
Abstract
Objectives:
Our aim was to provide an up-to-date and review the incidence and mortality of oral and pharyngeal cancer in Europe.
Methods:
Data were retrieved from both national and regional population-based cancer registries. The online browser used in the present study was the European Network of Cancer Registries (EUREG. Version 1.0), which provided data for 22 countries of Northern and Eastern Europe and for 20 countries of Western and Southern Europe on the incidence of and mortality for oral and pharyngeal cancer. For countries not included in EUREG, data were retrieved from the European Cancer Estimates (EUCAN), the Global Cancer Estimates (GLOBOCAN) and Cancer Incidence in Five Continents. Oral cancer sub-sites were classified according to International Classification of Diseases and Related Health Problems, 10th Edition categories.
Results:
Hungary recorded highest rates among European countries for both morbidity and mortality. Historically, France has had high rates particularly in areas in the north of France, where oral cancer was the most common in men. A decline in the incidence has been noted in the past one and half decades. However, France still has the highest incidence rates of orophayngeal cancer, one of the highest in the world. Denmark records high rates of oral cancer in women and lip cancer incidence is high in Spain.
Conclusions:
In Europe, regional differences in oral and pharyngeal cancer in terms of incidence and mortality are evident not only between north and south and between east and west but also within single regions (e.g. between the Scandinavian countries and the former Soviet republics). These findings reflect differences in lifestyle and in exposure to risk factors such as smoking (e.g. high incidence in Danish women), alcohol (e.g. in Lithuanian men) or both (e.g. Belgium and Portugal). Other traditional factors, such as actinic radiation, are responsible for a considerable number of cases of lip cancer (e.g. Spain), and oncogenic potential of human papillomavirus explains the rising trend in oropharyngeal cancer in some countries (e.g. Denmark and Scotland).
Introduction
Oral (International Classification of Diseases and Related Health Problems [ICD] 01-10) and pharyngeal cancer (ICD 11-14) is the 8th most common cancer and the 11th leading cause of cancer-related mortality in Europe. 1 The estimated annual new cases of oral and pharyngeal cancer in this continent are close to 100,000. 2 In 2012, the estimated global age-standardized incidence of oral cavity cancer (per 100,000 person-years) was 5.5 in males and 2.5 in females, while in Europe the rates were higher at 7.5 and 2.5, respectively. 3 When oral and pharyngeal cancers were considered together, the annual incidence rose to 18.2 in males and 4.9 in females. 3
There are differences in cancer burden across Europe, between Western European and Eastern European countries. This can be explained in part by differences in cancer risk factors, including smoking, alcohol and dietary habits 4 as well as human papillomavirus (HPV) distribution (HPV Information Centre; available at http://www.hpvcentre.net). Differences are more pronounced in terms of cancer mortality. 5 In 2012, the estimated age-standardized cancer mortality among men was 5.1 in Central and Eastern Europe and 1.6 in Northern Europe. 3 Many of these differences have their roots in socio-economic inequalities derived from diverse political systems, 5 as limited treatment facilities and comorbidities can increase mortality rates. 6
The aim of our study was to provide an up-to-date review of the incidence and mortality of oral and pharyngeal cancer in Europe and to analyse the differences between the European geopolitical regions as defined by the United Nations (United Nations Population Division, 2010). 7
Methods
Data were retrieved from population-based registries, including both national cancer registries and regional cancer registries (RCRs). The availability of population-based cancer registries was determined through the list of cancer registries provided by the International Association of Cancer Registries (http://www.iacr.com.fr) and by the European Network of Cancer Registries (http://www.encr.eu). Data from different RCRs in a single country were gathered and results were considered indicative of the whole national territory (e.g. Italy has 38 RCRs; the pooled data from all these registries were referred to as ‘Italy’).
The online browser used in the present study was the EUREG (available at http://eco.iarc.fr/ EUREG/AnalysisT.aspx), provided by the European Cancer Observatory (ECO), hosted by the International Agency for Research on Cancer (IARC) of the World Health Organization (WHO). EUREG allows geographical patterns and temporal trends in incidence, mortality and survival to be analysed in European population-based cancer registries for 35 major cancer entities in about 100 registration areas.
Adhering to the European regions defined by the United Nations, 7 we obtained data on the incidence and mortality for oral and oropharyngeal cancer in Northern and Eastern Europe from population-based cancer registries in 22 countries (Northern Europe: Denmark, Estonia, Finland, Iceland, Ireland, Latvia, Lithuania, Norway, Sweden and United Kingdom; Eastern Europe: Belarus, Bulgaria, Czech Republic, Hungary, Kazakhstan, Moldova, Poland, Romania, Russia, Siberia, Slovakia, and Ukraine). Analyses of oral and oropharyngeal cancer in Western and Southern Europe included data from 20 countries (Western Europe: Austria, Belgium, France, Germany, Luxembourg, the Netherlands and Switzerland; Southern Europe: Albania, Bosnia-Herzegovina, Croatia, Cyprus, Greece, Italy, Macedonia, Malta, Montenegro, Portugal, Serbia, Slovenia and Spain).
Oral cancer sub-sites were classified according to ICD-10 categories (WHO, 2008). 8 However, in order to standardize data, sub-sites C01 and C02 could not be separated and were included in the group ‘oral cavity’, which encompassed sub-sites C01–06.
For countries without a population-based cancer registry included in the EUREG, data were retrieved from the most recent literature as well as from sources derived by the WHO-IARC that provided an estimate of incidence and mortality rates for 2012, such as EUCAN, GLOBOCAN and Cancer Incidence in Five Continents (CI5). 2 The most recent year of registration available within EUREG, EUCAN (European Cancer Observatory), GLOBOCAN and CI5 was selected for both incidence and mortality. Data on incidence and mortality were further grouped by sex and were reported as ‘number of cases’ and ‘age-standardized rate’. Rates are given per 100,000 person-years.
Results
Northern Europe
Incidence
The incidence data extracted from cancer registries of Northern Europe are presented in Table 1. Based on the 2012 EUCAN national estimates and considering together the C00–014 sub-sites, the Northern European countries with the highest incidences were Denmark (13.0), Lithuania (9.9) and the United Kingdom (9.8).
