
Abstract
Aim
Hypoglycemia due to hyperkalemia treatment using intravenous insulin is a serious complication that affects patients’ safety. This study aimed to (i) describe the incidence rate of hypoglycemia and associated risk factors in adult patients who received hyperkalemia treatment and (ii) report the parameters of patients who experienced hypoglycemic episodes with corrected hyperkalemia and those without.
Methods
This prospective descriptive study included hospitalized patients between November 2020 and July 2022 who received intravenous insulin to treat acute hyperkalemia with serum potassium exceeding 5.0 to 5.5 mEq/L. Blood glucose monitoring was conducted 1, 2, 4, and 6 hours after treatment.
Results
Among 300 patients reviewed, the hypoglycemia rate was 19.7%; 78.6% of the hypoglycemic events occurred within the first 2 hours; 12.9% and 8.6% occurred at 4- and 6-hours post-treatment, respectively. One significant association with increased risk for hypoglycemia was a history of kidney-related conditions, including chronic kidney disease and undergoing hemodialysis or peritoneal dialysis. Among those who received the hyperkalemia treatment, 44.4% (n = 133) had persistent uncorrected serum potassium readings, and 21.6% (n = 29) experienced hypoglycemia episodes.
Conclusions
Hypoglycemia is a common complication associated with the use of intravenous insulin for hyperkalemia management in hospitalized patients, with a noted higher incidence in those with kidney-related conditions. Early monitoring within the first 2 hours after treatment is critical, as most hypoglycemic events occur during this period. Intensive blood glucose monitoring and standardized treatment protocols based on patient risk factors, such as renal history, are essential to enhance patient safety and minimize hypoglycemia.
Introduction
Acute hyperkalemia with serum potassium ≥5.5 mEq/L is a common complication experienced by patients in the acute care setting. 1 If immediate treatment is not administered, it may result in cardiac arrhythmias, and patients may experience severe muscle weakness or even paralysis. 2 Treatment of hyperkalemia using intravenous insulin is commonly administered to lower the serum potassium rapidly; however, it may result in risk, including hypoglycemia.3–5
Hypoglycemia is usually defined as a glucose concentration in the blood lower than 4.0 mmol/L. 3 The clinical manifestations of hypoglycemia are often progressive, and early signs often go undetected, with patients experiencing mild symptoms, including sweating, palpitations, tremors, and hunger, to severe complications, including arrhythmias and impaired cognitive function.6,7 Severe hypoglycemic episodes have also been associated with higher mortality, with an odds ratio of 1.66, and prolonged hospitalization. 6 Previous studies identified hypoglycemia incidences between 8.7% and 17.5%.6,8–10 A recent comprehensive scoping review reported a prevalence as high as 17.2%. 11
Background
Hypoglycemia following hyperkalemia treatment can be influenced by the variations of intravenous insulin and dextrose dose and the methods of administration.3,4,12 However, findings in the previous studies and reviews reflected inconclusive results of the impact of these variations on the hypoglycemia events. One of the studies highlighted that higher intravenous insulin or lower intravenous dextrose dosages were associated with an increased risk of developing hypoglycemic episodes; however, no recommended dosages for intravenous or intravenous dextrose were provided. 3 The effect of continuous infusion of intravenous insulin and intravenous dextrose administered over three hours was investigated, with the study reporting overall low incidences of hypoglycemia and severe hypoglycemia at 6.1% and 1.2%, respectively. 4 Conversely, the scoping review by Chothia et al. found no differences in the prevalence of hypoglycemia when comparing insulin doses, the rate of insulin administration, or the timing of insulin administration relative to dextrose. 11
Acute hyperkalemia requires immediate treatment with intravenous insulin and dextrose. However, the optimal correction rate for serum potassium is not established, and the importance of immediately lowering serum potassium in patients without the manifestations of hypoglycemia is uncertain. Previous study findings concluded that the decrease in serum potassium after insulin treatment has no significant differences between patients who developed hypoglycemia and those who did not.4,13 The association of hypoglycemia with pre-and post-treatment serum potassium levels is not well-explored. 14
Adequate monitoring of blood glucose levels can enable quick detection of the changes to the blood glucose levels following intravenous insulin and dextrose administration. Nonetheless, blood glucose monitoring post-hyperkalemia treatment guidelines are not standardized in the acute care.8,14–16 There is also no consensus on the ideal and safest approach to administering insulin for patients who experience hyperkalemia. It is critical to have a structured system to determine the risk and analyze the outcomes. Iatrogenic hypoglycemia is a critical patient safety event with serious complications that must be managed with appropriate blood glucose monitoring.
