
Abstract
Objectives:
To document the burden of oral cancer in South East Asia (SEA) and to examine the gaps in acquiring accurate data within these countries.
Methods:
Epidemiological data on oral cancer from countries in SEA were obtained and reviewed from public population-based databases. Descriptions on the incidence and mortality of oral cancer were based on data obtained from GLOBOCAN 2012, and prediction of the number of cases and deaths due to oral cancer were also taken from the same database. The availability of and accessibility to population-based cancer registry were also documented.
Results:
Five of the eleven countries in SEA have national cancer registries, but the reporting periods varied from 2002 to 2014 across these countries. Whilst incidence and mortality data were obtainable for all SEA countries from GLOBOCAN 2012, data quality varied substantially across the countries. Estimated incidences of oral cancer ranged from 1.6 to 8.6/100,000 per annum with similar rates in males and females for most countries. The incidence was the highest in Myanmar and Brunei for males and females, respectively. Mortality due to oral cancer was reported to be 0.4 to 5.3/100,000, with the highest mortality in Myanmar and Timor-Leste among males and females, respectively. Based on the predicted number of cases and deaths for 2020, oral cancer incidence and mortality is expected to increase and the trends are similar between males and females, which is not surprising as with population growth, the disease burden will rise further.
Conclusion:
This study demonstrates a severe lack of accurate epidemiological data on oral cancer and underscores the urgent need to develop expertise within this region that can address this issue. While there is a clear need for improved primary prevention, for increased skilled workforce and for improved diagnostic and treatment facilities, an essential first step is to establish robust cancer registries so that progress or lack thereof can be monitored accurately, and appropriate action planned.
Introduction