Latest incidence rates in Northern Europe.a
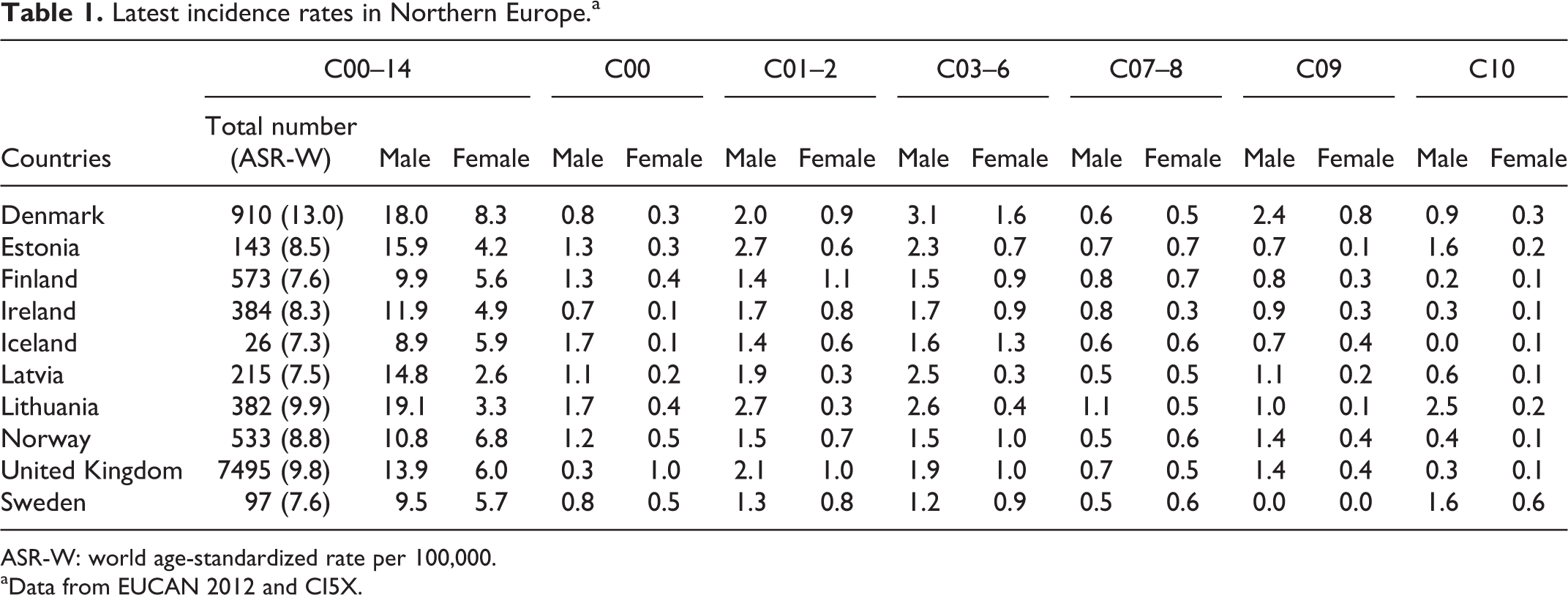
ASR-W: world age-standardized rate per 100,000.
aData from EUCAN 2012 and CI5X.
On analysis by gender, the highest incidences of oral cancer in men were observed in Lithuania (19.1), Denmark (18.0) and Estonia (15.9). Among women, the highest incidences were reported in Denmark (8.3), Norway (6.8) and the United Kingdom (6.0).
There was some controversy in the data provided for Estonia as, in 2012, the estimated incidence according to ECO: EUCAN was 15.9 in men, 4.2 in women and 8.5 in total, whereas the estimations of the Estonia Cancer Registry were 21.3, 5.4 and 12.8, respectively.
The 5-year cumulative prevalence was very similar in all the Northern European countries, ranging from 46.0 in Lithuania and Latvia to 51.7 in Finland.
The trends in incidence rates in the period 2009–2013 showed a significant and worrying annual percentage increase (API) among men in Denmark, Finland and Sweden (API 2.7%, 2.1% and 2.0% per year, respectively), and among women in Sweden and Denmark (3.0% and 2.5% per year, respectively).
Incidence by ICD-10 subsites
The highest incidence of C01–02 cancers in men was detected in Estonia (42.7) and Lithuania (2.7). The highest rates of C03–06 neoplasms in men were observed in Denmark (3.1), Lithuania (2.6) and Latvia (2.5); in women, these rates were highest in Denmark (1.6) and Iceland (1.3). Estonia showed a high incidence of C9–10 cancers (5.0). In contrast, no C09 tumours were detected in Swedish men or women. The incidence of C12–13 cancers in Estonian men was 4.7.
Regional differences have been detected in some countries. In the United Kingdom, for example, the National Cancer Registration Service (Oxford) reported an age-standardized incidence of C03–06 tumours in men of 1.9 for the period 2003–2007 compared with a rate of 3.4 in Scotland for the period 2004–2007.
A sub-site analysis of incidence data for all countries in the region is included in Table 1.
Mortality
The latest reported mortality data (2012) extracted from EUCAN for Northern Europe are presented in Table 2.
Latest mortality rates in Northern Europe.a
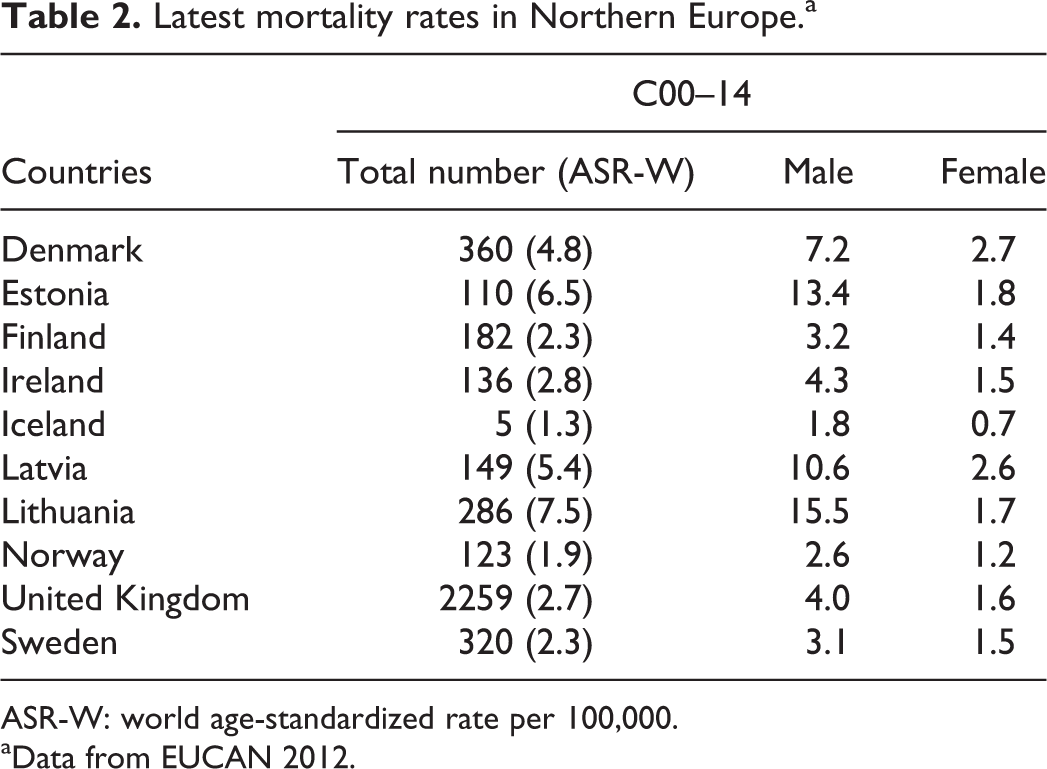
ASR-W: world age-standardized rate per 100,000.
aData from EUCAN 2012.