The study
Objective
This study aimed to describe the demographics of adult patients receiving hyperkalemia treatment in the inpatient wards of our institution and report the current practice of the blood glucose regimen about the outcomes of the patients, including the incidence rate of hypoglycemia and the associated risk factors. In addition, a comparison of the parameters (including the treatment regimen) between patients who experienced hypoglycemic episodes with corrected post-hyperkalemia reading and those who did not with uncorrected hyperkalemia reading was conducted.
Study design
A prospective descriptive design was adopted.
Participants and setting
Convenience sampling was used to recruit all adult patients hospitalized in the inpatient wards in one of the largest academic hospitals in Singapore between November 2020 and July 2022 who received intravenous insulin to treat hyperkalemia.
The inclusion criteria of reviewed patients were patients who experienced acute hyperkalemia with serum potassium exceeding 5.0 to 5.5 mEq/L.14,17 According to the European Resuscitation Council, hyperkalemia is further categorized into mild (5.5-5.9 mmol/l), moderate (6.0-6.4 mmol/l) or severe (≥6.5 mmol/l). Patients were excluded if they received continuous intravenous insulin or intravenous insulin for other medical conditions and not for the treatment of hyperkalemia or had potassium results concluded by laboratory staff to be haemolyzed. Patients with hemolyzed potassium results could have artificially elevated potassium levels, which can lead to misleading conclusions regarding the severity of hyperkalemia and its correlation with hypoglycemia risk during insulin treatment. 18 During the study monitoring period, there was no standardized insulin treatment regimen, but prescribed based on the team physician’s medical decision made from assessing the patient’s condition.
Data collection
Blood glucose monitoring protocol
In the current institution, there was no standardization on the specified follow-up time for checking blood glucose after insulin administration for patients with hyperkalemia. A standardized blood glucose monitoring protocol was then developed utilizing the best evidence from current hyperkalemia clinical guidelines.11,19–21 This protocol included monitoring capillary blood glucose at scheduled timing, including the first, second, fourth, and sixth hours after insulin with dextrose treatment. A previous study by Chothia et al. has suggested that most hypoglycemic events occur within the first few hours after insulin treatment. 11 By monitoring the first and second hours after treatment, the protocol ensures early detection of hypoglycemia when it is most likely to occur. In addition, monitoring at the fourth and sixth hours allows for continued surveillance as insulin’s effects may extend beyond the initial hours, particularly in patients with impaired renal function. Insulin clearance can be delayed in individuals with renal disease, which increases the risk of prolonged insulin action and subsequent hypoglycemia. 22 These time intervals allow detecting any delayed hypoglycemic episodes that may arise due to prolonged insulin activity or other factors like rebound hypoglycemia. This structured blood glucose monitoring protocol was implemented simultaneously in six inpatient wards (two surgical and four medical inpatient wards) for over a year.
The nurses in the participating wards were briefed on the structured blood glucose monitoring protocol. The nurses initiated blood glucose monitoring post-insulin with dextrose treatment as follows: first, second, fourth, and sixth hours after insulin with dextrose treatment. Patients who developed hypoglycemia were treated according to the institution’s hypoglycemia protocol workflow.
The demographic and clinical data collected included age, sex, race, body mass index, medical history (including diabetes and kidney disease including chronic kidney disease, undergoing hemodialysis or peritoneal dialysis), and concomitant use of medications that influence the blood glucose readings were documented from the electronic medical records. Commonly identified medicines that affect blood glucose levels in the literature were oral anti-diabetic medications, insulin, salbutamol inhalers, and corticosteroids. 3
The hyperkalemia treatment regimens prescribed, including intravenous insulin, intravenous dextrose, and intravenous calcium gluconate, were documented. These are the first-line hyperkalemia treatments used in this acute care institution. Pre- and post-treatment serum potassium levels were recorded. The blood glucose monitoring readings taken at the first, second, fourth, and sixth hours after the hyperkalemia treatment were assessed using the point-of-care blood glucose meter. The blood glucose meter is commonly used in the acute care setting, which provides a quick and accurate measurement of glucose levels at the patients’ bedside. 23 The quality control testing of the blood glucose meters used in the inpatient wards followed the institution’s guidelines to ensure the accuracy and reliability of the meters.
