
Abstract
The UK Royal College of Pathologists has published widely recognized guidelines that are finding increasing acceptance in the histological assessment of surgical margins of oral squamous cell carcinoma (OSCC). These guidelines are based on the distance of surgical margins from tumour tissue. The results of various published articles indicate that overall shrinkage of OSCC specimens varies from 15% to 75% and depends upon many irrepressible intrinsic and extrinsic factors. In the present article, the intrinsic and extrinsic factors accountable for shrinkage are discussed in depth. A novel basal cell counting method for the assessment of margins and the calculation of shrinkage in OSCC specimens with flat epithelial connective tissue interfaces have also been put forward.
Introduction
Oral squamous cell carcinoma (OSCC), which is usually preceded by a premalignant disorder, is the most common malignant neoplasm of the oral cavity. 1 –3 The most common treatment modality for OSCC is surgical excision followed by radiotherapy. 4,5 Histopathological assessment of the surgical margins of malignant diseases plays a crucial role in pathological practice, including the treatment of OSCC. Positive surgical margins are more frequently associated with OSCC than any other malignancy of the head and neck region. 6,7
Criteria for interpretation of surgical margins of OSCC have been widely discussed in the literature. The UK Royal College of Pathologists issued widely recognized standards that are finding increasing acceptance in the histological assessment of surgical margins. As per these guidelines, clear margins are defined as a distance of 5 mm or more from the invasive tumour cells. Likewise, a distance of 1–5 mm is considered to denote close margins, and <1 mm is considered to denote involved margins. 8
An important cause of OSCC treatment failure is local recurrence. 9 –11 A high rate of local recurrence is concurrent with histologically close or positive margins. 9,10,12,13 The clinical significance of obtaining histologically normal tissue around a resected tumour has been well described and discussed. 9,10,12,13 To attain an adequate margin in the oral cavity is often challenging. Frequently, the histologic margins are reported to be significantly short of those measured clinically (in situ margins), which may account for the high rate of close or positive margins reported in the recent literature. 14,15 This can be explained in two ways. The first is that microscopically, tumour cells may spread beyond the clinically detectable tumour. In routine surgical practice, a 1-cm margin of clinically normal tissue is removed along with the resected tumour to account for this. The goal is to create surgical margins with a minimum of 5 mm of histologically normal tissue. However, tumour extensions may sometimes invade out of the main tumour mass, leading to closer margins than anticipated. Last but not least, tissue retraction/shrinkage after resection and/or pathologic processing of the specimen may cause surgical margins to move closer to the tumour tissue. 16,17 In the literature, this phenomenon has been described in oesophageal cancer (50%), 18 cutaneous (20.66%), 19 melanoma (15–25%), 20 basal cell carcinoma (14%), 21 breast cancer (34%), 22 colorectal cancer (>50%), 23,24 uterine cervical tissue (15.3%) 25 and optic nerve tissue (30.3%). 26 With the aforementioned aspects in mind, we reviewed the studies published on shrinkage and discussed the possible effects of shrinkage on the interpretation of surgical margins in OSCC.
Search strategy and selection criteria
Research papers were identified through an electronic search of PubMed using the terms ‘oral squamous cell carcinoma’, ‘surgical margins’, ‘surgical margin shrinkage’ and ‘mucosal margin shrinkage’. Only papers published in English between 1978 and 2016 have been included for discussion.
OSCC and shrinkage
Oral cancer is unique in many aspects, 27 –30 but we believe shrinkage of OSCC surgical margins warrants special attention. It has been proposed that numerous factors may influence the shrinkage of tissue specimens. A majority of the shrinkage is attributed to post-resection or prefixation shrinkage, as opposed to shrinkage related to fixation and processing. 31 The literature suggests that the total shrinkage of OSCC depends on the site, 16,17,31 the stage, 16,17,32 the patient’s age, 33 the fixation technique, 16,17,31 and the method of resection. 33 Tissue composition is the determining factor in site-related variation in shrinkage percentage. Tongue tissue is mainly covered with keratinized stratified squamous epithelium and contains many muscle fibres, which are contractile in nature. Hence, OSCC of the tongue shrinks more than any other tissue in the oral cavity. 17 Further complicating this scenario, in two separate studies, site-specific shrinkage was reported with great variation (Table 1). For example, total shrinkage of buccal mucosa is 48.8% in one study 16 versus 71.9% in a second study 31 ; tongue, 32.4% 16 versus 42% 31 ; and post-resection shrinkage of buccal mucosa, 38.3% 31 versus 21.2%. 17 There is no proven mechanism underlying such variation, but it could be attributable to tumour-associated factors such as tumour cell cohesiveness, degree of keratinization, desmoplasia associated with either tumour or oral submucous fibrosis and degree of inflammation. Age has also been reported to influence the percentage of shrinkage. An interesting study by Kerns et al. 32 suggests that shrinkage decreases by 0.3% per year of the age of the patient. Various surgical techniques are also known to affect the shrinkage of tissue. Smith et al. 33 observed that cutting diathermy is associated with minimal shrinkage when compared with the use of Harmonic scalpels, conventional scalpels or coagulative diathermy. In fact, the use of conventional scalpels results in the maximum shrinkage of tissue specimens. The aforementioned points about the role of various intrinsic and extrinsic factors affecting tissue shrinkage are unpredictable, uncontrollable and inconsistent.
