
Abstract
Nurses’ professional conduct and work-related well-being are crucial for providing high-quality, safe patient care. Previous knowledge about nurse managers’ early interventions in nurses’ professional conduct is scarce. The aim of this study was to describe how nurse managers intervene in registered nurses’ professional conduct, based on the documents of early intervention and support. A retrospective, cross-sectional document analysis with inductive content analysis was conducted on 43 documents of an early intervention and support program for registered nurses in one Finnish hospital between 2019 and 2021. The manuscript and reporting of the findings were guided by the Standards for Reporting Qualitative Research checklist. The concerns about nurses’ work-related well-being and their working initiated the early intervention process. Nurse managers’ early interventions included supportive and strength-based approaches. These involved appreciating the nurses’ own awareness of their ability to work and supported the process, as did a collaboration with occupation health and other support services. More knowledge is needed about the influence of early intervention programs and nurses' and managers' awareness of different methods.
Keywords
Background
Professional conduct is a prerequisite for carrying out nursing work. It is every nurse’s duty and requires nurses to have knowledge-based and ethical expertise. 1 Nurses are made aware that they must have the professional abilities and good health to practice in order to provide quality, safe care.1–4 Nurses’ professional conduct can be weakened by their health issues. It can also be impaired or deficient, due to incompetence or their reduced ability to work,5,6 inadequate knowledge, skills, or work performance. 5 Such deficiencies are marginal, but they can increase the potential risks for errors, reduce patient safety,7–9 and influence nurses’ working careers.10,11
Nurse managers have a duty to create a safe working environment and ensure that all staff meet professional standards.12–14 They are responsible for the welfare of their staff and running their organization. They do this by supervising and intervening in nurses’ professional conduct, maintaining their occupational health, and supporting their work.11,13,15,16 Nursing practice can involve burdens 7 that create challenges for nurses’ well-being, such as work-related stress and mental health problems.8,9 These can affect their working life and have been associated with medical errors.7,17 That is why nurse managers play a crucial role in recognizing the early signs of nurses’ deteriorating well-being and professional conduct.10,12,18,19 Nurse managers supervise staff through discussions and monitoring. They also handle serious violations of nursing standards at the organizational level and set administrative sanctions, such as restrictions, warnings, or terminations of working contracts.14,20 Controlling absences due to sickness can help nurse managers to address the early signs of weakening work ability and help nurses to stay at work, or continue to work, after a work absence. 21
Previous studies about the early supervision of nurses’ professional conduct issues have dealt with the difficulties in identifying mental health issues that affect their professional competence 8 and monitoring substance abuse.22,23 In addition, previous studies have looked at strengthening the role of nursing managers, so that they can help nurses to stay at work 11 and addressed the effective supervision of enablers and barriers to work. 16 It is essential that nurse managers know about, and manage, early intervention programs. 24 These are needed to help nurses to access support 11 and maintain the required occupational well-being that enables them to have the professional ability to practice. 25 Nurses can be supported to continue in their role through workplace interventions that ensure their autonomy at work. These can involve their supervisors, professional and organizational support, including collaboration with occupational health professionals, and providing changes in working role. 11
Recent studies have highlighted the importance of the dialogue between employees and supervisors in early intervention processes.11,24 Early intervention aims to create a shared understanding that includes the employee's individual needs, enhancing their knowledge and skills, and improving the service they provide. 9 Understanding why nurses want to leave nursing has been addressed 26 and this is important when it comes to finding ways to help them to stay in their roles 11 and prevent work-related stress. 27 Identifying employees’ work-related problems as early as possible can reduce absences due to sickness. 28 Previous studies have indicated the need for further knowledge about multilevel and multipronged approaches to early interventions and support, as well as the relative effects of different approaches to employees’ well-being. 8 In addition, the need for clear structures for early interventions has been addressed, 24 especially when monitoring nurses’ substance abuse problems.22,23 Nurse managers need to understand what supports or undermines nurses’ professional conduct in order to achieve effective supervision.
Aim
The aim of the present study was to describe how nurse managers intervene in registered nurses’ professional conduct, based on the documents of early intervention and support. The research was guided by two research questions:
What kind of concerns about nurses’ professional conduct have been reported? What kind of early interventions have nurse managers used?