The incidence of hypoglycemia was measured at 1, 2, 4, and 6 hours after the insulin with dextrose treatment as the primary outcome in this study. Hypoglycemia was defined as a blood glucose of <4.0 mmol/L and severe hypoglycemia was defined as a blood glucose level of <2.8 mmol/L. 3
Data analysis
Data was entered into and analyzed using SPSS version 25.0 (IBM Corp, Armonk, NY). Descriptive statistics were used to report demographic and clinical data and the frequency of patients with hypoglycemia at 1, 2, 4, and 6 hours after hyperkalemia treatment. t test and chi-square or Fisher’s Exact test were used to compare the parameters between patients who experienced hypoglycemia events post-hyperkalemia treatment and those who did not. A comparison of parameters between patients who experienced hypoglycemia events with corrected post-hyperkalemia readings and those with uncorrected hyperkalemia readings was also conducted. Univariate analyses of the association between demographic and clinical variables and hypoglycemia outcomes were conducted using logistic regression. Given the operational constraints and the availability of patients who fit the inclusion criteria over a set time period, a formal sample size calculation was not carried out. Instead, a recruitment strategy based on the screening period was implemented in this study. A p-value of less than 0.05 was deemed statistically significant. For patients who experienced more than one hypoglycemia event, only the first event was analyzed for reporting demographic results.
Ethical considerations
This study was approved by the Central Institutional Review Board. The implementation of the blood glucose monitoring protocol was explained to the participants by the inpatient ward nurses, and verbal consent was taken to record their demographic and clinical data.
Results
Overall patient demographic and clinical characteristics
Overall patient demographics and clinical data and comparison of parameters between patients who experienced hypoglycemia events post hyperkalaemia treatment and those who did not (n = 300).

Note: BG = blood glucose; BMI = body mass index; K = Potassium; IV = Intravenous.
ddenotes multiple responses in each patient.
eIncludes patients with either Chronic Kidney Disease non dialysis, Hemodialysis or Peritoneal dialysis, denotes multiple responses.
fOnly included if medications were taken on the day of hyperkalaemia treatment.
bOnly the first hypoglycaemia event of each patient was included.
cIndependent two-sample t test.
aHyperkalaemia is defined as a potassium serum level of ≥5.5 mmol/L (The European Resuscitation Council).
Incidence of hypoglycemia
Blood glucose monitoring during the 1, 2, 4, 6 hours after receiving intravenous insulin, among patients with corrected and uncorrected post-hyperkalemia treatment serum potassium (n = 300).

Note: *Of the 70 hypoglycaemic events, 12 patients had ≥2 hypoglycaemic events consecutively during monitoring.
Patients with corrected serum potassium levels (4.5 to 4.8 mmol/L) reported 4.4% (blood glucose range 1.7–3.8 mmol/L), 4.4% (blood glucose range 2.2–3.9 mmol/L), 1.6% (blood glucose range 2.0-3.9 mmol/L), and 1.3% (blood glucose range 3.1–3.6 mmol/L) hypoglycemic events occurring at 1 hour, 2 hours, 4 hours, and 6 hours post-treatment. Patients with uncorrected serum potassium levels (5.2 to 5.7 mmol/L) reported lower rates of hypoglycemic events, with 3.4%, 5.0%, 1.3%, and 0.7% of events occurring at 1-, 2-, 4-, and 6-hours post-treatment, respectively.