Literature review of shrinkage associated with oral specimen.
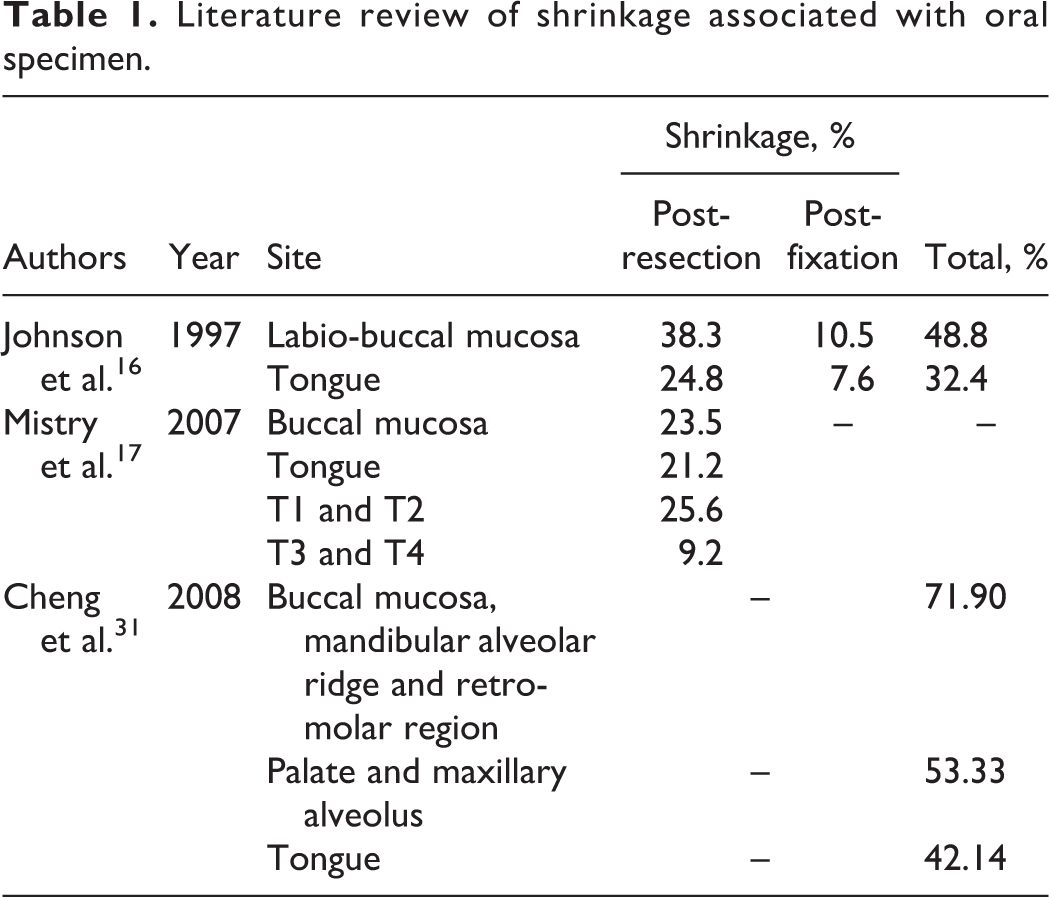
Tumour size is also reported to be a factor in the shrinkage of excised OSCC tissue. Mistry et al. 17 found shrinkage of 25.6% in T1–T2 stage OSCC versus 9.2% in T3–T4 stage. This finding has been attributed to the destruction of contractile cells and elements in the connective tissue stroma, all of which are replaced with non-contractile tumour cells that cause less shrinkage. 16 However, this may not be true, as Cheng et al. reported contradictory results showing more shrinkage in T3–T4 stage (75%) compared with T1–T2 stage (51.48%). 31
Shrinkage in a single specimen could vary by location. Intra-tumoral tissue may show less shrinkage due to the destruction of contractile elements and their replacement with non-contractile tumour cells. However, in a histopathological assessment, what really matters are the margins of the specimen and their interpretation. In this location, tumour tissue is usually absent or minimal, which can lead to significantly more shrinkage than that observed in the intra-tumoral region. Moreover, the composition of tissue margins may also contribute to the variation in shrinkage. Recently, mucocele has been reported in the surgical margins of excised OSCC tissue as an accidental finding. 34,35 This difference in shrinkage was reported by Blasdale et al. 21 in basal cell carcinoma of the skin (intra-tumoral: 11% and tumour free margin: 19%). Thus, the stage of OSCC does not influence shrinkage.
