity and pharynx cancers.
There exists a significant gap in the current assessment of Aboriginal Australian-specific data, given the small numbers held at each of the state registries, and there is a significant opportunity to improve the quality of such data.
According to GLOBOCAN, PNG has the highest rates of lip, OCC-OPCs in the world. However, as mentioned above, the data are extrapolated from the Solomon Islands (where the large majority of the population are of Melanesian ethnicity, similar to PNG) and from Fiji (which is predominantly Polynesian, with a large ethnic Indian minority). The aetiology and pathogenesis of OCC-OPC cancer in PNG is clearly related to heavy areca nut use, but the roles of other risk factors remain largely unknown. Given the high incidence rates in PNG, education and mass screening campaigns are urgently required. Government bans controlling the distribution of areca nut and its use in public places have been discussed, ironically because of littering and staining pavements with expectorated red ‘betel juice’.
PNG and the small island nations in Oceania face similar issues to South East Asian countries. These issues are addressed in a separate paper outlining data to the Global Oral Cancer Forum about the burden of OCC-OPC in South East Asia, recently published in this journal. 39
Globally, the projected increase in the incidence of OCC-OPC in developing countries is set to put significant pressure on these countries who are typically ill-equipped to deal with the burden this will place on their healthcare infrastructure and limited resources. 40,41
Conclusions
The Oceania region contains PNG, which is reported to have the highest burden of OCC-OPC worldwide, with significant projected increases in the incidence and mortality of OCC-OPC by 2030. There is an urgent need for the establishment of robust cancer registries in PNG, Samoa, the Solomon Islands and Vanuatu and the provision of resources to tackle this significant health burden. In addition to the collection of sound epidemiological data, primary and secondary prevention strategies provide the most significant opportunity to reduce the burden of OCC-OPC, not only in Oceania, but also worldwide. 42
There is a need to improve the quality of epidemiological data in the small island nations of Oceania through the use of cancer registries, to better quantify the burden of OCC-OPC in this part of the world. In 2014, the International Agency for Research on Cancer announced plans to establish an IARC Regional Hub in the Pacific Islands. The Pacific Islands Regional Hub will ‘focus on supporting cancer registries and improving data collection and data utilisation’ for cancer control in all Oceanic nations, excluding Australia and New Zealand. 43 Fundraising is currently underway to initiate a mutually agreed plan for the hub.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Global Oral Cancer Forum was fully funded by The Henry Schein Cares Foundation.