Oral cancer was not included in the top 10 world causes of death ranked by country (World Life Expectancy; available at http://www.worldlifexpectancy.com) in any of the Northern European countries.
In terms of mortality, the highest rates for the year 2012 were reported in Lithuania (7.5), Estonia (6.0) and Latvia (5.4); European Cancer Observatory, available at http://eco.iarc.fr).
In men the highest rates were observed in those same countries, Lithuania (15.5), Estonia (13.4) and Latvia (10.6), while the highest rates in women were observed in Denmark (2.7), Latvia (2.6) and Estonia (1.8).
In Ireland, as in most Northern European countries, there has been a progressive decrease in oral cancer mortality: This is inferred from the age-standardized, net 5-year survival of 41.9% in the period 2000–2005 and of 48.2% in 2008–2012. In Estonia, the age-adjusted mortality in women fell by 32.2% on comparing the period 2000–2001 with 2005–2007. Paradoxically, annual mortality among women in Iceland has increased by 10.5% per year over the past 10 years.
Eastern Europe
Incidence
The incidence data extracted from cancer registries of Eastern Europe are presented in Table 3.
Latest incidence rates in Eastern Europe.a

ASR-W: world age-standardized rate per 100,000.
aData from EUCAN 2012 and CI5X.
Based on EUCAN national estimates and considering together the C00–14 sub-sites, the highest incidences of oral cancer, in the Eastern European countries in 2012, were detected in Hungary (23.3), Slovakia (16.4) and Romania (15.5).
On analysis of the data by gender, the highest incidences in men were observed in the same countries: Hungary (39.8), Slovakia (30.3) and Romania (29.6). In women, the highest incidences were reported in Hungary (9.5), the Czech Republic (6.1) and Slovakia (4.8).
The 5-year cumulative prevalence was very similar across all the Eastern European countries, ranging from 46.8 in Slovakia to 49.7 in the Czech Republic.
Incidence by ICD-10 sub-sites
Oral cancer incidence rates in Slovakia in the period 2003–2007 were highest in men for the C01–02, C03–06 and C09 neoplasms.
Regional differences were detected in some countries. In Poland, the highest incidence in the Kielce Registry corresponded to C00 neoplasms, whereas the C03–06 neoplasms were more common in the Lower Silesia and Podkarpackie registries.
In terms of temporal trends in incidence, the Czech National Cancer Registry showed a progressive increase in C00–08 cancers from 2003 to 2013, and an increase in C09, C10 and C12–14 in the period 1996–2013. The Rzeszow Cancer Registry in Poland has information available from 1992 to 2012; during this period no significant variations were observed in C00–09 incidence, but an increase has been observed in C00–14 malignancies in men in recent years.
A sub-site analysis of incidence data for all countries in the region is included in Table 3.
Mortality
The latest reported mortality data (2012) extracted from EUCAN for Eastern Europe are presented in Table 4.
Latest mortality rates in Eastern Europe.a

ASR-W: world age-standardized rate per 100,000.
aData from EUCAN 2012.
In terms of mortality (ECO), the highest rates in 2012 were detected in Hungary (12.5), Slovakia (10.2) and Romania (9.1). In men, the highest rates corresponded to Hungary (23.1), Slovakia (19.8) and Romania (17.9), while in women the highest rates were observed in Hungary (3.7), Bulgaria (3.7) and Slovakia (2.3).
Oral cancer is among the top 10 causes of death in Hungary (World Life Expectancy); Hungary also ranked third in the world for mortality from oral cancer per 100,000 population. In 2014, Hungary also ranked first in the world for mortality from lung cancer and colorectal cancers and second in the world for pancreatic cancers. Slovakia ranked seventh in the world for mortality from oral cancer.
In recent years there has been a significant increase in oral-cancer-related mortality in women in most Eastern European countries. In Belarus, a 61% increase was noted when comparing the rate in 2007 with that in 2000–2003. In Romania the increase was of 31%, comparing the period 1990–1994 with 2000–2004, and in the Czech Republic it was of 37%, comparing the period 2000–2004 with 2005–2007. In Moldova the age-adjusted rate increased by 31% between the periods 1990–1994 and 2000–2004 and by 8% between 2000–2004 and 2005–2007 (22% considering the overall period). In Slovakia, the increase was of 59% on comparing 1990–1994 with 2000–2004, and in Hungary it was of 68% between 1990–1994 and 2000–2004, but there was a decrease of 10% in mortality between the period 2000–2004 and 2005. In Bulgaria, a 31% increase was detected when comparing the 1990–1994 rate with the figure for 2000–2003, and this rose to 76% when comparing the period 2000–2003 with 2005–2006.
The increase in oral-cancer-related mortality among men was most notable in Romania (65% between the periods 1990–2000 and 1994–2004), in Hungary (32% increase between the periods 1990–1994 and 2000–2004, though with a 10% decrease when comparing 2000–2004 with 2005) and in Bulgaria (30% increase when comparing the period 2000–2003 with 2005–2006).
Western Europe
Incidence
The incidence data extracted from cancer registries of Western Europe are presented in Table 5.
Latest incidence rates in Western Europe.a
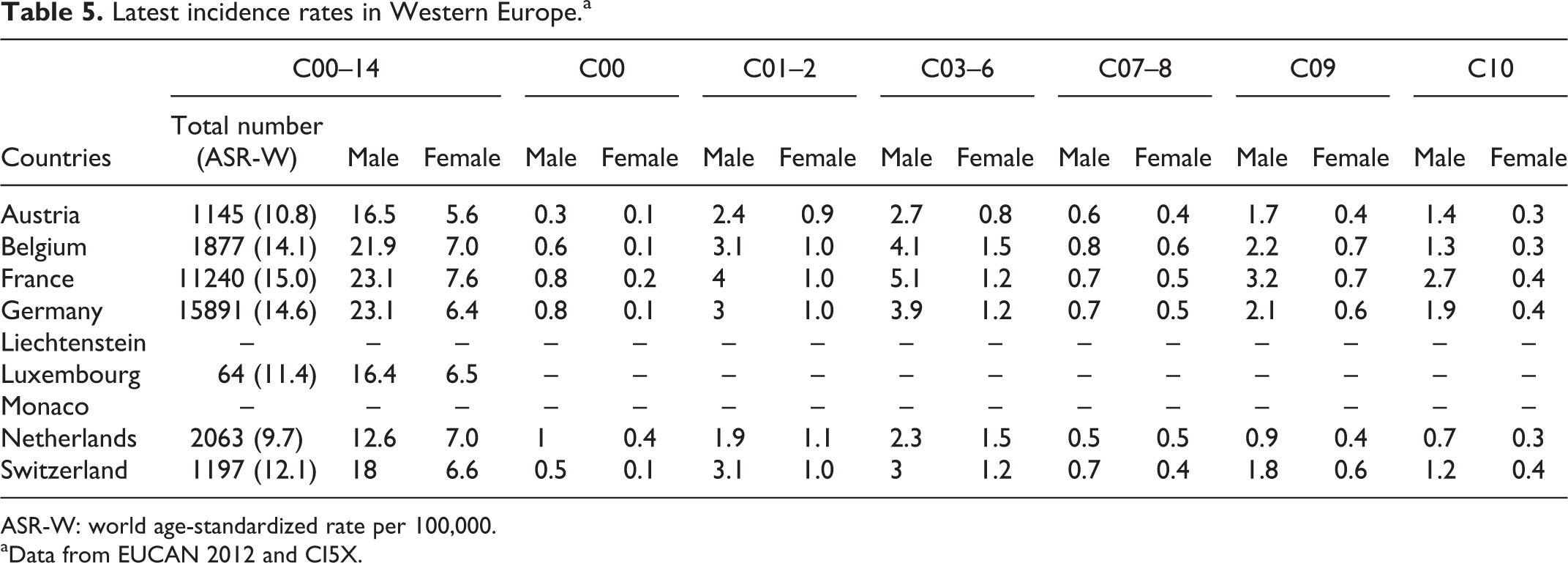
ASR-W: world age-standardized rate per 100,000.