Globally, oral cancers (ICD, 10th edition C00-08) accounted for 300,373 new cancer cases and 145,353 cancer deaths in 2012. 1 More than half of oral cancers in the world occur in Asia where an estimated 168,850 new cases were diagnosed in this geographical region alone. Of these, approximately 11% were from South East Asia (SEA; comprising 11 countries as defined by United Nations; Figure 1 and Table 1) where the incidence of oral cancer has been regarded as disturbingly high for many years. 5 Globally, while oral cancer is predominantly diagnosed among males, it can be as common or even more common in females than in males, in many SEA populations. 1,6 The mortality to incidence ratio in SEA is among the highest in Asia, 7,8 and in 2012, the mortality due to oral cancer in SEA has been estimated as 8508 cases, where 5014 and 3494 were men and women, respectively (Table 2) 1 ; however, because cause-specific recording of mortality is poor in most countries in SEA, the numbers here are likely under-reported.
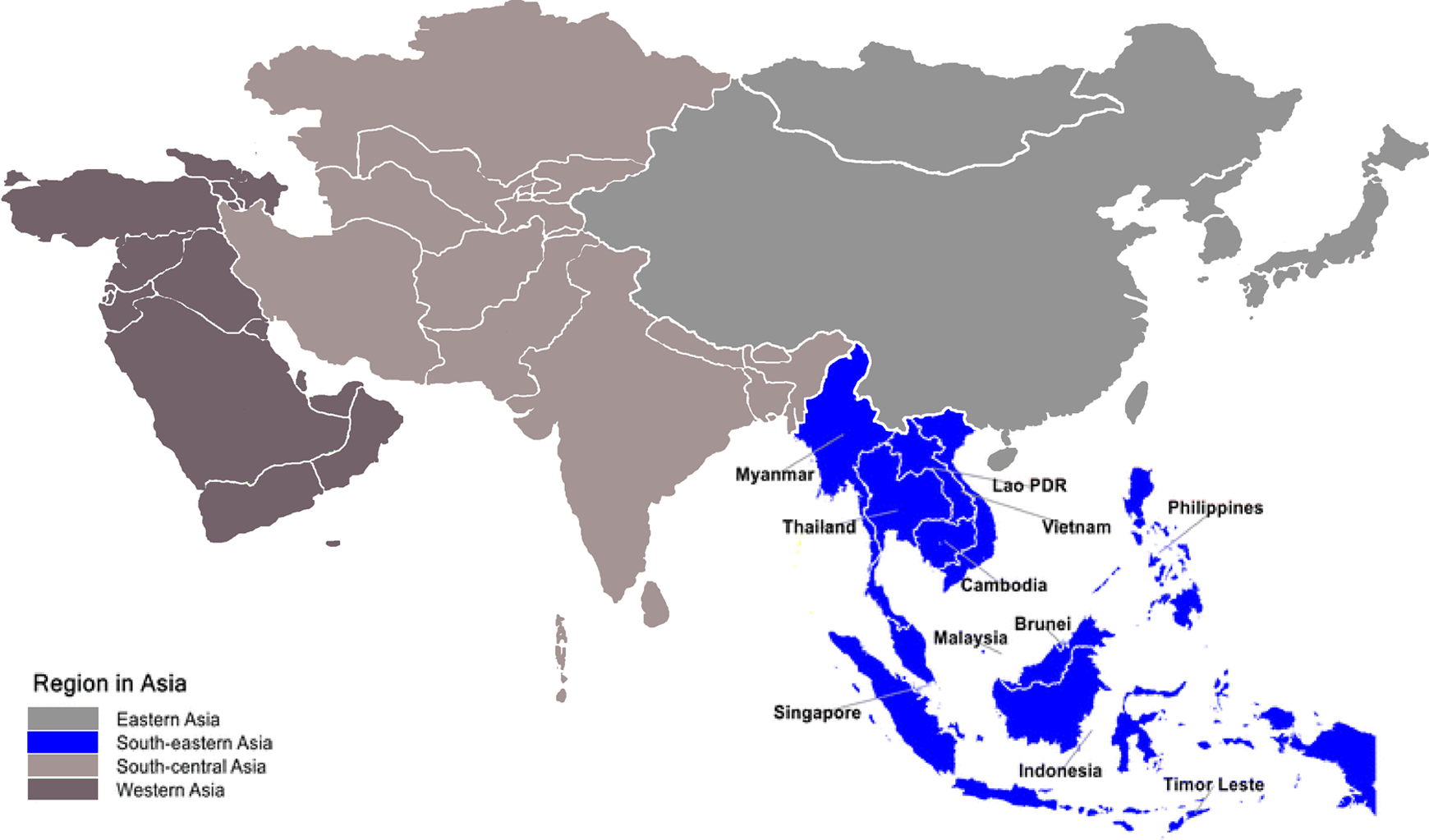
Sub-regions within Asia as defined by the United Nation. Countries highlighted in blue are those included within South East Asia.
Status of cancer registries in countries in SEA.

NA: not available; not known: data is not accessible.
aIncidence data source: A. High quality × national data or high-quality regional (coverage greater than 50%); B. High quality × regional (coverage between 10% and 50%); C. High quality × regional (coverage lower than 10%); D. National data (rates); E. Regional data (rates); F. Frequency data; G. No data.
bMortality data source: National statistics are collated and made available by the WHO for countries with vital registration. 1, High quality × complete vital registration; 2, medium quality × complete vital registration; 3, low quality × complete vital registration; 4, incomplete or sample vital registration; 5, other sources (cancer registries, verbal autopsy surveys, etc.); 6, no data.
Oral cancer incidence and mortality in SEA countries in 2012.

SEA: South East Asia; ASR: age-standard rate.
