
Abstract
Aim
This research examined the relationship between nursing managers’ power and nursing group power in public health service organizations.
Approach/Methods
A cross-sectional survey of first-line nurse managers (n = 264) from 11 Finnish hospitals was conducted. The power of nurse managers and nursing groups was examined through two reliable instruments: the Nursing Managers’ Power instrument and the Sieloff-King Assessment of Group Power within Organizations instrument©.
Findings
The power of nurse managers was perceived to be moderate on a 5-point Likert scale. Managers reported that they gained the most power from their role and position as a nursing manager, and lastly, from their resources. The power of nurse managers correlated no more than moderately with nursing group power.
Implications for Nursing Management
Organizations need to ensure that nursing managers have the power and opportunity to influence nursing goals and outcomes.
Introduction
In recent years, nursing managers have faced different challenges resulting from changes in health care organizations and service structure reform. One of these changes involves the changing role of first-line nursing managers (i.e., nurse managers and assistant nurse managers). For the first-line nurse manager, this means new and additional tasks, increased responsibilities and larger staff groups. 1 Competent professional nurses do not need to be managed. Rather, the health care environment needs to be managed so that nurses can better work with patients. 2 Thus, by managing the environment, the nurse managers exert influence on the achievement of the goals and outcomes of wards and nursing groups.3,4
During the last few years, researchers have studied nursing management from the point of view of hospitals’ Magnet factors and first-line nurse managers’ competency.5,6 First-line nurse managers need competencies, knowledge and skills in the essentials of power and influence to lead nursing groups to achieve their goals. 7 However, whether first-line nurse managers have the power to lead nurses, and the type of power they possess, has not been investigated.
In studies by Skytt 1 and Brown et al., 8 first-line nurse managers described the difficulties they face every day, such as staffing, nursing shortages and economics. These managers are responsible for issues such as the management of ward resources, recruitment, staff development, the guidance or support of staff, etc. 9 It is obvious that if first-line nurse managers are provided with additional support, resources and access to information, they could use the resulting power to more effectively influence ward, staff and patient outcomes. 10
Nursing group power, as a concept, has been minimally defined in public health care services in Finland, 11 although nursing power has been identified as an essential pre-requisite if a nursing group is to achieve its goals. Although traditional work environment factors have drawn the attention of nursing researchers, nursing group power (as a work environment factor) has received minimal attention. This study examined the relationship of first-line nurse managers’ power to the power of the nursing group.
Background
The concept of power
Power is a complex and broad concept with many diverse definitions and theoretical approaches drawn from organizational, psychological and social sciences. Several definitions of power have been identified in nursing. 12 Although power is often perceived as a negative concept, some nursing researchers 2 have viewed it as a positive resource available to every group within every health care organization.
Leadership, influence, authority and power are interrelated concepts. Power can be seen as a capacity to influence, while authority is the right to influence. In any case, power is an essential part of management, and is a characteristic of the social context and individual behaviour. 13 In this study, the concept of power is defined as a group’s capability to achieve its goals (Sieloff, personal communication, 27 November 2009), affecting the goals and outcomes of the health care organization.
Nurse managers’ power
Sieloff 3 defined nurse managers’ power as the knowledge and skills of a manager in relation to the achievement of nursing group goals. Several types of nurse manager power have been identified in the nursing literature: legitimate, expert, referent, 14 positional and personal.15,16 Based on these types, we examined nurse managers’ power in relation to their role, position and resources. First-line nurse managers were defined as nurse managers and assistant nurse managers, as these individuals work as the manager of units or wards.
Hersey et al. 16 stated that managers who understand and know how to use power in their role, are more effective than those who do not. Managers who feel they have the power in their role to implement change also report higher job satisfaction. 17 In addition, nurse managers who feel more efficacious in their nursing manager roles not only report more access to power for themselves but they also provide more access to power for their staff. 18
The literature shows that not all levels of nursing management have equal access to the same sources of power. The findings of Manojlovich 17 showed that the sources of power available to a nurse manager depended on the manager’s position in the organizational hierarchy. Positional power has been associated with nursing knowledge and management. Organizational cultures have clearly identified behaviours associated with nurse managers’ positions, delegated responsibilities and the authority to work independently. 16
Nursing group power
Sieloff 2 defined nursing group power as ‘the capacity of a group to achieve its goals’ (p. 54). This definition is based on Sieloff’s theory of the group power within organizations, that power is composed of eight components: controlling the effects of environmental forces, nursing position, nursing resources, nursing role, communication competency, goals/outcomes competency, manager’s power competency and power perspective. 3
Nurses expect that managers will provide them with resources to deliver patient care. Without these resources, nurses describe that they are unable to control their work environment. 22 However, literature has suggested that this provision of resources is not actually occurring, as nurses rated their levels of power in controlling the effects of environmental forces, nursing resources and their manager’s power competency as low. In contrast, nurses’ perceptions of the power perspective and goals/outcome competency were reported as moderate. 24 Nurses themselves perceive nursing group power as professional power that is related to the application of knowledge and skills to nursing practice, 23 and to achieving their professional role as patient advocates. 25 It is thus logical to propose that increasing work experience and knowledge would also increase power.