Method
Study design
This was a document analysis study, with a retrospective, cross-sectional qualitative design.29,30 It used a purposeful sampling and followed seven phases of document analysis. 30 The manuscript and reporting was guided by the Standards for Reporting Qualitative Research (SRQR) checklist. 31
Research environment
This study was conducted in one Finnish public university hospital that used an organizational program to provide early intervention and support for staff. The program was based on the national guiding 21 and uniformly applied in whole hospital district. The goal of the program was to help staff and supervisors to identify possible risks in an employee's ability to work, support them to continue to work, and reduce their sickness absences. The process could be activated by nurse managers or other professionals in response to early signs or changes in an employee's working. These signs related to managing working tasks or time, behavior, work motivation or suspected substance abuse. Different monitoring programs were used side by side and each could activate the early intervention and support process if the matter related to nurses’ professional conduct. The process could also lead to procedures of disciplinary sanctions. The program comprised three phases and discussions, depending on the seriousness of the case, and each involved filling a structured document by the employee and the manager, either electronically or by hand. The document contained an investigation of the employee's ability to work, assessments of the situation, and plans for performing at work, staying at work, or returning to work after an absence. The documents were securely stored by the supervisors.
Data collection
After receiving research permission from the organization that agreed to take part, the researcher (OP) contacted the administrators and asked them to provide documents on early intervention and support program from 1 January 2019 to 31 December 202129,30 that were held between registered nurses and their managers. A half-structured data extraction matrix was created based on previous literature5,6,12,32,33 and the structure of the early intervention and support program. The matrix included three open fields about the attentions of nurses’ professional conduct, issues influencing the nurses’ ability to practice, and how nurse managers intervene and support nurses.
The data were collected according to the pre-defined inclusion and exclusion criteria. The matrix was pilot tested after five documents were reviewed. Two documents were excluded as they did not relate to registered nurses. The research data consisted of 43 early intervention and support documents, with 167 sheets of paper, in the range of 1–12 pages in each case. The researcher (OP) manually transferred the information from the original documents to the electronic data extraction matrixes, which were randomly numbered. All the expressions were collected from each document according to the extraction matrix and research questions. 30 In this study, the term nurse is used to describe the target group, registered nurses.
Data analysis
The data were analyzed using an inductive content analysis. 34 At first, the data were read through to get an overall understanding of the material. NVivo12 analysis software (12.6.1.970 plus QSR International, 2017) was used to code the qualitative information and quantify the frequencies of the analysis units. These were the words, groups of words, and partial or full sentences of the 1261 original expressions. Analysis units were grouped together with similar contents and, after that, clustered together to 23 sub-categories, abstracted into seven categories, and then into two main categories.29,34 The categories were named based on their contents at each stage. The main categories were named such as the concerns raised about the nurses’ professional conduct and the early intervention methods used by the nurse managers. The results were supported with original quotes, with the professional role of their presenters and the random number of the document. The data collection and analysis were conducted by one researcher (OP) and then the entire research team participated in conducting the research (OP, AHL, MK).
Ethical considerations
The study was conducted according to ethical scientific guidelines.35,36 The research data were processed so that it was not possible to identify stakeholders. This type of study design does not require an ethical review statement from an ethical committee. 37 The research permission was given in December 2021 by the participating organization and subjected to the researcher protecting the research data. The administrator of a register had right to provide anonymized documents for research use. An internal public announcement about the research gave the stakeholders an opportunity to withdraw their documents from the research. To protect their anonymity, any background information about the stakeholders was not collected, except for their professional degree or title.