Globally, the most common risk habit associated with oral cancer is the use of tobacco, both smoked and smokeless, the latter often in combination with areca nut in numerous forms. Demographics and health surveys report that tobacco use in all countries of SEA exceeded 50% among men aged 15–49, 9 and some of these countries, notably Indonesia and Timor-Leste, are among those with the highest smoking rates among males in the world, where more than 70% of men smoke (72.3% and 96.5%, respectively). 10,11 Among the populations within the SEA region, the use of smokeless tobacco is very high, where, for example, in Myanmar, more than 50% of the male population indulge. 12 In contrast to smoking, where rates remain relatively low among women in SEA, the highest use of smokeless tobacco among women globally is in South and SEA. 11,13 In South and SEA, smokeless tobacco is often used as one of the ingredients of betel quid, a mixture of substances that contain areca nut (the fourth most consumed psychoactive substance in the world), slaked lime and other condiments. 14 The chewing of betel quid is practised by more than 600 million people (approximately 10% of the world’s population), many of whom reside in the geographical areas of South and SEA. 15,16 Wrapped in a betel leaf, the betel quid is often kept in contact with the oral mucosa for extended periods, even overnight. 17 As areca nut itself is a carcinogen, 18 the use of betel quid with or without smokeless tobacco is highly associated with oral potentially malignant disorders and oral cancer of the population in this region. 19,20 In a recent prevalence study in Cambodia, 19.7% of women were found to indulge in betel quid chewing and this was the strongest risk factor associated with oral potentially malignant disorders with a relative risk of 6.7. 21
There are huge disparities in the percentage of population covered by population-based registries between high- and low-income countries. While a large proportion of the population is covered by population-based cancer registries in Europe (42%), Oceania (78%) and North America (95%), only about 6% of the entire Asian population is covered. 1,2 Therefore, the true burden of oral cancer in this region is unknown and almost certainly significantly underestimated, and in SEA countries, many lack efficient methods of storing and disseminating information that are necessary to understand patterns in incidence and mortality associated with this disease. Therefore, the aim of this study was to document the burden of oral cancer in SEA through the review of current available data and to examine the gaps in acquiring accurate data within these countries. In addition, we discuss the challenges that are associated with the management of oral cancer and discuss possible collective approaches that will be important for countries within this region to take forward, in order to progress towards improving oral cancer prevention, management and survival.
Materials and methods
Epidemiological data on oral cancer from countries in SEA were obtained and reviewed from several sources including the population-based data from the public databases of Cancer Incidence in Five Continents (CI5 Vols IX and X) 2,3 and GLOBOCAN 2012 (http://globocan.iarc.fr/). 1 Further, data from cancer registries were reviewed for the individual countries where available, and for countries where the data are not accessible, the authors contacted head and neck cancer surgeons in the respective countries where possible, to determine the availability of data. Having reviewed these, data from GLOBOCAN 2012 were found to be the most comprehensive; therefore, detailed descriptions of the incidence and mortality due to oral cancer in SEA are derived therefrom. Age-standard rates (ASR) against the world standard population were used. Furthermore, prediction of the number of cases and deaths due to oral cancer was also obtained from GLOBOCAN 2012.
Results
Of the 11 countries within the SEA region, Singapore, Thailand, Philippines, Vietnam and Malaysia are the only countries that have population-based cancer registries. Reports from Singapore and Thailand’s registries were the most up-to-date with the last report dated 2015, with reporting periods till 2014 and 2012, respectively. 22,23 The most recent reports for Malaysia and the Philippines were in 2011 and 2008, with reporting periods up to 2007 and 2002, respectively. 24,25 Data on Vietnam were not accessible and, therefore, the last reporting period is not known. Looking at data on oral cancer specifically, these data were available from the Thailand, Philippines and Malaysia registries in the last reporting periods, the latest data for Singapore were not available and data on oral cancer were last reported for 2003–2007 (Table 1). As the majority of the SEA countries do not have national registries and only a minority contributed data to the CI5 Vols IX and X (Table 1), we relied on data from GLOBOCAN 2012 which appeared to be the most comprehensive for all countries within SEA. 1
Data quality in GLOBOCAN 2012 varied substantially across the different SEA countries with Singapore, Thailand and the Philippines having high-quality national or regional coverage of more than 10% (Table 1). Notably, while we look at the incidence of oral cancer across the world, three of the SEA countries were among the top 20 countries with the highest incidence of oral cancer, including Myanmar, Brunei and Cambodia for both genders. Among females, Brunei, Timor-Leste, Cambodia, Lao PDR and Myanmar were the countries with the highest incidence of oral cancer (Figure 2) with ASRs of up to 9.0/100,000. Focusing on the data for SEA countries more closely, 10,517 males and 7554 females were diagnosed with oral cancer in SEA per year, with a male-to-female ratio of 1.4:1. There is a marked variation in the ASR across the different countries in SEA ranging from 2.5 to 8.6/100,000 per annum for males, with Myanmar having the highest incidence; and 1.6–9.0/100,000 per annum for females, with Brunei being the highest (Table 2 and Figure 3). While in most countries oral cancer is more commonly diagnosed among males, there appears to be a predilection towards females in Brunei and Lao PDR, with ASR almost doubling that of males (Figure 3). Based on the estimated deaths due to oral cancer, a wide range is observed across the different countries in SEA. Among males, the mortality rates were 1.1–5.3/100,000 per annum, with Myanmar having the highest rates. Among females, the ASR were 0.4–3.4/100,000 per annum, with Timor-Leste having the highest mortality rates. Consistent with the higher incidence in Brunei and Lao PDR among females, the mortality rates due to oral cancer were also higher among females in these countries compared to males (Table 2 and Figure 3).