Groups who collaborate well with others are more likely to achieve their goals. 3 Doctor–nurse collaboration and communication have been found to contribute to positive results in patient care. 26 The nurses’ role as members of multi-professional groups also involves having a sufficient degree of power and autonomy. 27
The study
Aim and the research questions
The aim of this study was to answer the following research questions: 1) What is the level of power perceived by first-line nurse managers in public health care services? 2) What is the relationship between first-line nurse managers’ power and nursing group power in the public health care services?
The hypotheses designed to address the above research questions were: 1) Nurse managers’ overall levels of power are positively correlated with an individual nurse manager’s instrument scores. 2) Nurse managers’ power is positively correlated with nursing group power, as measured by the SKAGPO©.
Design
A cross-sectional descriptive correlation survey design was used. Information was obtained from first-line nurse managers in three specific divisions in eleven public health care hospitals in Finland.
Sample
In Finland, five university hospitals and 15 central hospitals provide public health care services. A convenience sample of 11 hospitals (population base approximately 200,000–250,000) was selected with divisions of surgical, medical and psychiatric care.
In calculating the differences between means, a power analysis identified a required sample size of 259 based on 90% power (p = 0.05) in order to detect a statistically significant 20% difference. At the time of conducting the research, there were 1,960 nurse managers and 1,390 assistant nurse managers working in Finnish hospitals. All first-line nurse managers in the three designated divisions of the selected hospitals were invited to participate in the survey. The nursing directors informed respondents about the study and data collection.
The first-line managers who responded to this study (n = 264) represented about 8% of the population. In addition to a bachelor degree in nursing, Finnish first-line nurse managers may have additional management education or university degrees.
Data collection
Data was collected from February to May 2010 using a questionnaire that consisted of three parts: 1) a background questionnaire, 2) the Nursing Managers’ Power instrument, 3) the Sieloff-King Assessment of Nursing Group Power within Organizations © (SKAGPO) instrument. The instruments were both pre-tested by a group of first-line managers (n = 27) to confirm the content validity and language clarity of the instruments in Finnish. Based on the outcomes, only linguistic revisions were required.
Background variables
The demographic data collected included: age, gender, length of work experiences in nursing (both as a nursing manager and in their present position), present title, and education level. The data collected on the organizations and divisions included: the type of organization, total number of health care staff in the organization, and the title of the first-line nurse manager’s supervisor, total number of wards managed by the first-line nurse manager and the nursing professionals on those wards.
In addition, managers were asked to assess their own overall level of power and responsibility as a first-line nurse manager using a Visual Analogue Scale of 0–10 (zero indicating the lowest and 10 the highest level). These were used as additional background variables.
Nurse Managers’ Power instrument
The Nurse Managers’ Power instrument included 31 items with three subscales: role 12 position 7 and resources. 12 Power was measured for each of the subscales by asking whether managers perceived that they had power, what made power possible for them, and also the source of that power. Items were measured on a 5-point Likert-scale (1 = Strongly agree to 5 = Strongly disagree). Consistent with the ranges associated with Sieloff’s instrument: 1–2.3 indicated a high level of power; 3.6–2.4 indicated a moderate level of power, and 3.7–5 indicated a low level of power. The internal consistency of the scale was measured by Cronbach’s alpha (overall α = 0.847; role subscale, α = 0.632; position subscale α = 0.599; resources subscale α = 0.697). These were at the satisfactory level, if a coefficient alpha of 0.70 is acceptable for new scales. The overall split-half reliability, tested by the Equal-Length Spearman- Brown Formula was 0.77.