Rigor of the study
The rigor of the document analysis involved decreasing potential bias with regard to the purpose, selection, and authors of the documents, together with the selected data and interpretation and reporting. 30 Purpose bias related to the fact that documents recorded the early interventions that the employees received, and these were not designed for research use. This meant that they could contain irrelevant information or lack essential information for the research purpose. Selection bias referred to the possible limited availability of the protected documents. This was avoided by targeting data collection to a certain period. Pilot testing of the data extraction matrix strengthened the reliability of the data collection. Author bias related to the authorship of the documents, as they were filled in by both the nurses and their managers from different points of views. However, the forms contained structured topics and focused both parties’ attentions, which strengthened the data collection. Data and interpretation bias referred to not collecting the documents that were not directly filled in by the nurse or their managers or included inaccuracies. 29 However, none of the documents were not excluded on this basis. In addition, potential reporting bias was considered by describing the document analysis process closely. 30
Results
Concerns about nurses’ professional conduct
The documents showed that the early intervention and support process was initiated by 435 concerns about nurses’ professional conduct, which were raised by colleagues, nurse managers, or the nurses. The concerns related to the nurses’ work-related well-being (n = 254), their compliance with the work framework (n = 154), and their competencies to implement patient care (n = 27) (Table 1).
Descriptions of the concerns about nurses’ professional conduct, reported by the nurses, their colleagues, and nurse managers.
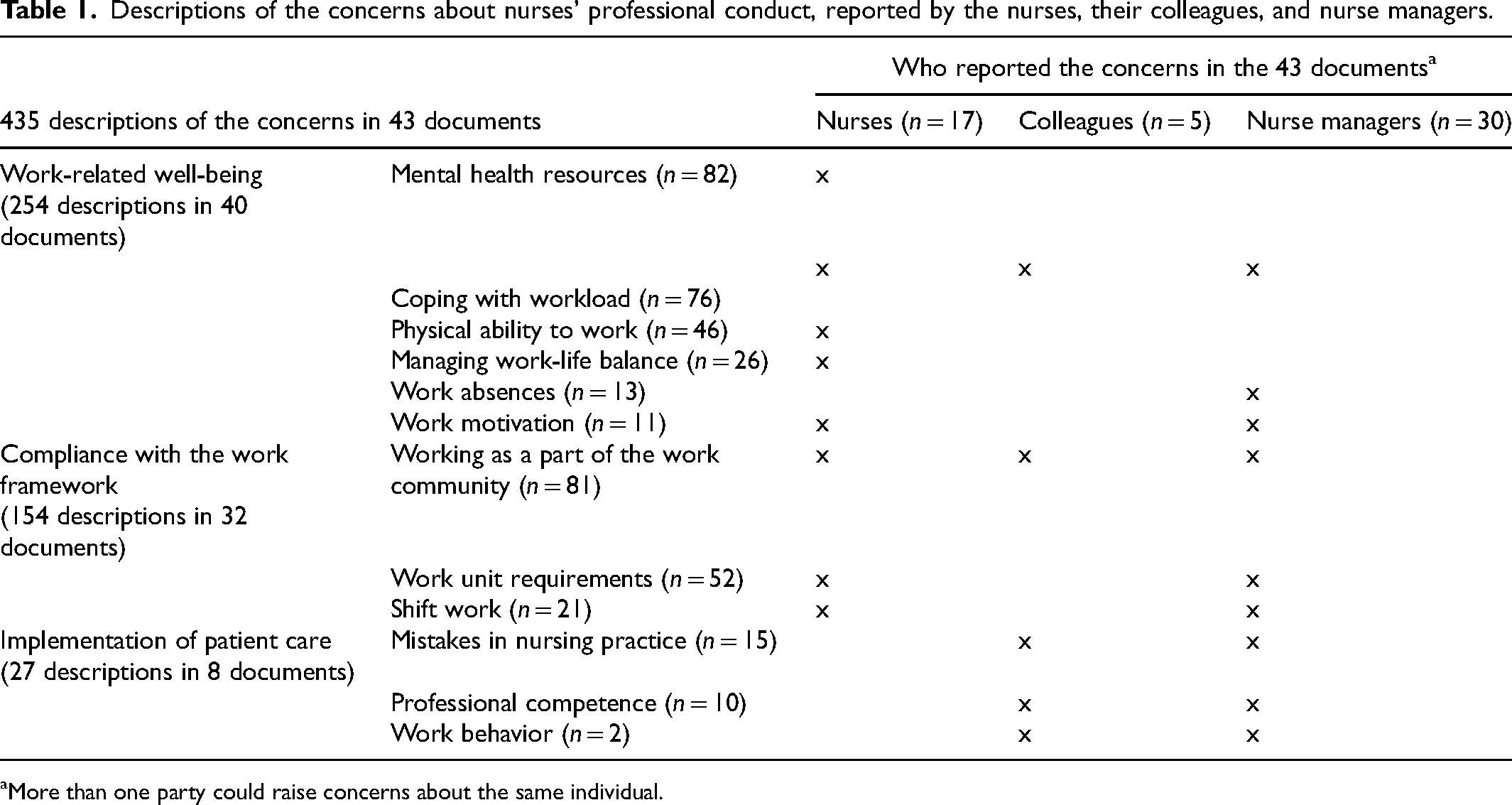
More than one party could raise concerns about the same individual.
