
Abstract
Objectives:
Oral cavity and oropharyngeal cancer (OCC-OPC) is a major health problem worldwide. The Middle East and North Africa (MENA) region is constituted of 23 countries, with a heterogeneous population of over 448 million people. This is the first review to report collectively on the epidemiology and etiology of OCC-OPC in the MENA region.
Methods:
Data are derived from GLOBOCAN 2012. We searched the published literature databases to report risk factors of oral cancer in the MENA region.
Results:
Age-standardized incidence rates per 100,000 per annum are estimated by GLOBOCAN 2012 for males and females and these were 2.6 and 1.8, respectively. The age-standardized mortality rates of OCC-OPC for males and females were 1.1 and 0.7, respectively. Importantly, the crude incidence and mortality rates are projected to double by 2030 especially in Egypt, Iran, Morocco, Sudan, and Turkey. This increase is double that of the projected worldwide rate.
Conclusion:
Local governments and international agencies should collaborate to improve the standard of clinical services, preventive measures, and public awareness of oral cancer. Future research should be undertaken to improve the quality of registry reporting data for OCC-OPC.
Introduction
Oral cavity and oropharyngeal cancer (OCC-OPC), as defined by the 10th edition of the International Classification of Diseases representing the rubrics C00 to C10 1 , is a global health burden with an estimated overall annual incidence of nearly 443,000 new cases and 241,450 deaths worldwide. 2,3 Most of the new OCC-OPC cases are diagnosed in the developing world. 4 Wide geographic variability is also observed in the incidence of constituent anatomic subsites. 4,5 Historically, the incidence of OCC-OPC has been highest in South and Southeast Asia, Western and Central Europe, and South America. 5,6 The inaugural Global Oral Cancer Forum (GOCF) took the initiative to address the regional disparity of oral cancer around the world. 7 The Middle East and North Africa (MENA) region is one of the cradles of civilization and urban culture and has had a volatile history. MENA is constituted of 23 states with a heterogeneous population of over 448 million people. Most MENA countries are ranked in the developing world with low- to middle-income states according to the World Bank. The incidence of cancer (all sites) in the MENA region is on the increase, and it is currently the fourth leading cause of death behind cardiovascular diseases, infectious and parasitic diseases, and trauma injuries. 8 More than 270,000 people are estimated to die of cancer each year in this region. Additionally, the World Health Organization (WHO) has predicted that the Eastern Mediterranean region (a larger definition of MENA that includes Afghanistan and Pakistan) will have the largest increase in cancer incidence among WHO regions in the next 15 years, with projection modeling predicting an increase of between 100% and 180%. 8
The burden of OCC-OPC in MENA, regarding incidence, mortality, survival, and the determinants of disease, is still not entirely acknowledged. Understanding this burden in a region characterized by critical resource issues and political turmoil could have important implications for policymaking, resource management, and most importantly prevention. Therefore, we aimed to report on the epidemiology and etiology of OCC-OPC and undertake future predictions in the MENA region.
Materials and methods
Geographic definition and data sources
We used data from the public database (GLOBOCAN 2012) that is maintained by the International Agency for Research on Cancer (IARC). 9 We included the following countries in the data analysis: Algeria, Bahrain, Djibouti, Egypt, Iran, Iraq, Israel, Jordan, Kuwait, Lebanon, Libya, Mauritania, Morocco, State of Palestine, Oman, Qatar, Saudi Arabia, Somalia, Sudan, Syria, Tunisia, United Arab Emirates, and Yemen (Figure 1). Data on Turkey were also included as it shares similar historical and cultural values of the vast majority of the MENA countries despite the fact that it is grouped within the WHO Europe region.

Map showing the countries of the MENA region that were included in this study (World Bank maps). MENA: Middle East and North Africa.
Anatomic sites
The GOCF specifically focused on cancers of the oral cavity, including those arising from the lip (International Classification of Diseases version-10 code C00), tongue (C01 and C02), gingiva (C03), floor of mouth (C04), palate (C05), and other/unspecified parts of the mouth (C06). Where available, data were also included for the oropharynx (base of tongue (C01), soft palate (C05.1 and C05.2), tonsil (C09), and other parts of the oropharynx (C10)) and salivary glands (C07 and C08). Cancers of the nasopharynx and hypopharynx were excluded from the current review as they have a distinctly different etiology and biology. Of note, published data on cancers of the tongue usually include the base of the tongue, which is better regarded as part of the oropharynx. It is part of Waldeyer’s ring where the associated lymphoid tissue and comparatively high prevalence of oncogenic human papillomavirus (HPVs) make it a distinct entity.