aData from EUCAN 2012 and CI5X.
Based on EUCAN national estimates and considering together the C00–14 sub-sites, the highest incidences in Western European countries in 2012 were detected in France (15.0), Germany (14.6) and Belgium (14.1).
When data were analysed by gender, the highest oral cancer incidences in men was observed in Belgium (21.9), followed by France (23.1) and Germany (23.1). Among women, the highest incidences were reported in France (7.6), Belgium (7.0) and the Netherlands (7.0).
Certain discrepancies have been noted among various databases in the present research. For example, data from the Regional Cancer Registries of France (available at: http://www.e-cancer.fr) showed a lower incidence of cancer in the C00–14 sub-sites than was reported on EUCAN (the estimated incidence in the French Regional Cancer Registries for 2012 was 10.8 in the overall population: 16.1 in men and 5.6 in women). Similarly, data from the Belgian Cancer Registry in 2013 (available at www.kankerregister.org) showed a significantly lower incidence of oral and oropharyngeal cancer than that reported on EUCAN (incidence in the Belgian Cancer Registry was 9.55 for the overall population: 14.4 in men and 4.7 in women).
Some countries, such as Austria, the Netherlands and Switzerland, have national cancer registries or RCRs with accurate data on incidence covering more than 15 years. In those nations, a slow but persistent increase in the number of cases of oral and pharyngeal cancer was observed between 1991 and 2007.
Incidence by ICD-10 sub-sites
Taking into account the most recent available data on national cancer registries, sub-classified according to the ICD-10 (Table 5) the highest incidence of cancer of the lip (C00) was recorded in the Netherlands (1.0 in men and 0.4 in women), followed by France (0.8 in men and 0.2 in women) and Belgium (0.6 in men and 0.1 in women). The highest incidences of cancer in the oral cavity (C02–06) were recorded in France (overall population, 5.6; men, 8.8; and women, 2.5 [EUREG, 2009]), Switzerland (overall population, 4.5; men, 6.3; and women, 2.8 [EUREG, 2009]) and Germany (overall population, 3.6; men, 4.7; and women, 1.9 [German Regional Cancer Registries, 2012]).
With regard to the pharynx (C01, C09, C10, C12, C13, C14), the highest incidences were again detected in France (overall population, 6.5; men, 11.2; and women, 2.2 [EUREG, 2009]), Belgium (overall population, 4.8; men, 7.8; and women, 1.9 [Belgian Cancer Registry, 2013]) and Germany (overall population, 3.9; men, 6.4; and women 1.6 [German Regional Cancer Registries, 2012]).
Mortality
According to the 2012 GLOBOCAN projections for Western Europe, mortality due to oral and pharyngeal cancer (C00–14) was highest in France, Belgium and Germany, with rates of 4.7, 4.2 and 4.2, respectively (Table 6). These findings are supported by the most recent data available in national cancer registries and RCRs. Looking specifically at cancer of the oral cavity (C02–06), mortality in Austria was 1.3 for the overall population, 1.9 in men and 1.7 in women (EUREG, 2009), in Belgium was 1.3 for the overall population, 2.2 in men and 0.6 in women (EUREG, 2006), and in Germany was 1.3 for the overall population, 1.5 in men and 0.4 in women (German Regional Cancer Registries, 2012).
Latest mortality rates in Western Europe.a

ASR-W: world age-standardized rate per 100,000.
aData from EUCAN 2012.
Among the Western European countries with national cancer registries or RCRs covering at least 15 years of follow-up (including Austria, the Netherlands and Germany) and considering all sub-sites (C00–14), a slight decrease in mortality was only detected in Germany (a fall from 5.1 in 1990 to 4.3 in 2007).
Southern Europe
Incidence
The incidence data extracted from cancer registries of Southern Europe are presented in Table 7.