Among all the 300 patients who had received hyperkalemia treatment, 59 (19.7%) patients experienced hypoglycemia (Table 1). The mean age of the group was 69 (SD14.1), with 61% male. A total of 50.0% of these patients had diabetes, and 64.4% had kidney diseases. Most of these patients received 10 units of intravenous insulin, 40 mL 50% intravenous dextrose, and 10 mL intravenous calcium carbonate 10% (74.6%). The mean pre- and post-treatment serum potassium readings were 5.9 mmol/L (SD 0.6) and 5.1 mmol/L (SD 0.7).
Patients who experienced hypoglycemic episodes with corrected and uncorrected post-hyperkalemia treatment serum potassium
Comparison of parameters between patients who experienced hypoglycemia events with corrected and uncorrected post-hyperkalemia treatment serum potassium (n = 300).

Note: BG = blood glucose; BMI = body mass index; K = Potassium; IV = Intravenous.
bdenotes multiple responses in each patient.
cIncludes patients with either CKD non dialysis, Hemodialysis or Peritoneal dialysis.
aOnly the first hypoglycaemia event of each patient was included.
dOnly included if medications were taken on the day of hyperkalaemia treatment.
Among the patients who received the hyperkalemia treatment with and without hypoglycemic episodes, 133 (44.4%) had persistent uncorrected serum potassium readings. Among these patients, 29 (21.6%) experienced hypoglycemia episodes and reported a mean age of 70 (13.8). A total of 51.7% were male, with 55.2% having diabetes and 37.9% having kidney diseases. Most patients were administered 10 units of intravenous insulin and 40 mL of 50% intravenous dextrose (58.6%). Among the patients who received hyperkalemia treatment, with and without hypoglycemic episodes, 167 (55.6%) had corrected serum potassium readings. Of these, 30 (18.0%) experienced hypoglycemic episodes, with a mean age of 69 (SD 14.2). A total of 60.0% were male, with 43.3% having diabetes and 66.7% having kidney diseases. Most patients were administered 10 units of intravenous insulin and 40 mL of 50% intravenous dextrose (90.0%).
Association of patient demographic and clinical characteristics with the occurrence of hypoglycemia event
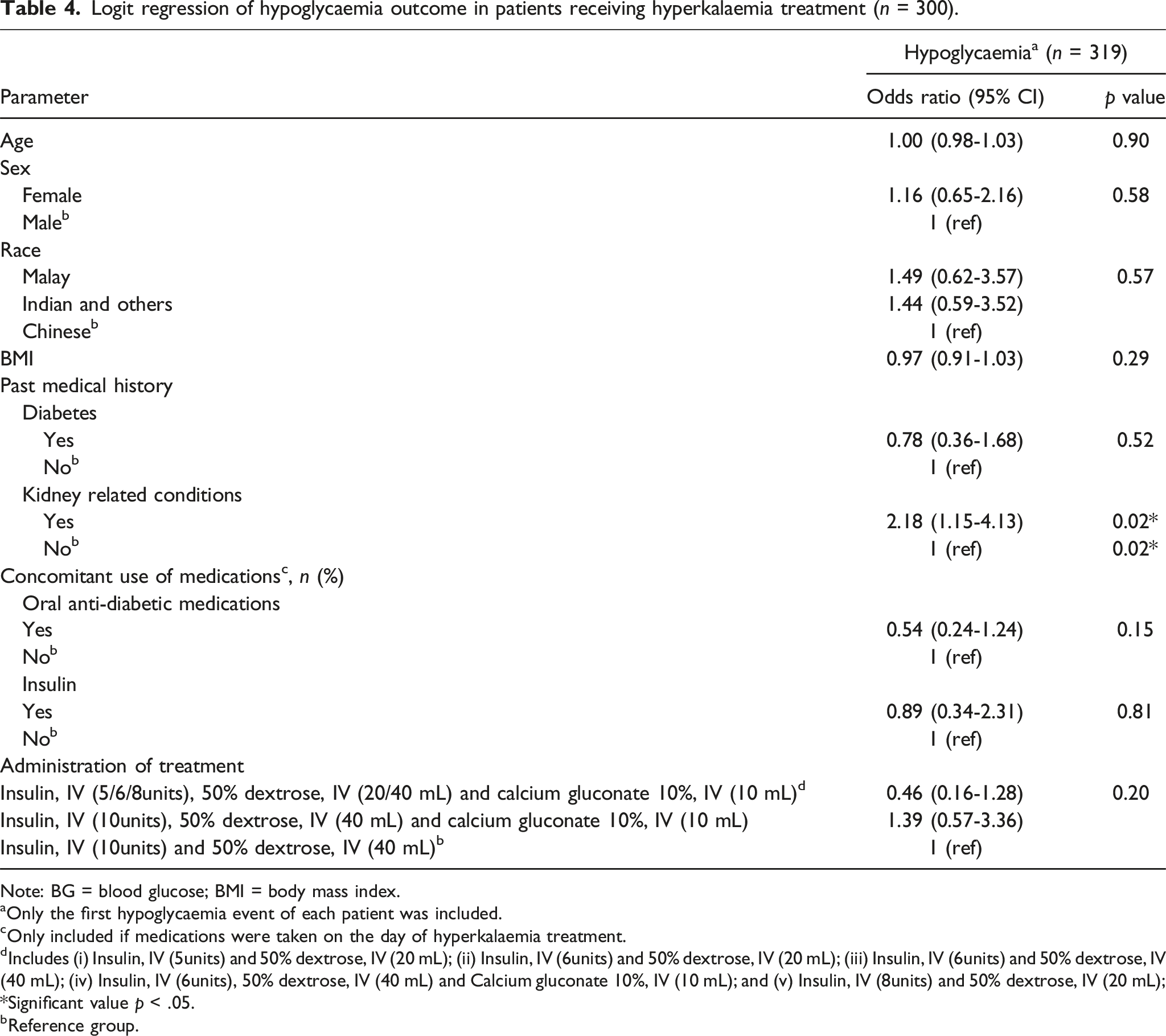
Logit regression of hypoglycaemia outcome in patients receiving hyperkalaemia treatment (n = 300).
Note: BG = blood glucose; BMI = body mass index.