The concerns about the nurses’ work-related well-being included their mental health resources. These related to the factors that affected their ability to work, namely burn out, sleeping problems and insomnia, depression, and anxiety. Some of them had difficult to cope with their workload, which manifested itself as fatigue, stress, burden, overload, concentration issues, and reduced work performance. Some of the nurses also had memory problems. Some of the nurses had challenges in managing work-life balance, because of issues in their private life, such as family, relationship, or financial situations. Some lacked the work motivation or commitment to work. The nurses raised concerns about their own health and how it influenced their work and limited their ability to manage certain nursing practices or tasks. Some reported about their reduced physical ability to work, as a result of long-term symptoms due to conditions, injuries due to physical traumas and respiratory symptoms. The documents showed that some managers had raised concerns about the nurses’ continued or prolonged sick leave (Table 1). “Nursing practice requires physical strength and that is practically impossible for me at the moment. I feel that I am capable of working in a nursing job that does not require physical effort.” [Nurse in document 28] “The nurse only had two sickness absences in the previous year, but during this year there have been six sickness absences with a physician's certificate.” [Manager in document 29]
Nurses’ compliance with work frameworks raised concerns relating to their ability to manage shift work, such as three-shift pattern or night work. Some could also have inadequate contributions to the working community. Some nurses found it challenging to meet the conditions required by the work unit and the nature of the work, including the hectic nature of the work or work pace. In addition, some of them had challenges with working environment issues, such as working in large facilities, with lots of equipment and long distances, indoor air problems, or working in isolation rooms. Issues related to the working community influenced a lot on some nurses’ working life. Some of them had experienced isolation and bullying. Some nurses expressed their own need to change their work, working time, or environment. Concerns about patient care included mistakes by the nurses in nursing practice that could risk patient safety and were reported by their managers and colleagues. Some had also issued about unusual or unprofessional work behavior. In this context, some nurses neglected nursing tasks and patient records and had errors in monitoring or medication administration. In addition, some of them had a lack of basic nursing skills, incorrect working, or problems handling health technology or equipment. “The staff provided feedback about the nurse that were related to patient care, such as insufficient recording and patient care tasks that were not done.” [Manager in document 41] “The work environment is really challenging, including cramped, indoor air problems and too much noise. Having to hurry. The responsibility is sometimes too hard.” [Nurse in document 11]
Early interventions by nurse managers
The documents showed that the nurse managers created an understanding of the nurses’ situations, strengthened their professional capability, and reshaped their working arrangements. These were established with a confidential atmosphere, by recognizing the nurses’ strengths and analyzing their current situations. They also monitored the nurses’ progress as part of the early intervention process (Figure 1).