Latest incidence rates in Southern Europe.a
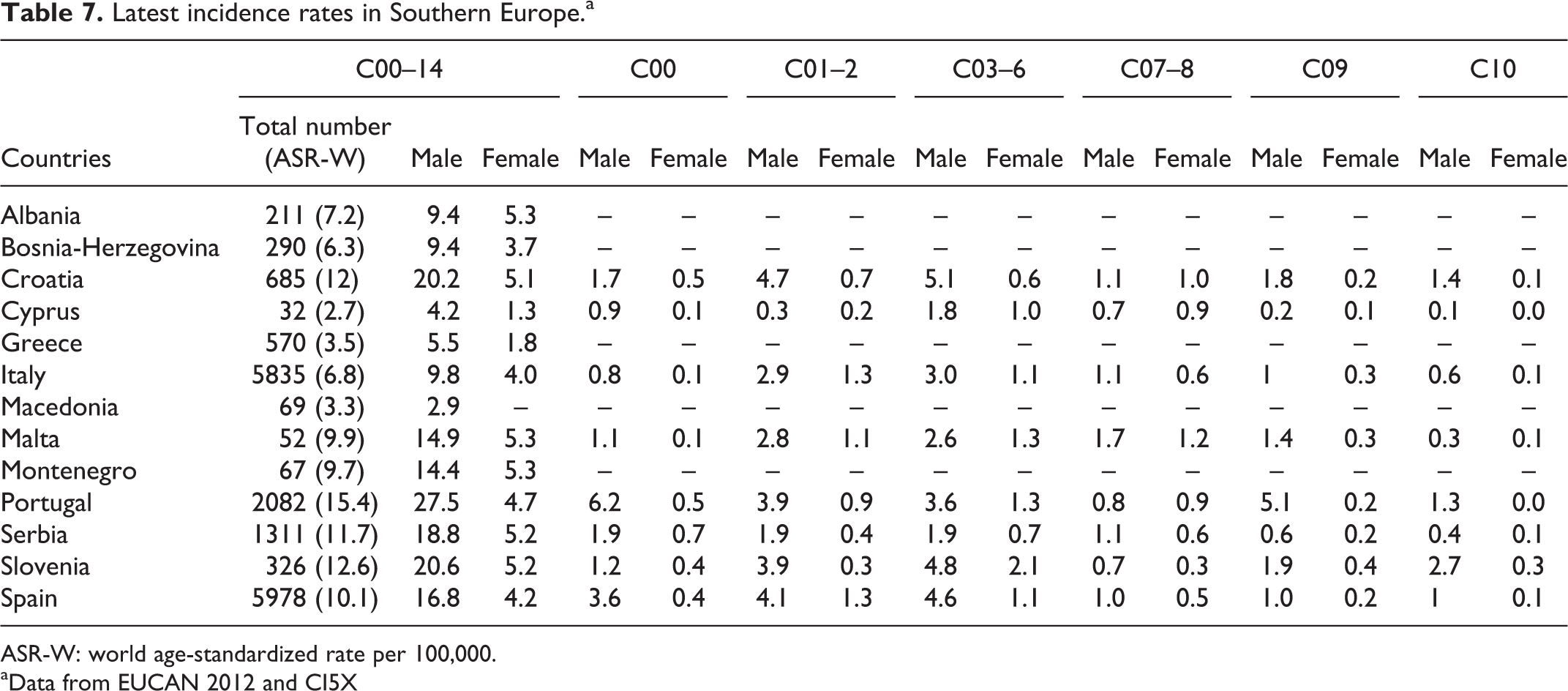
ASR-W: world age-standardized rate per 100,000.
aData from EUCAN 2012 and CI5X
According to the projections of GLOBOCAN 2012, the countries in Southern Europe with the highest incidence of oral and pharyngeal cancer considering all sub-sites (C00–14) were Portugal (15.4), Croatia (12) and Serbia (11.7). The same countries also presented the highest incidences among men: Portugal, 27.5; Croatia, 20.2; and Serbia, 18.8. However, the incidence among women was slightly higher in Montenegro (5.3), Malta (5.3) and Serbia (5.2). According to the same data source (GLOBOCAN, 2012), the countries in Southern Europe with the lowest incidence of oral cancer in 2012 were Cyprus (2.7), Macedonia (3.3) and Greece (3.5).
National cancer registries and RCRs with accurate data on incidence rates covering more than 15 years are available for Italy, Spain and Slovenia. Considering all ICD-10 sub-sites (C00–14), a decrease in the incidence of oral and pharyngeal cancer was observed in most areas of Italy and Spain, dropping from around 11.5 in both countries in 1991 to between 8 and 9.5 in 2007. In the same period, the incidence in Slovenia remained almost unchanged, between 6 and 7.
Incidence by ICD-10 sub-sites
For Southern Europe, homogeneous data on incidence sub-classified according to ICD-10 have been drawn from the EUREG database. We present the most recent data available for each nation using the tools of the European Cancer Observatory.
Lip cancer (C00) appears to be most frequent in Spain (2.3), followed by Serbia (1.6) and Croatia (1.5). The incidence of lip cancer in men is also highest in Spain (4.6), followed by San Marino (3.1), Croatia (2.6) and Serbia (2.4).
Considering both sexes, cancer of the tongue (C01–02) has its highest incidence in Spain (2.6) and Croatia (2.6), followed by Portugal (2.4) and Italy (2.1). When considering only men, tongue cancer showed the highest incidence in Croatia (4.7). Countries with higher incidence rates of cancer at this site in women are Italy (1.3) and Spain (1.3).
The highest incidence rates of cancer in the C03–06 sub-sites were observed in Slovenia (3.4), followed by Spain (2.8) and Croatia (2.7). The highest rates in men were observed in the same countries: Croatia (5.1), Slovenia (4.8) and Spain (4.6).
Similarly, cancer of the pharynx (C09–14) in the Southern European countries was also more common in Slovenia (6.5), Spain (5.6) and Croatia (5.2). A sub-site analysis of incidence data for all countries in the region is included in Table 7.
Mortality
According to the most recent data retrievable from EUREG, mortality from cancer in the C01–06 sub-sites is highest in Croatia (1.8), followed by Portugal (1.4) and Spain (1.4) (Table 8).
Latest mortality rates in Southern Europe.a

aData from EUCAN 2012
According to the GLOBOCAN projections, oral and pharyngeal cancer-related mortality (C00–14) in men in Southern European countries is highest in Croatia (6.5), followed by Portugal (5.6) and Serbia (5.3). However, the highest mortality rate in women was observed in Serbia (2.0), Montenegro (1.7) and Italy (1.5).
Taking into account Southern European countries with national cancer registries or RCRs covering a period of at least 15 years (e.g. Italy, Spain and Slovenia), and considering the overall group of C00–14 sites, a moderate decrease in mortality was observed in all these countries in the period between 1991 and 2007, with a mean figure of 3.5 at the end of that period.
Discussion
Previous studies have reported differences in cancer burden across the globe 9 and within Europe. 1,3 Differences become yet more pronounced in terms of cancer mortality. 4,5
The main strengths of the available data are that they come from common population-based registries that are available online, are regularly updated and are adapted to ICD-10. These registries include the European Cancer Observatory (EUCAN) and the Association of Nordic Cancer Registries. The weaknesses of cancer registries have been described elsewhere, with attention drawn particularly to the need to measure their completeness regularly, and to apply more quantitative methods; this can have implications for the timeliness of data publication. 10 The registries of some Eastern European countries do not cover the entire population, are not adapted to the ICD-10 classification, and data may sometimes be unavailable (e.g. Kazakhstan and Siberia; Tables 9 to 12).
Quality of data from Eastern Europe, according to parameters reported on Global Cancer Estimates (GLOBOCAN) 2012.a

Availability of incidence data: (A) high-quality national data or high-quality regional (coverage greater than 50%); (B) high-quality regional (coverage between 10% and 50%); (C) high-quality regional (coverage lower than 10%); (D) national data (rates); (E) regional data (rates); (F) frequency data; (G) no data.
Availability of mortality data (national statistics are collated and made available by the WHO for countries with vital registration): (1) high-quality complete vital registration; (2) medium-quality complete vital registration; (3) low-quality complete vital registration; (4) incomplete or sample vital registration; (5) other sources (cancer registries, verbal autopsy surveys, etc.); (6) no data.