aOnly the first hypoglycaemia event of each patient was included.
cOnly included if medications were taken on the day of hyperkalaemia treatment.
dIncludes (i) Insulin, IV (5units) and 50% dextrose, IV (20 mL); (ii) Insulin, IV (6units) and 50% dextrose, IV (20 mL); (iii) Insulin, IV (6units) and 50% dextrose, IV (40 mL); (iv) Insulin, IV (6units), 50% dextrose, IV (40 mL) and Calcium gluconate 10%, IV (10 mL); and (v) Insulin, IV (8units) and 50% dextrose, IV (20 mL); *Significant value p < .05.
bReference group.
Discussion
Hypoglycemia is a clinically relevant and widely recognized adverse event associated with the administration of insulin in the acute care setting. Treatment of hyperkalemia with insulin may lead to significant iatrogenic hypoglycemia. Our study implemented a structured blood glucose monitoring protocol developed based on updated clinical guidelines and evaluated the incidence and risk factors of hypoglycemia in patients treated for hyperkalemia with intravenous insulin in the general wards.
Although the patients in our study were older, consistent with literature suggesting that individuals over 60 are at a higher risk of hypoglycemia, age did not emerge as a significant risk factor.10,12,24 This may be due to several factors, including the influence of treatment protocols and comorbidities, which warrants further investigation. 25 Older age is often considered a risk factor for hypoglycemia due to factors such as deteriorating renal function affecting drug clearance, increased adverse drug interactions from polypharmacy, and reduced cognitive functioning, which may impair the ability to detect or respond to hypoglycemic episodes. 26 This study found a significantly increased risk of hypoglycemia with an odds ratio of 2.18 in patients with kidney diseases, which is consistent with existing literature.10,27 Renal insufficiency impairs insulin clearance, leading to prolonged insulin action and increases the risk of hypoglycemia in patients with kidney disease. 22 Patient-specific factors, such as the history of kidney disease, may be useful for predicting blood glucose fluctuations during the treatment of hyperkalemia. This will be beneficial for developing future standardized treatment order sets with an integrated decision tool that can advise appropriate prescriptions of different insulin and dextrose dosages based on the patient’s risk factors.