Statistical analyses
Key metrics of burden including age-standardized (world standard population) rates (ASR) of incidence and mortality per 100,000 population as well as the annual number of incident/new cases were included. Analyses were conducted both overall and stratified by sex.
Results and discussion
Epidemiology of oral cancer
Incidence and mortality rates
In the MENA region, the newly diagnosed cases of OCC-OPC were estimated in 2012 at around 8928, amounting to 1.5% of all human malignancies; however, the associated deaths were 3573 (1% of all human malignancies). OCC-OPCs rank among the top 20 cancers in the MENA region (Figure 2). New cases accounted for 5164 in males and 3764 in females. The male:female ratio for both incidence and mortality rates in the whole MENA region were 1.38:1 and 1.36:1, respectively. 9,10 Of note, the ASR incidence rates per 100,000 of OCC-OPC for males and females were 2.6 and 1.8, respectively, whereas the ASR mortality rates were 1.1 and 0.4, respectively (Table 1).
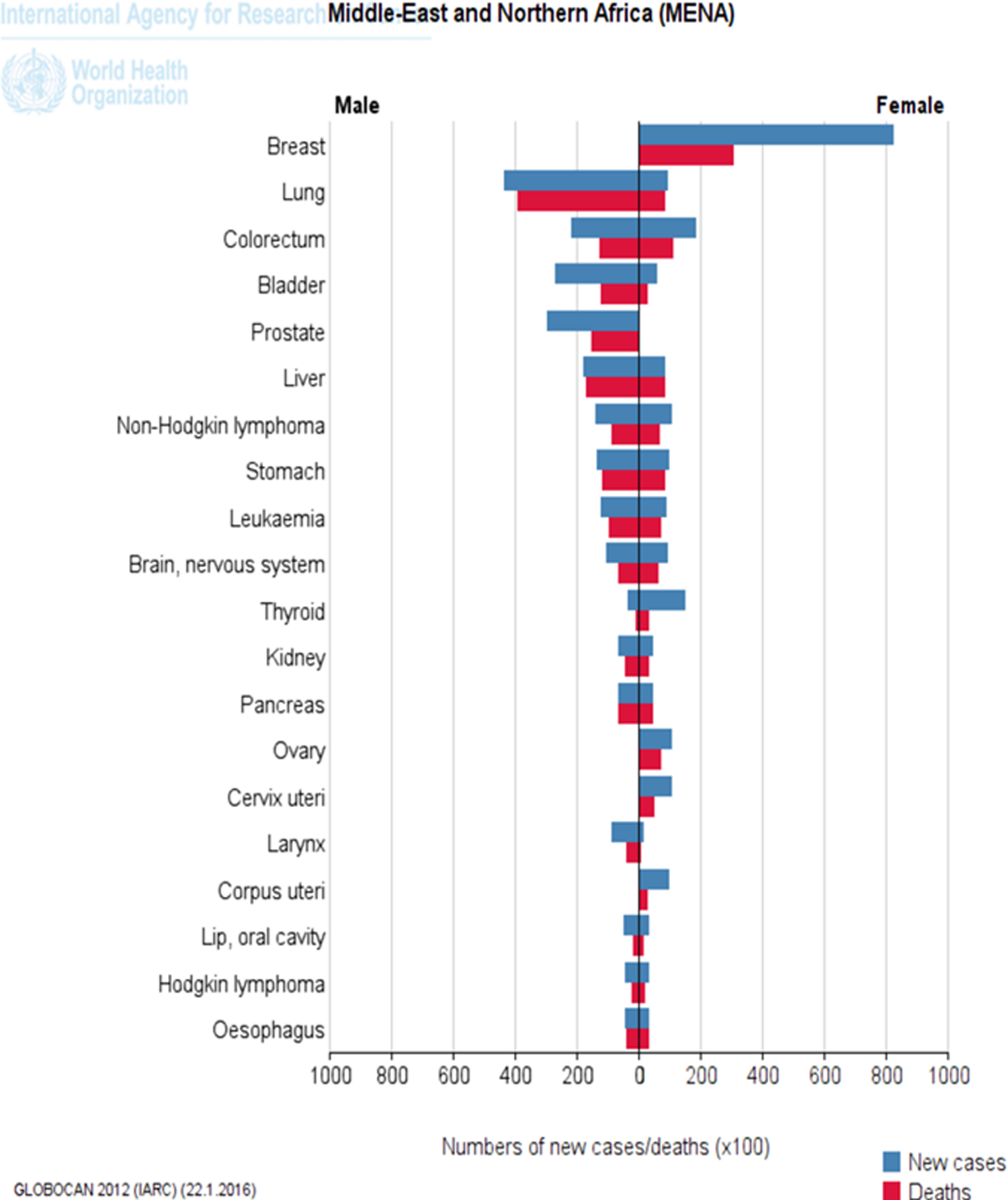
Top 20 malignancies in the MENA (GLOBOCAN 2012). 9 MENA: Middle East and North Africa.