Quality of data from Norther Europe, according to parameters reported on Global Cancer Estimates (GLOBOCAN) 2012.a

Availability of incidence data: (A) high-quality national data or high-quality regional (coverage greater than 50%); (B) high-quality regional (coverage between 10% and 50%); (C) high-quality regional (coverage lower than 10%); (D) national data (rates); (E) regional data (rates); (F) frequency data; (G) no data.
Availability of mortality data (national statistics are collated and made available by the WHO for countries with vital registration): (1) high-quality complete vital registration; (2) medium-quality complete vital registration; (3) low-quality complete vital registration; (4) incomplete or sample vital registration; (5) other sources (cancer registries, verbal autopsy surveys, etc.); (6) no data.
Quality of data from Western Europe, according to parameters reported on Global Cancer Estimates (GLOBOCAN) 2012.a

Availability of incidence data: (A) high-quality national data or high-quality regional (coverage greater than 50%); (B) high-quality regional (coverage between 10% and 50%); (C) high-quality regional (coverage lower than 10%); (D) national data (rates); (E) regional data (rates); (F) frequency data; (G) no data.
Availability of mortality data (national statistics are collated and made available by the WHO for countries with vital registration): (1) high-quality complete vital registration; (2) medium-quality complete vital registration; (3) low-quality complete vital registration; (4) incomplete or sample vital registration; (5) other sources (cancer registries, verbal autopsy surveys, etc.); (6) no data.
Quality of data from Sothern Europe, according to parameters reported on Global Cancer Estimates (GLOBOCAN) 2012.a

Availability of incidence data: (A) high-quality national data or high-quality regional (coverage greater than 50%); (B) high-quality regional (coverage between 10% and 50%); (C) high-quality regional (coverage lower than 10%); (D) national data (rates); (E) regional data (rates); (F) frequency data; (G) no data.
Availability of mortality data (national statistics are collated and made available by the WHO for countries with vital registration): (1) high-quality complete vital registration; (2) medium-quality complete vital registration; (3) low-quality complete vital registration; (4) incomplete or sample vital registration; (5) other sources (cancer registries, verbal autopsy surveys, etc.); (6) no data.
Northern Europe
Northern European countries were grouped according to the United Nations classification, but the rates and trends in Baltic countries more closely resemble the patterns of the former communist states of Central and Eastern Europe than those of the other countries of North-Western Europe, possibly because of shared history and lifestyles. 11
The estimated age-standardized cancer incidence rates in Northern European countries in 2012 were 5.9 in men and 3.1 in women; these figures are lower than those recorded for Europe as a whole. 2 Between 1983 and 2002, rates of oral cavity cancer increased among both men and women in a number of Northern European countries, including Denmark, Finland, Iceland, Latvia, Norway and the United Kingdom. 12 The highest incidence rate among the Northern European countries corresponds to Denmark. In this country, the prevalence of smoking has decreased since 1970 and oral hygiene has improved, but it has a higher alcohol intake than other Scandinavian countries and only 12% of the Danish population eat a minimum of 400 g of fruits and vegetables a day. 13 Even though the rates of oral cancer are comparatively low among women, a steady increase has been observed in some countries, such as Denmark. As a result, the male to female ratio has decreased over the past 20 years. In 2006–2008, this ratio ranged from 12.6 in Belarus to 1.3 in Iceland. 11
It has been suggested that there might be differential reporting across regions as a result of the different resources and infrastructures available to each registry. 14
Within the United Kingdom, age-standardized incidence is highest in Scotland (Cancer Research UK, 2006; available at http://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/oral-cancer). Disadvantaged backgrounds could be differentially exposed to carcinogens and other lifestyle-related risk factors, and this could explain the disproportionate increase in incidence rates in the northern regions. 14 The lower incidence rates detected in the south of England was limited to the older age group and this implies that the differential exposure to risk factors in this age group crosses socio-economic boundaries. 15 Deaths due to other reasons in this elderly group from common risk factors may account for the lower number of deaths attributable to oral cancer.
In Northern European countries, the estimated oral cancer mortality rate in men (1.6) was lower than in Europe as a whole; however, the rates in women were similar (0.7). 2 Oral cancer survival in Nordic countries has moderately improved over time and has tended to be slightly higher in females than males. Reduction in smoking but high alcohol consumption is likely to be partially responsible for differences between countries as well as advances in therapy and standards of care. 16 Gender differences in cancer survival have been reported in Estonia, with females showing a increasing survival trend. It is likely attributable to biological factors, though other factors, such as smoking and alcohol use, treatment compliance and health behaviours, may also contribute. 17 The results reported by Innos et al 17 were consistent with the findings of the European Cancer Registry (EUROCARE-4) data analysis for cancers of mouth and pharynx, stomach, lung and skin melanoma. 18
From the mid-1990s until 2002, the prevalence of smoking in men in Estonia, Latvia and Lithuania was around 50% (compared to 29% in Finland) and was between 10% and 20% in women. 11 The high estimated incidence of lung cancer in women in Northern Europe (23.7) reflects variations in the uptake and intensity of smoking. 2 In 2010, the highest incidence rates of lung cancer in women were observed in Iceland (95) and Denmark (93). 11 Lung cancer rates in women were higher than in men in Denmark, Iceland and Sweden (35–64 years). 11 However, the trends in oral cavity cancers do differ from those of lung cancer. In particular, oral cancer rates in men have been increasing in some countries such as Denmark, while lung cancer incidence rates have declined. 11 This suggests that other risk factors, such as alcohol and HPV, may play a significant role. Sweden has relatively close prevalence estimates of smokeless tobacco use and tobacco smoking. Although trends cannot be observed from the limited data available, an increase in smokeless tobacco use has been observed in Denmark, Norway and Sweden (WHO, 2008). 19
Estonia, Lithuania, Denmark and Finland are situated in positions 1, 2, 6 and 9 in the world ranking of ‘alcohol as a cause of death’ (World Life Expectancy). According to the WHO, alcohol consumption among persons aged over 15 years in Denmark has increased over the period 1960–2010 from around 7 L to 11 L of pure alcohol per year per person (WHO, 2013). 20 Alcohol drinking at high frequency is an independent risk factor for head and neck cancers, but the association appears to be limited to cancers of the oral cavity, oropharynx/hypopharynx and larynx. 21 This could explain the high incidence of C09–10 and C12–13 cancers detected in Estonia.