Incidence and mortality of oral cancer across the world for males (a), females (b) and overall (c). Several SEA countries were among the top 20 countries with the highest incidence of oral cancer (*).

Incidence (a) and mortality (b) of oral cancer across the countries in SEA in males and females.
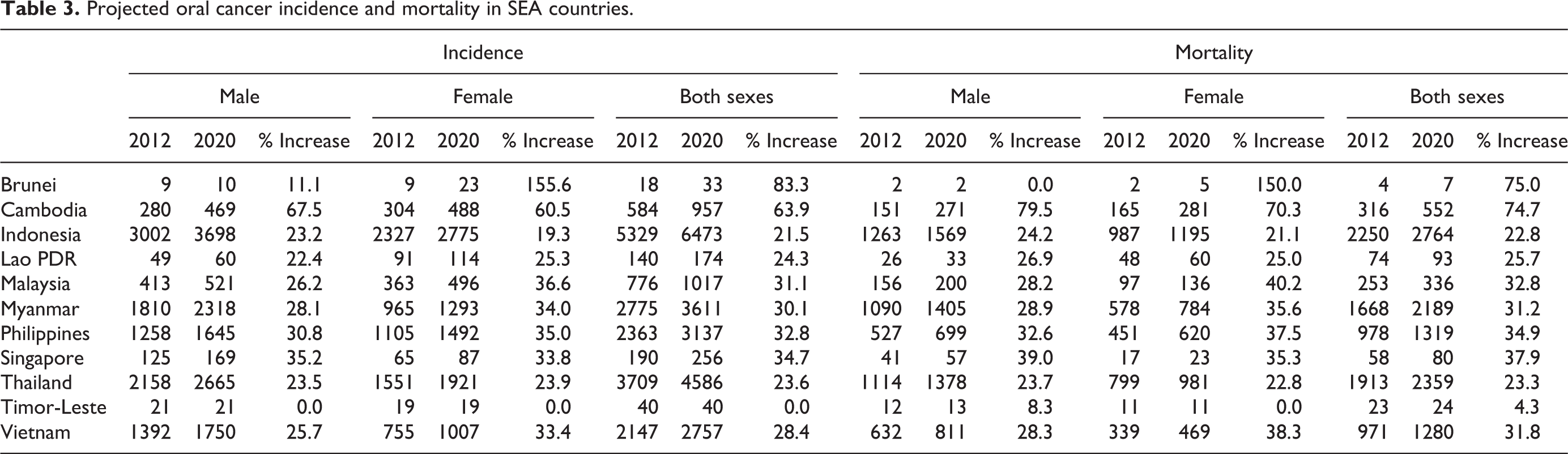
We also examined the predicted incidence and mortality trends in GLOBOCAN 2012 for 2020. Comparing the incidence and mortality projected in 2020 to those reported in 2012, the data suggest that oral cancer incidence would continue to rise in every one of the SEA countries, with increases of up to 83.3% and 63.9% by 2020 in Brunei and Cambodia, respectively (Table 3). Consistently, the mortality rates are also predicted to increase in all SEA countries, again with Brunei and Cambodia predicted to have the steepest increase of up to 75.0%. These trends are consistent across both sexes with similar rates of increase (Table 3).
Projected oral cancer incidence and mortality in SEA countries.