Incidence and mortality rates of oral cavity and oropharyngeal cancer in the countries of MENA region (modified from GLOBOCAN 2012). 9
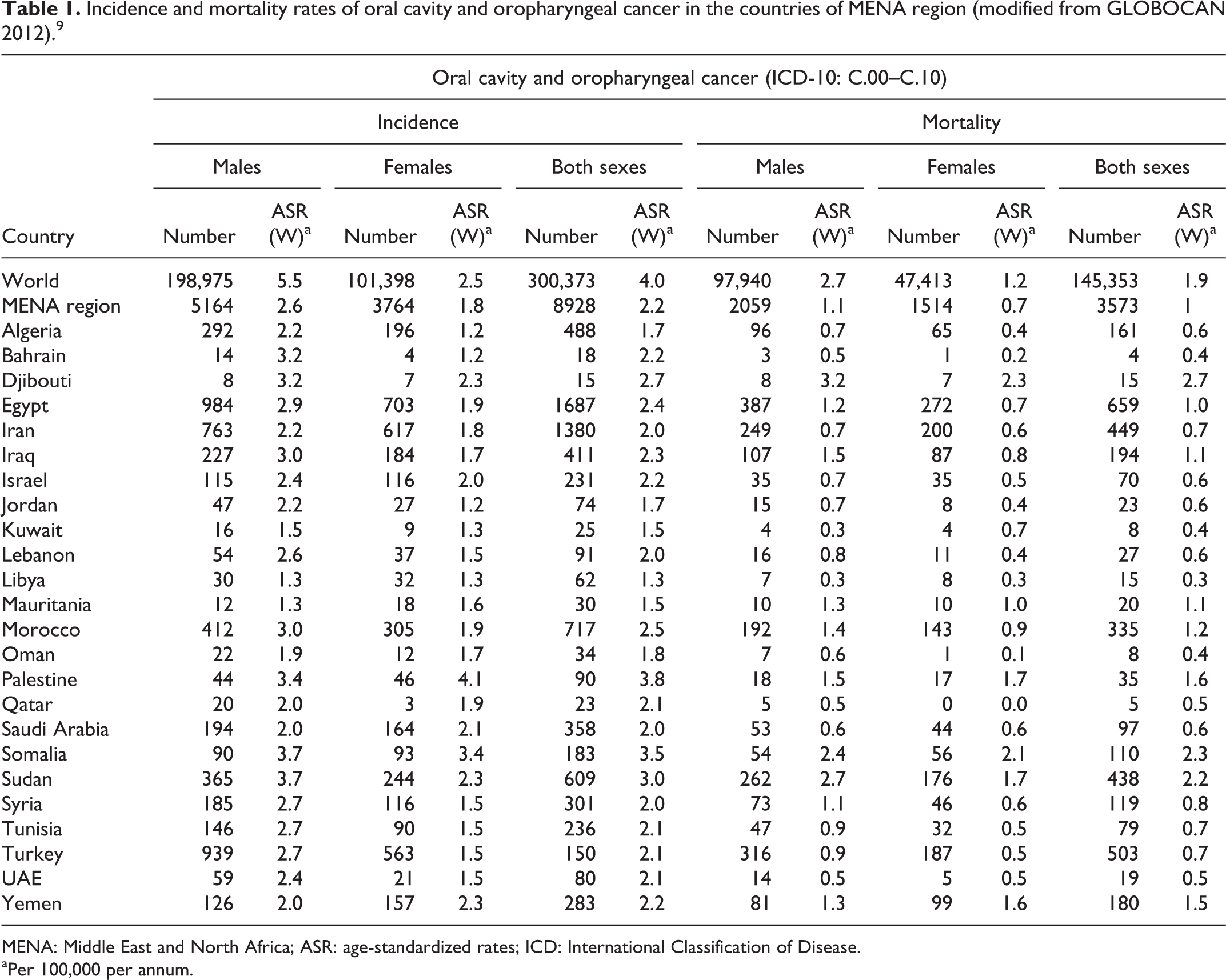
MENA: Middle East and North Africa; ASR: age-standardized rates; ICD: International Classification of Disease.