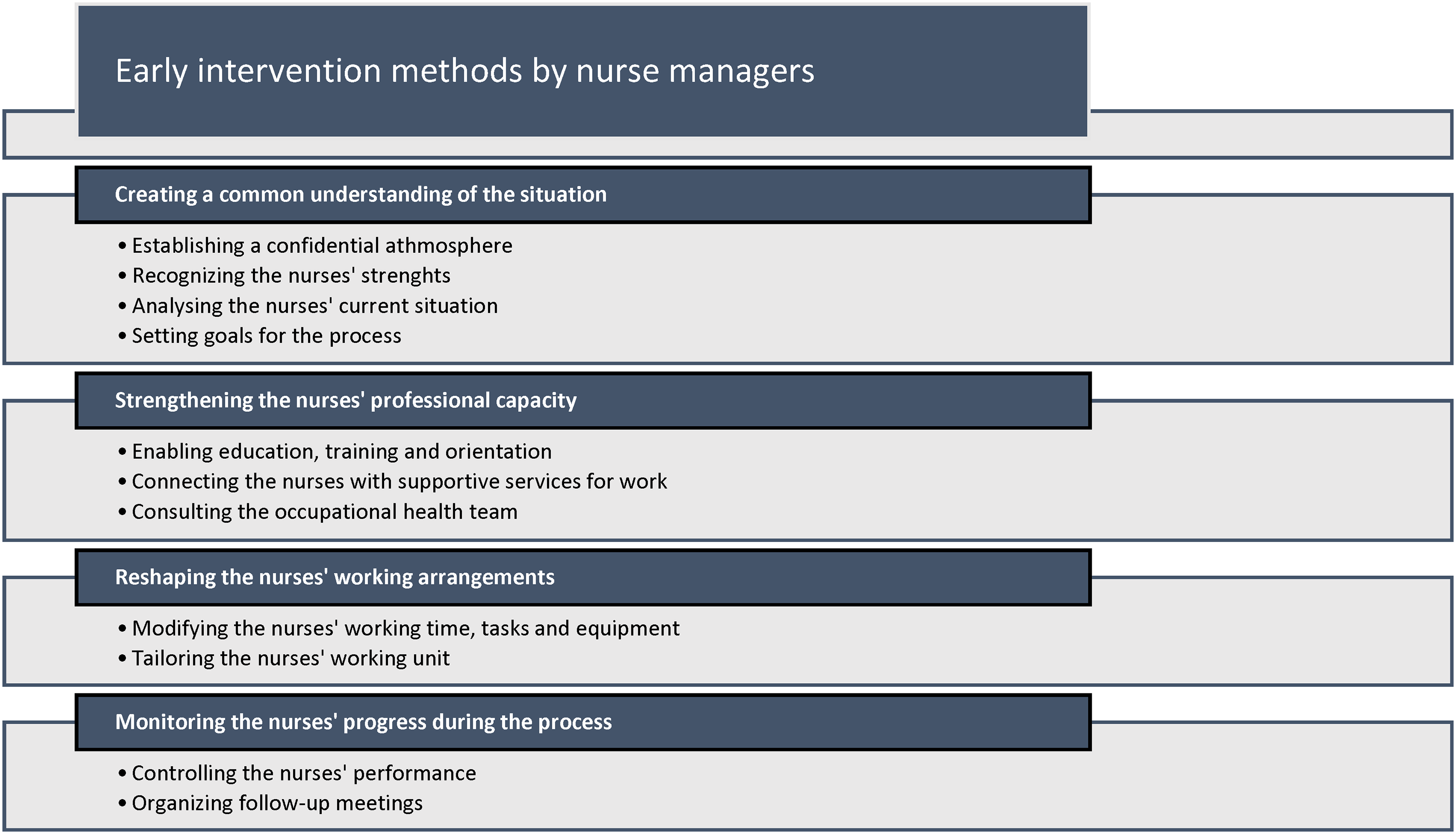
Nurse managers’ early intervention methods: categories and sub-categories.