Discussion
This study examined the status of cancer registries, the incidence and mortality due to oral cancer in countries within SEA, with the aim to provide evidence that there is an urgent need to prioritize resources to put in place structured programs that would benefit the region to reduce oral cancer burden here. While this report discusses the extent of the oral cancer burden in SEA, the main limitation is the lack of systematic documentation of the disease, where most of the countries in SEA do not have an official cancer registry. 4 While the data were available for all SEA countries from GLOBOCAN 2012, many were either obtained from regional registries or estimated from rates of neighbouring countries and, therefore, may not be entirely representative of the respective countries. This is perhaps not surprising as only 2% of Asia’s population is covered by population-based registries and, subsequently, coverage in GLOBCAN for Asia is sparse. 1 This is not to say that epidemiological studies are not conducted in SEA countries: in fact, in many of the countries, regional or hospital-based cancer registries exist, 26–28 while for other countries such as Lao PDR, wider data collection has recently been initiated (see below). It is evident that data collection in many of the SEA countries is very much driven by a bottom-up approach and largely supported through external regional and/or international collaborations. 29–31 Without the presence of robust population-based cancer registries, data on the mortality due to cancer are also difficult to ascertain. Furthermore, many SEA countries do not have comprehensive death registration systems and even when such a system exists, the quality of the cause of death information is very often poor. 7 Political conflicts, internally displaced persons and struggles with weak economies compound the challenges in data collection. Development of robust population-based registries will require strong support from governments as this relies heavily on strong networks with flow of accurate information among public and private healthcare service units, registries of births and deaths, and population census data. While cancer registries in lower resource settings may find it difficult to match the strict criteria of a quality data set for inclusion into international databases such as CI5, population-based registries are critical to cancer control and therefore should remain a priority. Recognizing the critical need for regional and national support, the International Agency for Research on Cancer (IARC) has developed regional hubs through the Global Initiative for Cancer Registry Development to empower low- and middle-income countries to produce high-quality information on the burden of cancer through educational support and collaborative research. In 2011, a hub for Asia was launched in the Tata Memorial Hospital in Mumbai, India. While it is currently unclear how and whether or not this initiative will impact countries in SEA, one approach by which SEA countries can improve the state of cancer registries is through regional collaborations. Meetings to set up an Asian Network on Cancer Registries were held in Korea in 2008 and Thailand in 2009 with objectives to include training for standardization of records, networking, planning and execution of collaborative research and evaluation of cancer control and treatment outcomes. Encouragingly, the National Cancer Institute of Thailand have collaborated with the International Agency for Cancer Registries (IACR) to help the Association of South East Asian Nations (ASEAN) countries, including Lao PDR, Myanmar, Cambodia, Malaysia and Indonesia, to provide training that will enhance their capacity to develop or strengthen their population-based cancer registries. Notably, this collaborative effort has led to the initiative to document oral cancer cases in Lao PDR (Patravoot Vatanasapt, personal communication, 18 October 2016), but more efforts in regional and global support should be strongly encouraged and systematically facilitated.