aPer 100,000 per annum.
Variation in the regional distribution of OCC-OPC has been documented (Table 1). Likewise, a discrepancy in the number of OCC-OPC-related deaths has been observed between several countries (Table 1). The top three ASR rates of incidence in both genders were found in the State of Palestine (3.8 per 100,000 per annum), Somalia (3.5), and Sudan (3.0). In contrast, the lowest incidence ASR for both genders was in Libya (1.3). Interestingly, the highest ASR rates of OCC-OPC-associated deaths were found in Djibouti (2.7) and Sudan (2.2), with the lowest found in Bahrain (0.4) and Libya (0.3).
Although this neoplasm occurs in various oral and oropharyngeal subsites, it is most common on the lower lip, lateral border of tongue, and floor of the mouth (Table 2). Notably, Turkey has the highest ASR incidence of lip cancer in males, whereas Israel has the highest ASR incidence of lip cancer in females.
Age standardized rate of incidence of oral cavity and oropharyngeal cancer in selected countries in the MENA by site grouping (per 100,000 per annum), modified from Cancer Incidence in Five Continents, Vol. X. Lyon: International Agency for Research on Cancer. 2

MENA: Middle East and North Africa; ASR: age-standardized rates.
In a similar fashion to worldwide trends, OCC-OPC in the MENA region is mainly a disease of middle-aged and elderly men, with a peak incidence in the sixth to eighth decades of life.
Unfortunately, there is no substantial documentation on the effect of ethnic background and whether this has an influence on the demographic variations regarding incidence, prevalence, stage at diagnosis, and mortality rate associated with OCC-OPC. Likewise, the influence of the cultural factors particularly the alcohol prohibition is not well documented.
Projected burden of OCC-OPC by the year 2030
Our projection analysis using the GLOBOCAN 2012 prediction shows that the number of estimated new cases of OCC-OPC in the MENA region will double by the year 2030. In contrast, the number of estimated new cases of OCC-OPC worldwide will only increase by 50% in the same timeframe. Similarly, our results demonstrate that the mortality rate is estimated to dramatically double by the year 2030, whereas the mortality rates of oral cancer worldwide will only increase by 50% (Table 3). These dramatic changes in the estimated incidence and mortality rates will be mostly observed in Egypt, Iran, Morocco, Sudan, and Turkey. This projected increase could be due to demographic changes in relation to population growth and in particular to increases in the number of individuals above 65 years of age.
Projected burden of ASR incidence and mortality of oral cavity and oropharyngeal cancer in countries of MENA region between 2012 and 2030 (per 100,000 per annum),a modified from GLOBOCAN 2012. 9

ASR: age-standardized rates; MENA: Middle East and North Africa.
aThere is no available prediction on State of Palestine.