Nursing Group Power Instrument
The Sieloff-King Assessment of Group Power within Organizations © (SKAGPO) is a 36-item questionnaire that estimates nursing group power and includes eight subscales: controlling the effects of environmental forces, 7 nursing position, 4 nursing role, 3 nursing resources, 6 communication competency, 3 goals/outcome competency, 4 group manager’s power, 4 and power perspective. 5 The items were measured, and cut-off (mean) scores indicated as above. The instrument has previously been psychometrically evaluated in three studies and its reliability and validity has been consistently demonstrated.27,28,29 In this study, for the Finnish version of the instrument, the internal consistency of the overall scale was 0.87 and the Cronbach’s alpha coefficients for the eight subscales were at satisfactory level ranged from 0.49 to 0.75. The overall split-half reliability (Spearman- Brown Formula) was 0.86.
Ethical considerations
Permission to conduct the study was obtained from each target organization, however further permissions from associated ethical committees were not required. Written permission to use the survey instrument was obtained from the authors. The participants were informed about the opportunity to participate in the study by their own supervisor by the cover letter. In that had been told about length of the instrument and possibility to interrupt their completion of the questionnaires without cause. No one took advantage of this option. Each respondent consented to participate in the study by completing the research questionnaires and questionnaires were completed anonymously. 25
Data analysis
The data was analysed using SPSS 18.0 statistical software (SPSS Inc., Chicago, IL). Descriptive statistics (mean, range, and standard deviation) were analysed for all variables and demographic data. The distribution of the variables and sum scores were analysed with tests of skewness and kurtosis. The mean scores for the subscales were derived by calculating the scores of the individual items and then dividing them by the number of items in the subscale. Differences between groups were examined using the independent samples t test and one-way analysis of variance (ANOVA). Pearson Product-moment correlations were used to analyse the relationship between the nurse managers’ and nursing group’s power. The relationship between the overall level of power and responsibility as a constant variable was analysed using Spearman’s Rank Correlation Coefficient. The level of statistical significance was set at p < 0.05 for all analyses. 31
Validity and reliability
The Nursing Managers’ Power instrument was developed for this study based on a literature review, the SKAGPO instrument and a qualitative study.14,15 Construct validity was statistically evaluated using item-total correlations. A pilot study was conducted with the first-line nurse managers in three different divisions in one health care organization. The reliability of the instrument was measured by its internal consistency (Cronbach’s alpha = 0.847; Split-Half = 0.77).The SKAGPO© was translated into Finnish using back translation. 25 A panel of eight experts (two charge nurses, two nurse managers, two experts in research related to organizational power and two experts in research methodology) assessed content validity. 26 They were chosen on the basis of their length of work experience, experience in the field of research, and their educational background. The construct validity of the translated instrument was statistically evaluated using item-total correlations. 27 The reliability of the translated SKAGPO© was comparable the basis of Cronbach’s alpha and item- total correlations to that determined in previous studies.28,29
Results
Description of participants
The study participants’ mean age was 49 years (SD = 6.94, range = 29–63). The majority of the participants were women 92% (n = 241). The mean length of nursing work experience was 24 years (SD = 7.97, range 5–40) and the mean length of managerial nursing work experience was 10 years (SD = 8.51, range = 1–32). Over half, 56% (n = 249), of the respondents had less than 10 years of experience as a nursing manager. The mean length of time in their current position was 8 years (SD = 7.36, range 1–30) (n = 237). However, of the 25 participants who had been in their current position for less than one year (mean of six months, SD = 3.2, range = 1–11), 85 % were nurse managers and 14 % assistant nurse managers.
Nursing managers’ power
First-line nursing managers’ (n = 264) perceptions of their own overall level of power and responsibility as reported by their scores on nursing managers’ power-instrument.