The conversations were enhanced by respect, understanding and skilful communication, openness, and trust. The nurses and their managers set goals for the process. Some documents detailed open conversations with the working community, especially about changes to working arrangements. The nurses described numerous supportive factors for their own ability to practice. These were good work motivation, their ability to cope at work, and external factors that supported their coping and well-being, such as physical exercise and hobbies, resting and socializing, and the support they receive from their close ones. A supportive working community was also mentioned. Nurse managers often recognized the nurses’ good professional competence. In some cases, they had not recognized the early signs that related to the nurses’ reduced ability to work. “The supervisor is easy to approach, flexible and understanding, and does not confuse too many nurses.” [Nurse in document 01] “The employee performs the required work responsibly. The employee's fatigue has not been reflected in work performance and that came as a surprise to the supervisor.” [Manager in document 10]
The nurses’ current situation was assessed by examining their current working arrangements, such as working time, shifts, and tasks and how well they managed them. In a few cases, the length of the nurses’ working career and the permanent or temporary status of the nurses’ working contracts were reported . Several nurses had received previous early intervention and support, including orientation, development and work ability discussions, work ability assessments, and three-part meetings (an employee – a manager – occupational healthcare team) to evaluate their working ability. The goal for the program was to set a common agreement between the nurses and their managers that was primarily based on the nurse's individual needs and wishes. In some cases, the progress of the process was hindered due to the nurse's personal reasons, such as health issues. “I have a three-shift job. I have done a lot of night shifts over the last 35 years because I like them, and they fit into my routine.” [Nurse in document 37] “We came up with a joint plan of measures. Based on the discussion, we agreed that we would schedule a joint appointment for occupational healthcare, where we would review the situation and further plans.” [Manager in document 27]
During the early intervention process, the nurse managers aimed to strengthen the nurses’ professional capacity. The nurses were offered retraining, education, and learning new nursing tasks (Figure 1). In addition, the organization's personnel work planner was used when the nurses’ working patterns were rearranged. The managers also helped the nurses by involving occupational healthcare services. Their well-being was also supported by rehabilitation, physiotherapists, and occupational psychologists. The managers consulted occupational healthcare officials and asked them to assess the nurses’ health and work ability, if needed. In some cases, the process was inhibited due to the limited availability of occupational healthcare services. “I asked the department pharmacist to provide training for the employee.” [Manager in document 26] “The employee is in contact with occupational healthcare about the possibility of getting a psychologist's appointment.” [Manager in document 09]
The documents reflected how the nurses’ wishes and their managers’ suggestions reshaped the nurses’ working arrangements. These changes were based on a shared plan, including modifying their working time or tasks, working environment, the equipment they used, and tailoring their working unit (Figure 1). The revised arrangements included working part-time, not working nights shifts, and having extra holidays and free days. Some managers suggested that the nurses had regular shift rhythm, longer breaks between shifts, or only worked day shifts. In addition, the nurses’ work-life balance was supported with an autonomic shift planning. The documents showed that working environments could be improved by ergonomic equipment or different room arrangements. Nursing tasks were also rearranged to help the nurses avoid heavy tasks, such as taking care of bed-bound patients. Tailoring the nurses’ working unit referred to wide arrangements that did not just concern the current working unit. Those included work cycles, relocation, and work trials in another unit, department, or organization. Some of the nurses received pensions, were able to partly retire, or had sick allowances that enabled them to modify their working time. However, some documents described organizational or administrative constraints that meant it was not possible to change the nurses’ work arrangements. These included the need for a three-shift working pattern and no options to make the role less demanding or swap the nurses with members of staff from other units. Some communications between nurses and their managers were challenging. “Part-time work aims to support coping at work and the smooth running of family life, as well helping the employee to cope.” [Manager in document 14] “It is impossible to choose an easier job when it comes to working tasks.” [Manager in document 35]
The managers monitored the nurses’ progress in the process. This included controlling the nurses’ performance and organizing follow-up meetings in close collaboration with occupational healthcare (Figure 1). Some documents referred to three-part meetings, if needed. Steering and follow-up meetings also supported the nurses’ progress. Some nurses’ work performance was controlled by requiring that they only obtained sickness absence certificates through occupational healthcare. Nurse managers also restricted the nurses’ nursing tasks and provided re-training, for example on certain medical treatments. Some documents indicated that the early intervention process ended when the nurse was got a new job in another department or if no new follow-up meeting were agreed. “We will review the situation next spring and the employee says that she will be in touch earlier if the situation changes or if she feels that she needs support.” [Manager in document 24]
Discussion