The most common type of malignancy found in the oral cavity is squamous cell carcinoma. 4,11–18 Similar to other malignant neoplasms, symptoms of oral squamous cell carcinoma (OSCC) vary according to location, size, degree of invasion of neoplastic cells, and ultimately the time of diagnosis. Oral cancer cases in the MENA region present clinically as either a solitary lump or ulcer or as a red or white lesion. 12–14 Unfortunately, a high percentage of oral cancers are only discovered when they become symptomatic, at which point they may be at an advanced stage. 12–14,16 Early squamous cell carcinomas may appear as white plaques (leukoplakia), red patches (erythroplakia), or mixed red and white lesions (erythroleukoplakia). As the lesion progresses, it may become an exophytic mass with a fungating or papillary and/or ulcerated surface; while other lesions have an endophytic growth pattern characterized by a depressed, ulcerated surface with a raised rolled border. 12,14,17,18
Etiology of oral cancer
The projected increase in cancer burden in the MENA region can be attributed to population growth, population aging, better detection approaches, and most importantly to greater exposure to risk factors. 8
The etiology of OSCC is considered to be multifactorial. 17,19 In the MENA region, the main risk factors of heavy tobacco and alcohol consumption, infection by oncogenic HPV, and genetic susceptibility are likely to play a role. 11–20 Other risk factors such as environmental, occupational, and dietary may also play a role in carcinogenesis in the region and potentially may contribute to the oral and oropharyngeal carcinogenesis. 8 The most important of these factors is tobacco consumption. The role of alcohol is shadowed by social and religious barriers. No current data on alcohol consumption and oral cancer in the MENA region are available.
Tobacco habits
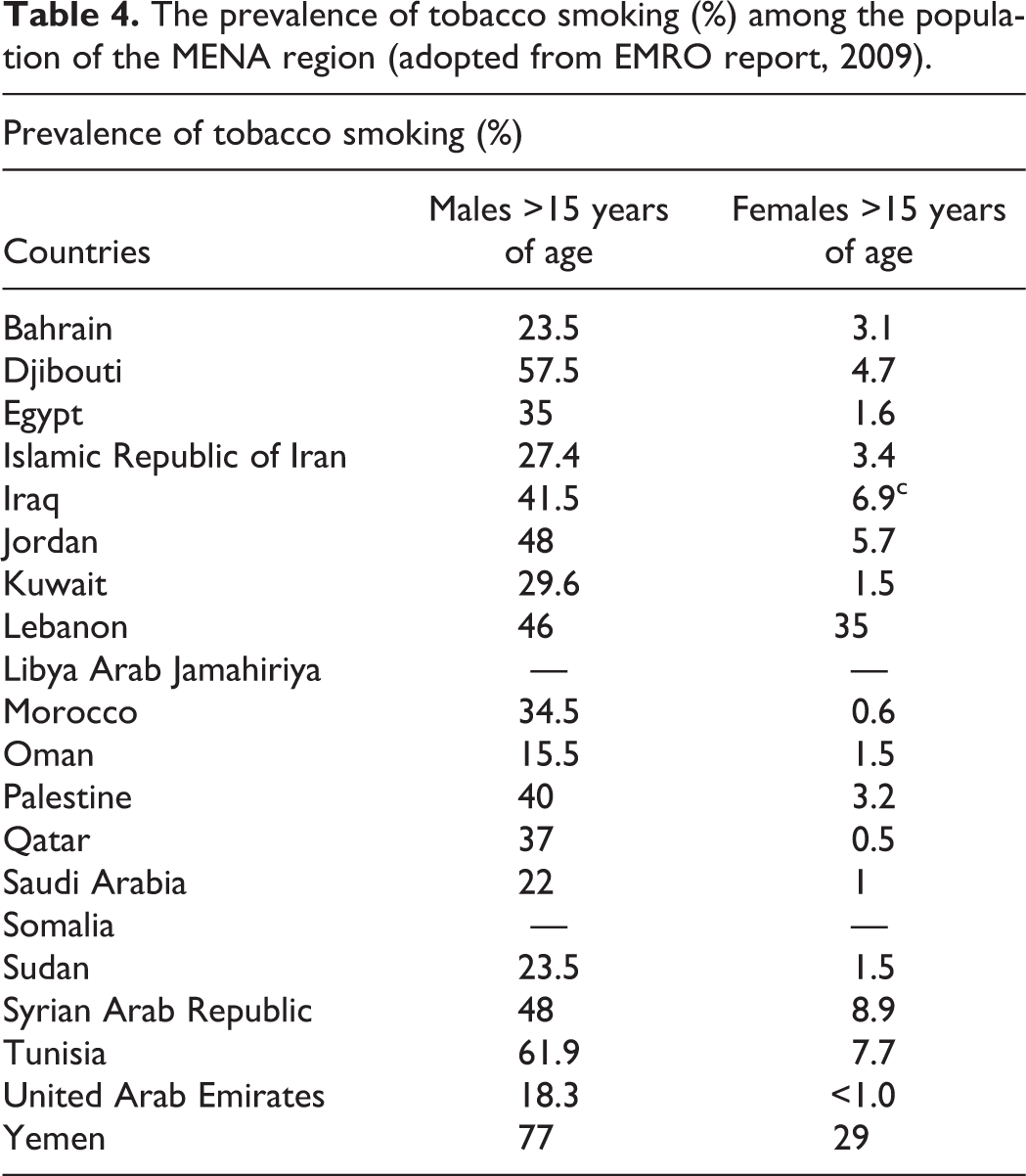
Tobacco smoking is endemic in the MENA region with high rates in male populations particularly in Tunisia (60%), Djibouti (58%), and Syria (48%). 8 Table 4 illustrates the prevalence of tobacco smoking (%) among populations of MENA. In addition to smoking tobacco, the use of smokeless tobacco, whether in the form of snuff or chewing tobacco, has been strongly linked to oral cancer. In the countries of Sudan, South West region (Jazan) of Saudi Arabia, and Yemen, smokeless tobacco and snuff (toombak and shammah) are widely used. 11,21–24 Interestingly, the high rates of oral cancer in Sudanese users were attributed to the use of these habits. 22 Idris et al. found that toombak is the most prevalent type of tobacco use in a specific region of Sudan (Nile State). 25 Specifically, the long-term use of toombak dipping has elevated the adjusted odds ratio (OR) of having oral cancer to 11.0 compared to the control group in Sudanese patients. 26 Similarly, the shammah use in Jazan province, Saudi Arabia has increased the risk of developing oral cancer by 29 times (OR = 29.3; 10.3–83.1) compared to 10 times (OR = 10.5; 2.88–3.11) for cigarette smoking. 23 These forms of smokeless tobacco are very high in tobacco-specific nitrosamines. 22