Shrinkage and misinterpretation of surgical margins
Studies in the literature have reported an increase of nearly 2½ times the hazard ratio (or risk) of recurrence in OSCC. 36 In a recent study, compared to patients with clear margins, the relative risk of local recurrence in patients with an involved margin was 7.89, and in those with a close margin, it was 3.79. 37 Other studies have reported 64%, 8 10.5%, 9 36%, 10 21.9% 12 and 29% 38 risk of local recurrence associated with involved and/or close margins. We feel the risk of recurrence in cases of involved margins or close margins without local recurrence needs to be explained. The reasons could be attributed to the effect of post-operative radiotherapy and/or chemotherapy or misinterpretation of involved margins due to shrinkage of the specimen. However, post-operative radiotherapy does not seem to decrease the rate of recurrence, as seen in many studies, 8,9,39 and thus the reason could be attributed to the misinterpretation of surgical margins.
Definition of surgical margin interpretation
Although surgical margin interpretation has been widely investigated, a lack of uniformity exists in the literature because no consensus has been reached on the definitions of involved, close or clear surgical margin. Some authors have defined a close margin by the presence of tumour cells within 2 mm of the resection margin and have reported different prognoses for clear and close margins. 39 –41 However, others have defined a close margin as the presence of tumour cells within 3 mm of the resection margin 42,43 or within one high-power field of the resection margin. 44 Moreover, some authors have relied on variable definitions related to the pattern of invasion. 12 The most broadly accepted definition of marginal status is given by the Royal College of Pathology UK (also called UK guidelines), which states that a close margin encompasses a width of 5–1 mm and an involved margin encompasses less than 1 mm. 7 Due to the lack of consensus on definitions, a call for reliable, standardized guidelines has been proposed in the literature. 41 We believe this lack of consensus stems from inter-laboratory and inter-institutional variability in the percentage of tissue shrinkage attributable to extrinsic factors and resulted in discrepancies in the definition of surgical margins.
The UK guidelines for the histological assessment of surgical margins do not mention any particular percentage of shrinkage, so it is impossible to modify the existing guidelines on this basis. The current guidelines need to be reassessed and new guidelines established. We believe the current guidelines should take into consideration tissue shrinkage, and shrinkage-based guidelines could be the answer to this problem. Thus, future studies are needed in this direction. The calculation of tissue shrinkage is an easy, time-efficient process that requires minimal instrumentation (ruler or vernier caliper). Hence, in routine pathology practice, it is feasible to calculate shrinkage for every surgical specimen. 15,16,31 We recommend that pathology reports mention the distance (in millimetres) of tumour cells from mucosal and deep resection margins to simplify the establishment of modified guidelines based on shrinkage. The comparison of shrinkage to margin status, which is correlated with local recurrence, prognosis and survival rate, will assist us in standardizing the guidelines.
Suggestions
To overcome the issue of shrinkage, the distance can be calculated by counting the epithelial basal cells of surgical margins (width of a basal cell is 10 µm). This method gives us an accurate measurement of the distance irrespective of the shrinkage. However, this method should only be used when the epithelial connective tissue interface is flat at the mucosal margins. This method cannot be used in the case of deep margins, epithelium with rete ridges, basal cell hyperplasia, cases involving the loss of polarity of basal cells, or in cases where basal cell counting is not possible. We have used the basal cell counting method for accurate calculation of tissue shrinkage, and it can be used in the future for shrinkage-based assessment of surgical margins. 45,46
Shrinkage-related issues can be avoided with intraoperative analysis by various methods: frozen section analysis of margins, microendoscopy, optical coherence tomography, or elastic scattering spectroscopy. 47 The major problems associated with these methodologies are cost and the complexity of the procedures. Hence, UK guidelines are applied worldwide for routine histopathological assessment of surgical margins. We believe that shrinkage-normalized assessment of surgical margins will provide more consistency in predicting loco-regional recurrence. Although it could take many years of prospective study, the ultimate outcome will benefit the generations to come.
Footnotes
Acknowledgement
A portion of the article was presented as a poster in XI Indian Association of Oral and Maxillofacial Pathologist Post-Graduate Convention at Manipal, India, on July 2011 and won a best scientific presentation award.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.