This study conceptualized nurse managers’ early interventions for nurses’ professional conduct and produced new knowledge on the topic. Previous studies have focused on serious supervision issues relating to nurses’ professional conduct.6,20 This study showed that most of the concerns raised in the documents dealt with the nurses’ well-being at work. The nurses themselves were often the initiators of the early intervention processes. This underlines the nurses’ important role in detecting problems at an early stage and preventing any severe consequences from their deficient professional conduct. Nurse managers and colleagues had noticed to more evident problems in the nurses’ professional conduct, such as compliance with the work framework and implementing patient care. Concerns about patient care were the least documented. This may be interpreted as the success of the early intervention methods that the nurse managers had used. These included showing appreciation of the nurses and adopting a supportive and strength-based approach, rather than supervising in a controlling way or even blaming the nurses. These kinds of approaches have been used in serious issues and when nurses were facing disciplinary actions.33,38
Previous studies have focused on early signs of nurses’ deficient professional conduct, such as avoiding tasks, taking long breaks, or being absent from work due to substance abuse.22,23 However, very few similar descriptions were documented in this study. The early concerns that nurses expressed themselves in this study tended to be mental health issues, such as stress, fatigue, burn out, sleeping problems, depression, and anxiety. Studies have indicated that these are common among nurses.25,27,39,40 The findings that nurses’ self-initiative in bringing out issues relating their work ability highlight their own awareness and ability to evaluate and recognize their own professional conduct. Nurses can avoid asking for help because of the stigma of health issues. Tensions with people they work with and a lack of discussions about professionalism can exacerbate their reluctance. 8 The courage that nurses show in seeking help, and their own ability to evaluate their own professional conduct, is a strength that organizations need to appreciate. The nurses’ own awareness of their issues must be taken into account when developing early interventions, as shown in studies about the relationships between an employee's competence and the quality of care they provide.15,39,41 Managers also need to be able to accept the nurses’ own concerns and take them into account when they assess their work ability. The early intervention documents reviewed during this study revealed concerns about nurses’ deficient professional conduct. A more comprehensive understanding of the phenomena requires further studies that use different methodological solutions, such as interviews with nurse managers and colleagues. Previous studies18,19 have shown that some concerns are difficult to bring up and further studies may suggest different ways to do this.
The nurses’ current situations, and the possible limitations of staying in their jobs, were defined by the nurses and their managers together. Reaching a consensus about the nurses’ current situations required interactivity and discussion. Examining the status of the nurses’ work performance was based on openness, trust, and mutual understanding between the nurses and their managers. This was in line with previous studies that have addressed a need for shared understanding 16 and trusted relationships between employees and their supervisors. 11 The findings of this study implied that the nurse managers and nurses had established a trustful and safe relationship. The findings also showed that in some cases, it was difficult to progress the early intervention process due to challenges in communication or commitment to shared plan. Barriers to the effective supervision of professional conduct issues have been also shown in previous studies. These included on-site meetings, disagreements, and conflicts between an employee and a first-line manager, and employees having severe health symptoms.16,24 This underlines the need for providing nurses regular opportunities for open discussions. Being able to raise early concerns and provide interactive, resource-oriented early support can strengthen open communication.
The nurses and their managers were not the only ones involved in the early intervention process. This study showed the close collaboration with occupational healthcare. The target was to find the best solutions that enabled nurses to work and stay at work with supportive work arrangements. This study showed that the nurse managers’ attentions often focused on the nurses’ work absences, as they provided visible early signs of work-related concerns. The importance of supporting employees after long sickness absences has been highlighted in a recent study. 28 One method used by the nurse managers in this study was to tell the nurses that any sickness absence certificates should be obtained through occupational healthcare. This enabled the nurse managers and occupational health to identify any issues related to the nurses’ working capacity.22,23 More detailed documentation on early intervention processes, such as assessing whether goals had been achieved and what helped or hindered the process, would help managers to continue to help nurses. It would be easier to evaluate current situation in a more comprehensive way if all the material relating to the nurses were in one file, including their current working role, career, working arrangements, and other professional information.
The methods that nurse managers used to help the nurses to stay in their job confirmed previous research.11,26 These included providing work that was better matched to nurses’ skills, enhancing their autonomy and professional support, and making sure the organizations fulfilled their’ responsibilities, including providing safe and trustful work environments. This kind of targeted support was particularly necessary when the nurses had weakened capacity. However, previous studies have found that nurses could lack adequate support from their supervisors13,15 and nurse managers lacked sufficient options to resolve situations. 16 That is why more knowledge is needed on how nurse managers intervene and support employees and what kind of specific orientation and training they need to handle early intervention and support programs. Further studies should target supervision at an organizational level. Knowledge is also needed on what kind of structures and processes would support nurse managers during an early intervention process.