The estimated proportion of oropharyngeal cancers attributable to HPV varies between 17% in Southern Europe and 38% to 39% in Northern, Western and Eastern Europe. 22 Of particular note is the steep rise in the incidence of oropharyngeal cancer in Denmark in both sexes. 16 In a nationwide study performed in Denmark over a period of 30 years, from 1978 to 2007, the incidence rates for cancer at HPV-associated sites showed a marked increase, whereas cancers at sites probably not related to HPV decreased in men and showed virtually no change in women. 23 The incidence rates for tonsillar cancer in Denmark increased significantly between the periods 1978–1982 and 2003–2007, from 0.63 to 2.61 in men and from 0.25 to 0.88 in women; by 2007, more than half the cancers at HPV-associated sites were tonsillar cancers involving the Waldeyer ring. 23 Even though no cases of tonsillar cancer have been recorded in the Swedish population in some international registries between 2003 and 2007, 24 it has been suggested based on data from the Swedish Cancer Registry that the incidence of tonsillar cancer has increased in the past 30 years by 2.6% per year in men and by 1.1% in women. 25 The incidence of HPV-positive cancers is increasing in the County of Stockholm, and practically all tonsillar malignant neoplasms will perhaps in the future be HPV positive, as has been observed with cervical cancer. 26 Similar marked increased trends in oropharyngeal cancer have been reported from Scotland. 27
Eastern Europe
Eastern Europe is one of the areas with the highest age-standardized incidence rate of oral cancer worldwide (9.1). 2 In terms of tumour sites, the high incidence of cancer of the lip detected in Slovakia, particularly in certain south-western districts 24 and in some regions of Poland (Kielce Regional Cancer Registry Profile Page; available at http://www.iacr.com.fr/index.php?option=com_comprofiler&task=userprofile&user=1056&Itemid=498), probably corresponds to areas where the majority of the population is still engaged in agriculture and in other outdoor occupational activities, as has previously been reported. 28 The increasing incidence of neoplasms of the tonsils and oropharynx were detected in some countries such as Slovakia, the Czech Republic and Poland. The highest values in men correspond to Hungary (18.7), Slovakia (14.0) and Romania (13.6); in women, the highest rates are observed in Hungary (3.3), Slovakia (1.3) and Poland (1.2) (HPV Information Centre).
The estimated mortality rate in men in Europe in 2012 was 3.0 and in the Central-Eastern European Region reached 5.1. 2 Overall, cancer mortality in Europe has been steadily decreasing since the early 1990s. However, cancer burden in the Central and Eastern European countries is substantial and still continues to rise in some Eastern European countries, with exceedingly high rates recorded in Hungary and Slovakia (IARC); mortality is also increasing. 29
Oral and pharyngeal cancer mortality rates are comparatively low in European women, though trends have been rising over the last decades, and rates in some countries such as Hungary and Romania have reached relatively high levels. 30 This is not surprising, given that smoking and alcohol consumption have not declined in European women as in men. 19
Mass cigarette use followed economic development in Europe, initially in Northern and Western Europe, followed by Southern Europe, and finally Central and Eastern Europe. 11 Lung cancer is now the most common cancer in men worldwide, with highest rates in Central and Eastern Europe. 2 Oral cancer incidence rates have been higher in men than in women, but the converging male and female incidence trends over the past 20 years have produced a fall in the male to female ratio during this period. 11 In Russia, tobacco smoking rates in women were reported to have more than doubled (from 7% to 15%) between 1992 and 2003. 31 In the ‘smoking as a cause of death world rank’, Russia and Ukraine are in the top 10 for men, while the Czech Republic and Bulgaria are in the top 10 for women (World Life Expectancy).
Oral cancer mortality trends and geographic patterns also appear to be related to changes in alcohol consumption. The exceedingly high rates in Hungary and in a few other countries of Eastern Europe can be related not only to the overall quantity of alcohol consumed but also to the drinking pattern and to the type of alcohol consumed (alcohol derived from fruit and home-made alcoholic beverages are widely consumed and may contain high levels of the carcinogen acetaldehyde). 32 Belarus, Russia and Ukraine are found in positions 3, 4 and 5 in the ‘alcohol as a cause of death world rank’ (World Life Expectancy).
With regard to oral cancer, Hungary ranks first among European countries for both morbidity and mortality. 33 Although some degree of overestimation might exist, it has been suggested that the Hungarian National Cancer database and its effects on current cancer data collection activities is exemplary in Europe. 34 Clinical stage has the most significant impact on survival and the most important high-risk habits in north-eastern Hungary are smoking and alcohol consumption. 35 Smoking correlates with advanced clinical stages and drinking habit correlates with tumour site. 35 However, the increase in oral cancer-related morbidity among elderly women and young adults who do not smoke or drink alcohol suggests that other factors – probably including some gender-specific systemic risk factors – may also play a role in the pathogenesis of oral cancer. 33 Although the majority of patients are diagnosed with early stage lesions and moderately differentiated tumours, the 5-year overall survival rate is below 40%. 35 Hungary leads the male mortality statistics in smoking-related lung and oral cavity cancer. Additionally, Hungary ranks first for female mortality due to colorectal cancer and leukaemia. 36 This high mortality rate has been attributed to cigarette smoking, excessive alcohol consumption, and inequalities in the care received by cancer patients. 37 In Hungary, 36.1% of the adult population smokes cigarettes and 40.6% of men and 31.7% of women smoke regularly, suggesting an increase of smoking among women. 38 In Europe the number of medical consultations per person per year was highest in Hungary and the numbers of magnetic resonance imaging units and computed tomography scanners per million population were lowest in Hungary and Romania 39 ; however, in 2008 Hungary had the lowest ratio of cancer cases per medical oncologist among 12 European countries. 40 Other factors require further deliberation, including high levels of contaminants in drinking water and food (e.g. a high arsenic concentration increases the incidence of lung cancer), 41 and high atmospheric concentrations of small particulate matter detected in Central and Eastern regions of Hungary correlated strongly with lung cancer incidence. 42 A possible association with oral cancer requires exploration. In a pooled database including 11 national cohorts, Hungary showed the highest cancer risk driven by chromosome-type aberrations. 43
Western Europe
The incidence of oral and pharyngeal cancer in France has traditionally been high in both men and women and has shown marked geographical variability, with a higher incidence in the north, east and west of the country compared with the south. 44 In areas of the north of France, oral cancer is still the most common one in men. 45 Geographical variability is also observed in Belgium, with a higher incidence of oral and pharyngeal cancer in the south, on the border with France, and a lower incidence in the north, at the border with the Netherlands. Additionally, a strong association between oral and pharyngeal cancer and the prevalence of chronic liver disease has been detected in Belgium, supporting a possible aetiological association between alcohol and oral and pharyngeal cancer. 46
The rates detected in Germany are similar to those of other Western European countries, with an incidence rate that is typically higher than in Northern or Southern Europe and that tends to be similar to rates in Eastern and Central European countries. 3 However, although the incidence and mortality appear to be decreasing in the younger age groups, the opposite is observed in the older population. The incidence is higher in men in all age groups and for all oral cancer sub-sites. 47 The decreasing incidence in the younger age groups mirrors the incidence patterns observed in the Netherlands, 48 though this is not a universal phenomenon, as evidenced by the increasing incidence in the younger population in the United Kingdom. 49
Lip cancer is associated with specific aetiological factors, particularly prolonged sun exposure, outdoor occupations, socio-economic level, smoking and host-related factors. In the Netherlands, with the highest incidence of cancer of the lip, in the Western European countries, a strong association has been shown between this cancer and residence in rural areas, both for men and for women. 50
Southern Europe
In Portugal over the past decade, the incidence of oral and oropharyngeal cancer has shown a tendency to increase in both men and women, but particularly in women; this has typically been attributed to high rates of smoking and high alcohol consumption. Although smoking has decreased throughout Europe in recent decades, the reduction has been slower among women. 51 Moreover, although alcohol consumption has fallen since the beginning of the past century, in 2005 Portugal was the country ranked fourth in the world for per-capita wine consumption (WHO, 2011). 52 In addition, the consumption of beer and distilled beverages has increased, particularly in women. In recent years, excessive alcohol consumption (binge drinking) has increased among Portuguese women, although its impact on the incidence of oral cancer has not yet been determined. 53 Other risk factors, including socio-economic exclusion and a diet poor in fruit and vegetables, may also contribute to increased incidence rates of oral cancer, 54 although the impact of these factors on the incidence rates of oral and oropharyngeal cancer in Portugal is unknown. An alarming lack of knowledge regarding the risk factors for oral cancer in the Portuguese population has been documented raising the need to improve health literacy. These societal factors need attention if we are to expect any reversal of increasing trends in oral and oropharyngeal cancer in that country. 55
In Spain, predictions indicate a reduction in the difference between men and women in the incidence of head and neck cancers, including oral and oropharyngeal cancer. 56 In recent years, there has been a fall in the incidence rate in men and an increase in women, a reflection of the changes in smoking and alcohol consumption. The traditional gender difference in the prevalence of smoking in Spain has reduced due to an increase in the number of women who smoke, particularly in the younger age groups (National Health Survey, Spain; available at http://www.msc.es/estadEstudios/estadisticas/encuestaNacional/home.htm).