The prevalence of tobacco smoking (%) among the population of the MENA region (adopted from EMRO report, 2009).
Narghile smoking
Some synonyms have been used to describe narghile, another type of tobacco smoking, including water pipe, hookah, shisha, hubble-bubble, argileh, sheesha, narghile, nargileh, mada’a, and goza. 27 This habit consists of flavored tobacco that is burnt on charcoal and inhaled through a water-filled glass container. An interesting case–control study from Jordan found that narghile smokers were significantly younger when diagnosed with oral cancer compared with nonsmokers and that narghile smoking is an independent risk factor associated with the development of oral cancer at a younger age. 27
Alcohol
Data on alcohol drinking in the vast majority of MENA countries are missing as alcohol drinking is prohibited and considered as a taboo subject. Moreover, there are no epidemiologic studies conducted specifically to assess alcohol consumption with the risk development of OCC-OPC in MENA region. There is therefore a need for case–control studies to evaluate the role of alcohol in the development of OCC-OPC in this region.
Qat
Qat, also spelt khat or chat, is the common name for Catha edulis, an evergreen plant indigenous to Yemen and East Africa, where its fresh leaves and twigs are habitually chewed for their amphetamine-like effects. 28 This habit is also claimed to be associated with oral cancer; however, the epidemiologic evidence for this remains weak and is based on a case series which did not adequately account for concomitant tobacco use, and a descriptive retrospective study that did not include a control group. 28–30 Moreover, in a case–control study by Nasher et al. in a Yemeni cohort of 60 patients with previously untreated SCC of the oral cavity proper, and 120 gender- and age-matched controls, qat chewing did not show any association with oral cancer. 28 On the contrary, concurrent qat chewing and shammah use were associated with much lower odds of having OSCC than was shammah use alone, suggesting that qat has some protective effects against shammah-induced carcinogenesis, even if only by dilution of the main culprit. 28
Maté drinking
Dried leaves and stemlets of the perennial tree Ilex paraguariensis are brewed and consumed as a beverage in many countries in South America. 31 Drinking of maté is also very common in Syria, Lebanon, and northern Israel. A meta-analysis on data from Latin America suggests that oral cancer risk increased with the number of matécups consumed per month 31 ; however, a recent report by the Working Group of IARC outlined that this trend was statistically significant only for “hot” or “very hot” maté drinking. 32 No specific studies of such an association have been carried out in MENA countries.