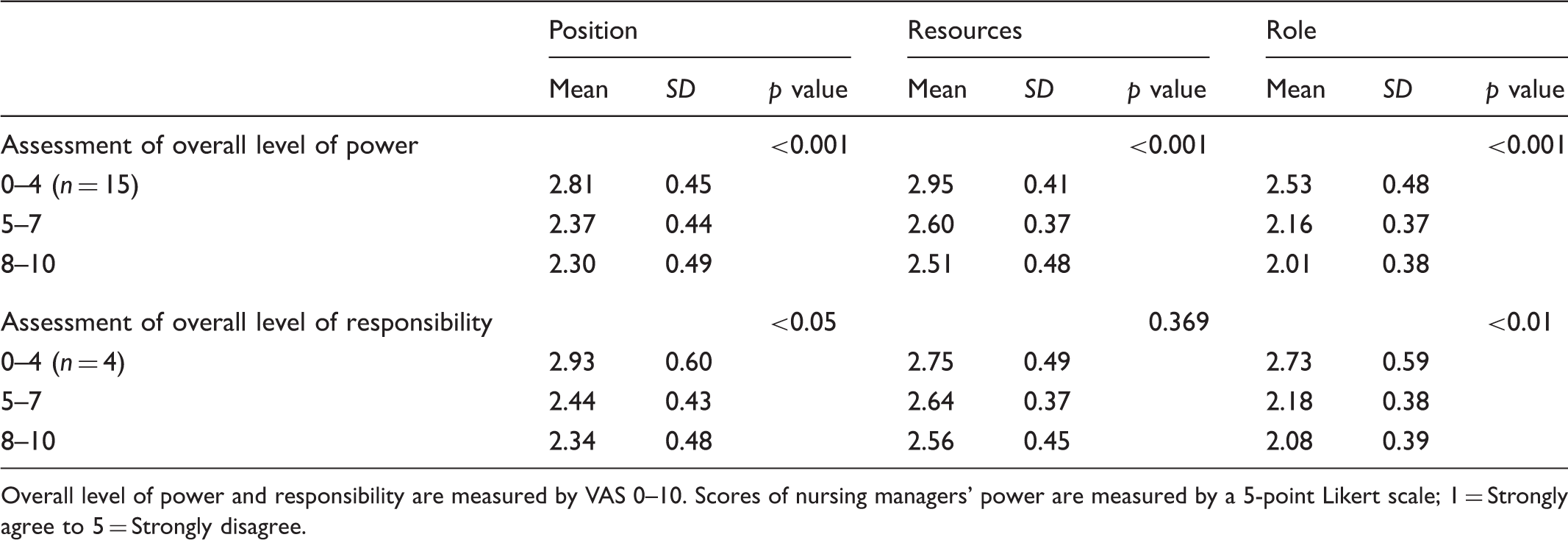
Overall level of power and responsibility are measured by VAS 0–10. Scores of nursing managers’ power are measured by a 5-point Likert scale; 1 = Strongly agree to 5 = Strongly disagree.
Relationship between sum scores of nursing manager’s power and assess of overall power and responsibility perceived by first-line nurse managers (n = 264).
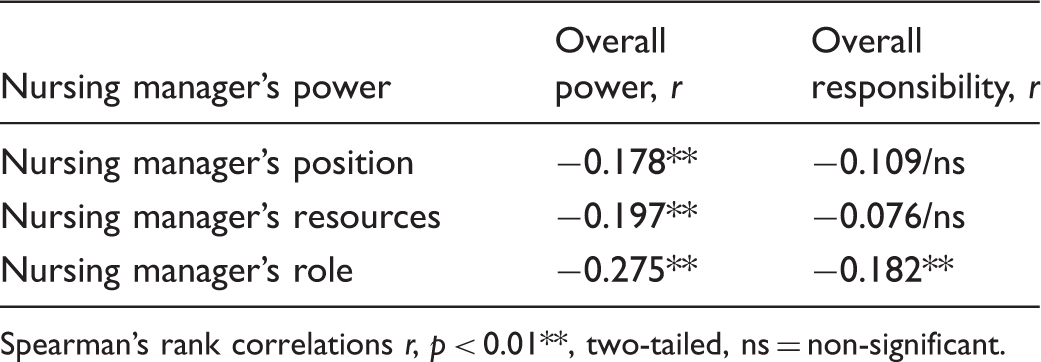
Spearman’s rank correlations r, p < 0.01**, two-tailed, ns = non-significant.
First-line nursing managers’ power as described by subscales
Respondents’ self-reported power was initially evaluated on a visual analogue scale from 0 to 10. This level of power correlated negatively, but weakly with the nurse managers’ position (r = −0.178, p < 0.01), resources (r = −0.197, p < 0.01), and with the nurse managers’ role (r = −0.275, p < 0.01). Most respondents (92%, n = 264) reported that they drew power from their position as a nurse manager, while an indication of personal power was only reported by 65% of the respondents.