The effects of deficient professional conduct on patient care and safety due to incorrect or incomplete nursing practice cannot be denied,7–9 but the descriptions were marginal in this study. Understanding what causes errors due to nurses’ deficient professional conduct, and how often they happen, could increase the ability of nurse managers to improve safe care by preventing risks. 12 Early interventions and support are not just an issue for the nurse, as they also have an impact on their ability to provide patients with safe, quality of care. Therefore, more research on the possible risks of deficient professional conduct on patient safety is needed.
Strengths and limitations of the study
The limitation of the study was the small sample from just one organization. This meant that the causality could not be demonstrated, and it was not possible to address generalizations or geographical incidence. There were few detailed descriptions on the early intervention cases in some of the documents that were used. That is why it was not possible to report the exact concerns that triggered the early intervention and support program in all cases. The consequences for nursing practice and patient safety were rarely reported in the documents. It was not possible to describe a reprehensible professional conduct, because the organization had separate administrative supervision monitoring programs for nurses’ unprofessional conduct in place.
The validity of the study was strengthened using a trustworthy method of data collection and sampling strategy and selecting suitable units of analysis. Purposeful sampling also strengthened the reliability of the study. 30 Although sufficient descriptions were gathered to answer the research questions, wider data could have increased the credibility of the study. The original quotes in the documents supported the results, the reliability of the research, and the credibility of the analysis.31,34 The data were collected during the COVID-19 pandemic, but it was not possible to assess what impact that had on the results.
Recommendations for further research
This study suggests the need for further research into how nurse managers use early intervention and support programs in professional nursing. Providing equal access to such programs at a national level would enable wider systematic reporting and research on the phenomenon. Standardizing program documentation would support the development of early interventions and help nurse managers to discharge their duty to provide professional supervision. It would also enable systematic and wider research use of the associated documents in future. The early intervention methods identified by this study could help to develop future documentation and increase nurse managers’ awareness of the process.
This study also recommends that more research is needed about the benefits of early intervention and how nurses could be supported in the future. Nurses should also be taken involved in the development of early intervention methods. Further research is needed on the interventions that nurses feel are useful and support them at work and their nursing career. In addition, it needs to be established how nurse managers use different early intervention methods and are able to evaluate them. Understanding of nurses’ deficient professional conduct could be enhanced by using other documents produced by nurse managers when they are supervising good work behavior protocols and tackling substance abuse.
Practical implication
This study conceptualized early intervention by nurse managers to nurses’ professional conduct. This new knowledge can be used to inform the development of future programs and to enhance nurse managers’ training and awareness about the phenomenon. Nurse managers who are helping nurses could be supported to manage nurses’ working and to stay at work by identifying deficient professional conduct, developing the reporting and implementation of early intervention and support methods. The findings could also help to deepen our understanding of the influence that deficient professional conduct has on patient safety and nursing careers and the need for initiatives that reduce risk, promote safety, and help to keep nurses at work.
Nurse managers can reinforce professional conduct by paying more attention to the early signs that nurses’ abilities to work are being impaired and provide early interventions to prevent those issues from significantly affecting their work performance. This could also help nursing workforce to stay in their role. Interactive support and strengthening resource-oriented approaches should include in early intervention methods. In these must be considered the nurses’ own work activities and their awareness of their own ability to work, including strengths and barriers. Employers are in central to provide opportunities for nurses to hold regular open discussions with their managers and raise concerns about issues that could affect their professional conduct negatively.
Footnotes
Acknowledgments
The authors would like to thank the contact persons of the participating organization for the collaboration in data collection and The Finnish Nursing Association and University of Turku for the support of the research.
Declaration of conflicting interests
The author(s) declare that there is no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Turun yliopiston tutkijakoulu. This study was received grants from The Finnish Nursing Association and University of Turku for the corresponding author.