If the number of women who smoke continues to increase, predictions indicate an increase in the incidence of head and neck cancers. The incidence of cancer of the lip is also particularly high in Spain. The city of Granada is traditionally considered to be the area with the highest incidence of lip cancer in Europe, although it has recently been overtaken by Cuenca, a city in central Spain, close to Madrid. But in the case of Cuenca, there continues to be a marked gender difference in favour of men. 57 In contrast, the incidence of lip cancer reported in public hospitals in Madrid has been falling since 2001–2002. 57
Conclusions
This study confirms the heterogeneous distribution of oral and pharyngeal cancer in Europe in terms of incidence and mortality (Figures 1 and 2). These regional differences are evident not only between north and south and between east and west but also within single regions (e.g. between the Scandinavian countries and the former Soviet republics). These findings reflect differences in lifestyle and in exposure to risk factors such as smoking (e.g. high incidence in Danish women), alcohol (e.g. in Lithuanian men) or both (e.g. the increasing incidence in the younger population in the United Kingdom). Furthermore, other traditional factors that have typically been underestimated, such as actinic radiation, are responsible for a considerable number of cases of lip cancer (e.g. Spain), and identification of the oncogenic potential of HPV explains the increase in oropharyngeal cancer in some regions (e.g. Denmark and Scotland). The challenges we now face, based on these results, are to update the registries and achieve universal coverage, to individualize preventive policies adapted to the socio-economic and cultural characteristics of each region, and to investigate in detail some of the more interesting findings, such as the high incidence of oral cancer in Hungary, which has still not been fully explained.
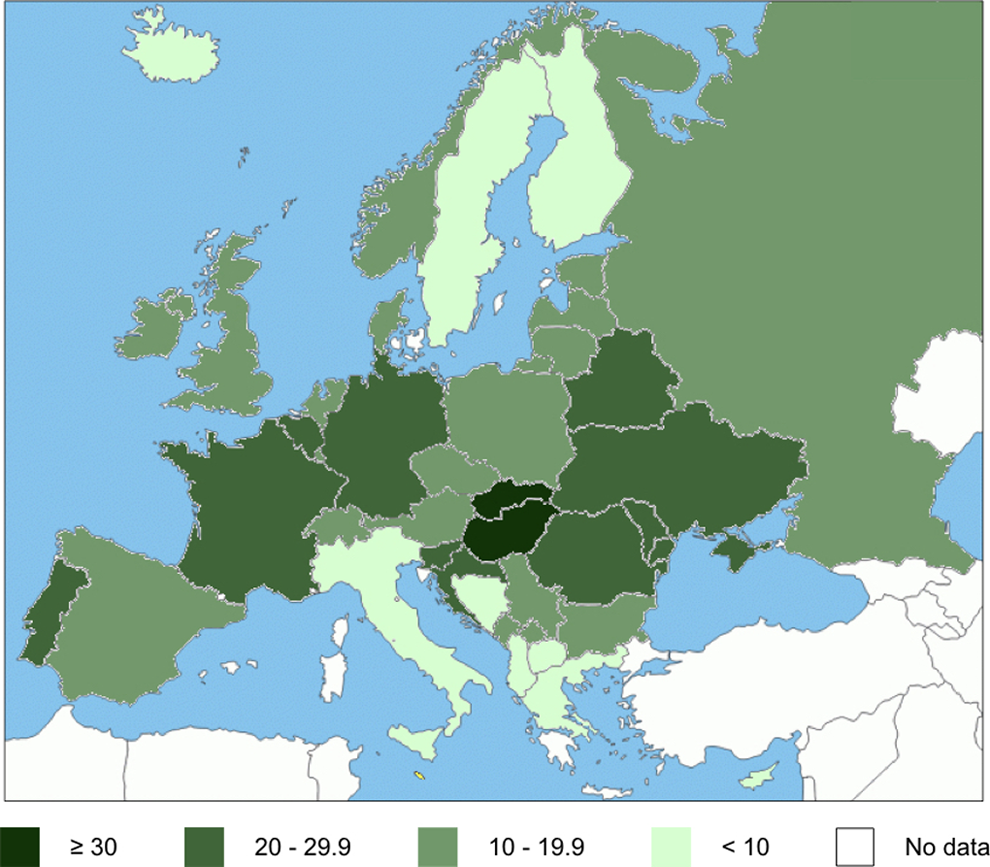
Incidence of oral and oropharyngeal cancer (C00-C14) among male in Europe (age-standardized rate per 100,000 person-years).

Incidence of oral and oropharyngeal cancer (C00-C14) among female in Europe (age-standardized rate per 100,000 person-years).
Translational value
The challenges, based on these results, are to update the registries and achieve universal coverage, to individualize preventive policies adapted to the socio-economic and cultural characteristics of each region, and to investigate in detail possible reasons for some of the major findings, such as the high prevalence of oral cancer in Hungary, which has still not been fully explained. During policy development, the governments in high-risk countries in Europe should give priority to the establishment of oral cancer preventive programs.
Footnotes
Authors’ Note
This study was presented at the Global Oral Cancer Forum held in New York, USA, in March 2016.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The forum received funding from Henry Schein Cares Foundation.