Decreasing trends of oral cancer have been reported in Singapore, Thailand and Philippines, while 32–34 from GLOBOCAN 2012, it appears that both incidence and mortality of oral cancer will continue to increase. The data from the cancer registry from Khon Kaen, Thailand, also showed an increasing trend of oral cancer, especially among females. 6 Some of these apparent discrepancies could be due to regional differences within countries, for example, while oral cancer cases are reportedly declining in Chiang Mai in the north of Thailand, the rates are increasing in north-eastern Thailand in Khon Kaen. 6,34 The overall increase in incidence and mortality due to oral cancer is perhaps not surprising as the use of tobacco, both smoked and smokeless, is high in SEA countries. SEA countries including Indonesia, Vietnam and Timor-Leste are among the top consumers of cigarettes. 9,10 Among females in SEA countries, Lao PDR and Brunei have the highest percentage of women smokers (11.4% and 8.4%, respectively), 10 and this could in part explain the high incidence rates among females in these countries, and this observation should be studied more carefully for effective cancer control planning. The rampant use of tobacco both smoked and smokeless is attributed primarily by the fact that the tobacco industry and tobacco marketing are not regulated well in most of SEA even though all of these countries, apart from Indonesia, have signed the World Health Organization’s Framework Convention of Tobacco Control and direct advertising is supposedly banned in Brunei, Cambodia, Lao PDR, Malaysia, Philippines, Singapore and Thailand. 35,36 In fact with the tobacco industry contributing significantly to the economics of the country, conflict of interest in the revenue taxes generated from the tobacco industry must be consciously examined in accordance with guidelines stipulated in Article 5.3. Betel quid chewing which is also closely linked with oral cancer and widely practiced in SEA countries compounds the issue of tobacco control. 24,28,37–39 In some areas, for example in the north-eastern region of Thailand, betel quid chewing is the strongest risk factor for oral cancer with odds ratio of 9.01, and the habit continues to be popular among youths. 19,20,28,38,40 The betel quid chewing habit is practised both among the men and women and therefore, in contrast to many other parts of the world where there is a preponderance of oral cancer among males, the number of oral cancer diagnosed in women rival that in the men and this is in major part because of the betel quid chewing habit that is also widely practiced among the women. 41,42 While efforts to control the use of betel quid have been somewhat successful in India, there are currently no regulations in place to control betel quid chewing within any SEA country and educational programmes to highlight the risks are limited or non-existent. Although emerging studies in some pockets of society indicate that betel quid use may be on the decline, 30,43 we must not be complacent as large migratory waves across SEA have occurred in recent years, and such habits could be reintroduced into the host countries resulting in future increase in oral cancer risk. For example, while betel quid chewing was commonly observed in rubber estates among the Indian population 2–3 decades ago in Malaysia, this habit is prevalent in the cities at present time, albeit among migrant communities (authors’ observations).
With the challenges outlined for all the SEA countries in this study, it is apparent that many have overlapping issues which could be more effectively addressed if there is committed collaboration within the region. As the SEA countries come together as the ASEAN, this affords an opportunity to address some of these issues under the objectives of ASEAN to promote active collaboration and mutual assistance on matters of common interest including those pertaining to social, technical and scientific fields and to provide assistance to each other in the form of training and research facilities in the educational, professional, technical and administrative spheres. The importance of oral cancer was underscored in a recent publication on the burden of cancer on member countries where oral cancer was reported to be the fifth most common cancer among ASEAN member countries contributing to 50% of all new cancer cases. 44 Furthermore, the need for programmes that would promote prevention and early detection of oral cancer was highlighted at a 2013 Chief Dental Officers’ meeting among ASEAN countries in Chiang Mai. Such collaborations within ASEAN are emerging 45 and an opportunity to form an organization for Asian co-operation on cancer registration could be the next step forward so that collaborative and comparative epidemiological studies across the different countries can be conducted. Clear guidelines were put forward within the Resolution of the WHO Regional Committee for SEA and further discussed under the Disease Control Priorities in Developing countries. 46 To address these, several other challenges urgently need addressing in relation to the development of robust cancer registries. There is an urgent need to build human resource capacities in epidemiology and medical sciences to provide global standards of reporting. The need for basic and specialised training is real and critical to improve diagnosis and treatment of oral cancer in SEA countries. Data on oral cancer should be based on histologically confirmed cases, which are currently not possible without adequately trained specialists in some of these countries. As previously suggested, global and perhaps more practically, regional collaborations could be a way forward in developing expertise to address these issues. While much of this requires commitment from the respective governments, assistance to map a national cancer control plan from international governing bodies including the World Health Organization (WHO), IARC 15 , IACR and the Union for International Cancer Control would go a long way in addressing the challenges discussed in this study.
Footnotes
Authors’ Note
This study was presented in the Global Oral Cancer Forum (GOCF) 2016 held in New York, USA, in March 2016. We are committed to an understanding of cancer prevention, diagnosis and treatment through a fundamental research program.
Acknowledgements
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is funded by sponsors and donors of Cancer Research Malaysia. Cancer Research Malaysia is a non-profit research organization. The Global Oral Cancer Forum (GOCF) 2016 was funded by the Henry Schein Cares Foundation. SCC received financial support from the same foundation to present this data at the GOCF.