Human papillomavirus
The link between HPV and oropharyngeal SCC is well established globally; however, studies from Sudan, Yemen, and Iran have found a very weak association between HPV and oral cavity cancer. 28,33,34 Oropharyngeal SCC is generally regarded as a sexually transmitted infection, arising from oral/genital contact, and cultural sensitivities make accurate data on sexual practices difficult to obtain from these populations. Further research on the role of HPV in OPC in the MENA region is needed.
Limitations of the study
Most current data on oral cancer incidence and mortality are derived from the database of the IARC (GLOBCAN 2012) and WHO reports. The published data are both scarce and often of weak quality as shown in Table 5 and mainly based on estimations from surrounding countries. The reliability of rate estimates is subject to several factors, including the accurate reporting of race/ethnicity, small numbers when classifying cases by multiple characteristics, and the accuracy of population estimates. Table 5 illustrates the quality of cancer registry data in countries of the MENA region. In fact, the highest quality cancer registry data are reported in Bahrain, Israel, Kuwait, Oman, and Qatar, while the poorest data quality are reported in Djibouti, Mauritania, Somalia, and Syria. Unfortunately, little attention has been paid to research on the epidemiology and etiology of oral cancer in the MENA region.
Quality of cancer registry data in countries of MENA region (Adopted from GLOBOCALN 2012). 9

MENA: Middle East and North Africa; WHO: World Health Organization.
aAvailability of incidence data: A, high-quality national data or high-quality regional (coverage greater than 50%); B, high-quality regional (coverage between 10% and 50%); C, high-quality regional (coverage lower than 10%); D, national data (rates); E, regional data (rates); F, frequency data; and G, no data. Availability of mortality data: 1, high-quality complete vital registration; 2, medium-quality complete vital registration; 3, low-quality complete vital registration; 4, incomplete or sample vital registration; 5, other sources (cancer registries, verbal autopsy surveys, etc.); and 6, no data. National statistics are collated and made available by the WHO for countries with vital registration.
There have been several attempts to implement cancer prevention measures in this region. The WHO East Mediterranean Regional Office has published a strategy report on cancer prevention and control in the region over the period 2009–2013. The Ministry of Health in Saudi Arabia has launched a Tobacco Control Program that includes several campaigns to increase the awareness of the harmful effects of tobacco smoking, shammah, and toombak use 35 ; nonetheless, there are no studies on the effectiveness of these efforts in reducing these habits. Remarkably, the Ministers of Health of Egypt, Israel, Jordan, Cyprus, and the Palestinian Authority signed an agreement to establish the Middle East Cancer Consortium (MECC) in 1996, 35 after which Turkey joined the Consortium in 2004. A comprehensive publication of the MECC Cancer Registration Project was released in 2006. 36 The monograph presents information about cancer incidence for populations in Cyprus, Egypt (Gharbiah Region), Israel (Jews and Arabs), and Jordan for the period 1996–2001, but no further reports have been published.
Conclusions
Given that the MENA region is currently in turmoil, particularly in those countries with running conflicts (Syria, Iraq, Libya, and Yemen), little attention has been paid to tackle cancer as a health system concern. Cancer registries in the region are almost overlooked, with resources in the region directed exclusively to treatment.
Gaps in our knowledge of the etiology and epidemiology of oral cancer in the region exist in terms of reporting and registering newly diagnosed cases, differences in incidence and mortality within countries, the association with socioeconomic status, in addition to the inter- and intracountry variations in the distribution and patterns of risk factors. The accuracy and completeness of death registration is also a significant concern—as in much of the world.
There is a need to improve the infrastructure of cancer registries in countries of the MENA region in addition to reporting strategies, to extract high-quality data. Initiatives led by local governments and international agencies (WHO and World Bank) are required to implement preventive measures, such as improving public awareness of the harmful role of high-risk habits such as tobacco in increasing the risk of oral cancer. It is also crucial to ensure provision of high-standard clinical services for patients with oral cancer in this region. Attention should be paid to funding opportunities that aim to train clinicians and scientists to undertake research to fill the gaps in our current knowledge of oral cancer and oral potentially malignant disorders in this region.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.