More than a third of participants (36.9%, n = 97) reported that they did have enough financial resources to manage their ward, in contrast to 38.4% (n = 100) who perceived they did not. Similar results were reported in relation to human resources, with 42% (n = 112) of participants perceiving they had sufficient resources, while 43% (n = 113) did not. Over two-thirds (68%, n = 179) of the participants reported that sufficient informational resources were available for decision-making.
Nearly all of the respondents thought that their role as a nurse manager included staff development (93%, n = 245) for their ward. 98% (n = 258) believed that their role included responsibility for the performance of the ward. 87% (n = 228) perceived that they were responsible for the finances of the ward, and 97% (n = 256) perceived that they were responsible for monitoring the delivery of nursing care on the ward.
Participants reported that nursing management knowledge contributed more to their position of power on the ward, than power that was delegated to them (84%, n = 221). About two-thirds (65%, n = 170) of the respondents perceived that the power delegated to them was associated with the availability of resources, however 85% (n = 224) perceived that delegated power facilitated power associated with their role.
In relation to organizational contributions to power, 78% (n = 204) totally agreed or agreed that organizational hierarchy facilitated their position of power, while 74% (n = 193) reported it facilitated power associated with their role, and 57% (n = 149) of respondents totally agreed or agreed in terms of whether the organization’s hierarchy facilitated their power associated with resources.
The greatest differences were noted in participants’ responses regarding the factor that contributed most to their power. Nearly one-third (30%, n = 78) of the participants perceived that their position power was not effected by their supervisor. In contrast, 64% (n = 168) of the respondents reported that the power associated with resources was influenced by their supervisor.
In total, 92% of the respondents perceived that their power was associated with their position (n = 242), however 46% (n = 120) felt their role was not dependent on nurses. Similarly, 56% (n = 146) of the respondents also reported that their power associated with resources was not dependent on nurses. In contrast, 32% (n = 84) of the respondents perceived that their power associated with their position, role and resources, was dependent on their colleagues, while 25 % (n = 66) did not report which type of power was most dependent on their colleagues.
The relationship of a first-line nursing manager’s power to the power of nursing
Relationship between sum scores of Nursing Manager’s Power and the Sieloff-KingAssessment of Group Power within Organizations instrument (SKAGOAO©) perceived by first-line nurse managers (n = 264).
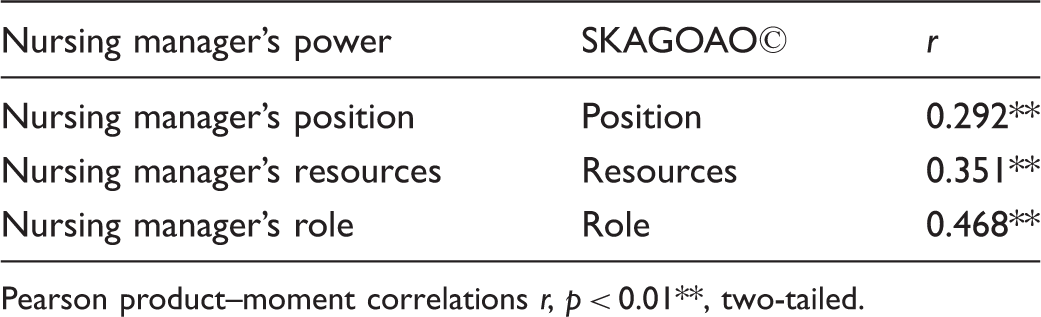
Pearson product–moment correlations r, p < 0.01**, two-tailed.
Discussion
Study limitations
Even if power is a general concept within organizational and social theory, there is a paucity of literature addressing the power of nurse managers or nursing. Therefore, it is difficult to compare the results of this study with previous research. In addition, it was the first time the Nursing Managers’ Power and SKAGPO instruments had been used in Finland, although the Nursing Managers’ Power instrument demonstrated reliability in this study and the SKAGPO instrument had previously demonstrated reliability and validity in the United States.12,29,30,32 Despite the translation issues related to SKAGPO, there may also have been different cultural interpretations of items by the respondents and this may have affected their responses. There may be differences in interpretation between the use of the SKAGPO© in different countries and when using different languages. Consequently, these differences may present some limitations to the generalizability of related findings. However, the generalizability of findings within the Finnish public health care system is possible as the sample was representative of ten of the twenty public hospitals in Finland.
Discussion of study results
The findings revealed that first-line nurse managers perceive the highest levels of power to be associated with their role, position and resources (respectively), on all three subscales at a moderate level. The respondents also perceived that their role as nurse manager was to be responsible for the ward’s daily operations, staffing and finance, and as a developers of nursing practice. This supports the earlier findings of Kleinman 9 and Jooste 7 However, the respondents did not unanimously support the idea that they should be nursing experts, so first-line nurse managers must further identify those nursing practices that need improvement and support their nurses to develop nursing practice.
The nurse managers’ role related power and the power of the nursing group (also associated with the role subscale), were moderately related to each other (r = 0.468, p < 0.01). This positive relationship is consistent with findings from previous studies, since a nurse manager’s role is to provide leadership in their ward and support nursing groups to achieve defined outcomes and goals3,4,12 When nurse managers perceive themselves to be powerful in relation to their role, this perception should also contribute to the nursing group’s view of the importance of their role within the organization.
According to the respondents’ perceptions of their power of position, they have power and legitimacy that occur specifically through the nursing context. 16 The results concerning the overall level of power and the first-line nursing managers’ power of position support this. However, the correlation between first-line nursing managers’ position and the nursing group’s position subscale was weak (r = 0.292). Both positional powers could be influenced by organizational culture factors not explained by this study, however, the respondents’ assessments of the power of first-line nursing managers’ position in the different divisions did not differ significantly.
Even if first-line nurse managers perceive that they have power associated with their position, the level of power seems to depend on the manager’s supervisor and colleagues, and depends less on the nursing group. In addition, respondents described the organization’s statutes as facilitating this positional power. This perception seems logical as the position of first-line nurse managers is defined by the organization’s policies, and these policies and guidelines also play a role in the nursing group’s power. 3 In contrast, previous research has found that the organization’s past and current statutes also could limit first-line nurse managers’ power 16 through the organization’s culture.
Over half of the first-line nurse managers experienced personal power. Personal power was previously described as the ability and opportunity to get things done in advance, and is also seen to influence cooperation and communication. 16 Upenieks 32 stated that personal power increases through the development of trust in relation to others. Therefore, personal power is an important resource and proposed to be linked to informal power.
In this study, the respondents perceived that they had low levels of resources to support the provision of care. This perception was consistent with that of the nursing group. At the same time, first-line nurse managers perceived that they are responsible for the budget of the ward’s nursing practice and the organization’s policies, governing the work of nurse managers, are thought to generally contribute to these perceptions.
Respondents also reported that they did not have sufficient information on which to base their decisions. These findings support those of Upenieks’, 32 where first-line nurse managers reported that they did not have sufficient knowledge to manage their budgets effectively. As a result, first-line nurse managers are often the least prepared to meet organizational challenges, even though they are expected to provide sufficient information to the staff. 4 Power related to knowledge has been identified in other studies as important,10,18 and having sufficient knowledge means being informed of the organization’s overall goals and actively participating in the organization’s decision-making processes. 33
Conclusion
When first-line nurse managers do not have sufficient power, they cannot effectively foster the development of nursing practice, or ensure that their units achieve their operational goals. The positive relationships between a manager’s perceived power and the power perceived by their nursing group should be viewed as important at unit and organizational levels, as these relationships could subsequently have a significant impact on the attainment of patient goals and outcomes related to safety and quality of care.
The results of this study suggest that nurse managers perceive that their power base lies with their supervisor and colleagues, rather than their own nursing group. In order for nurse managers to further increase their power and decrease their oppressed group behaviours, it is critical that they look to alliances within their nursing group rather than to external parties.
Due to changing health care environments, particular attention should be paid to the first-line nurse manager’s role, position and resources, in order to enable them to safeguard the operations of their unit or ward and ensure successful change management.
Footnotes
Author contributions
SV, PA and TS were responsible for the study conception and design; SV performed the data collection and data analysis; MH provided statistical expertise; SV were responsible for the drafting of the manuscript; CS, PA and TS made critical revisions to the paper for important intellectual content; PA and TS supervised the study.
Funding
Competitive Research Funding of the Central Finland Health Care District (B11208), Satakunta Hospital District 67/2011 (81021), Pirkanmaa Hospital District (9L099), (9N074), (R9048) and Finnish Cultural Foundation supported this study.
Conflict of interest
The authors declare that there is no conflict of interest.