Published studies report a wide range of hypoglycemia rates (8.7% to 19.7%) associated with inpatient insulin use for hyperkalemia treatment.4,13,15,28,29 Our study found an incidence of 18.5%, consistent with these reported rates. The relatively high incidence of hypoglycemia in this study highlighted the importance of adequate blood glucose monitoring. Frequent monitoring is a key preventive strategy for rebound hypoglycemia as a result of insulin administration.30–33 Although the recommended monitoring protocol remains unspecified in the literature, our study implemented a structured protocol with glucose measurements at scheduled times: first, second, fourth, and sixth hours post-treatment.19–21,34 We found that 78.6% of hypoglycemic events occurred within the first 2 hours, with 12.9% and 8.6% occurring at 4 and 6 hours, respectively. Previous studies have shown hypoglycemia episodes occurring between one to six hours post-insulin administration.12,13,27,30,32,33 Additionally, this study revealed that the peak timing of hypoglycemia was 2 hours after starting insulin therapy, aligning with Chothia et al.'s findings, which reported a median timing of 124 minutes. 11
Among the patients who received the hyperkalemia treatment, 44.4% had persistent uncorrected serum potassium readings. Among these patients, 21.6% had hypoglycemia episodes. Hypoglycemia can occur despite uncorrected potassium levels because of the timing mismatch between insulin’s effects on glucose and potassium, delayed insulin clearance, insufficient glucose supplementation, or excessive insulin administration.25,35 While correcting potassium is critical for managing hyperkalemia, proper management of blood glucose through intensive monitoring of patients with repeated intravenous insulin administration is important to prevent hypoglycemia.
Limitations
This study had its limitations. Firstly, we could not control potential confounding factors that may influence the results, one of which was the pre-admission administration of medications that affect blood glucose levels, which may be temporarily suspended by the team physician due to the patient’s medical condition and were not included in the analysis. It remains unclear to what extent patients may have taken these medications before admission, which can increase the risk of hypoglycemia. The lack of a standardized insulin regimen during the study’s duration introduced a potential source of variability, which could impact the reliability of our findings. Future studies could benefit from subgroup analyses based on the insulin regimen used, allowing for more granular insights into how different treatment protocols influence hypoglycemia risk.
We could not determine the association between patients’ nutritional status during hospitalization and the risk of hypoglycemia post-hyperkalemia treatment. The patients who received the hyperkalemia treatment in the current study were found to be older. It is common for older patients to experience loss of appetite in the hospital setting. Malnutrition can still occur even when patients’ diet is not restricted.
Another limitation is the potential for information bias, as the accuracy of hypoglycemia identification relied on consistent documentation of blood glucose levels and symptoms. Any inconsistencies in these records could impact the reliability of the results. Additionally, the use of convenience sampling may have introduced selection bias, as patients included in the study may not represent the broader population. Future studies could employ a more rigorous sampling method to ensure a more representative and diverse sample, thereby enhancing the external validity of the findings. Furthermore, our study was conducted at a single institution, which may limit the generalizability of the results to other settings. A larger, multicenter study would provide a broader sample and greater external validity, enabling more robust conclusions to be drawn about the incidence and risk factors for hypoglycemia in patients treated for hyperkalemia.
Implications for practice
Given the significant incidence of hypoglycemia in patients treated for hyperkalemia with insulin, healthcare providers should adopt structured blood glucose monitoring protocols. This study found that regular glucose measurements at scheduled intervals (first, second, fourth, and sixth hours post-treatment) were essential for identifying hypoglycemia events early. Instituting a similar monitoring protocol could reduce the risk of undetected hypoglycemia and help guide timely intervention. In addition, monitoring timeframes for hypoglycemia can be reevaluated. This study found that 78.6% of hypoglycemic events occurred within the first 2 hours of insulin administration, and the peak timing was 2 hours. This suggests clinicians should prioritize early glucose monitoring within the first 2 hours after insulin administration. Additional monitoring could be necessary at later time points (e.g., 4-6 hours), depending on the patient’s risk profile. Monitoring for patients with persistent hyperkalemia should also be prioritized. Since 44.4% of patients in this study had persistent uncorrected serum potassium levels, those patients would require more intensive monitoring for hypoglycemia, especially after repeated doses of insulin and dextrose.
Standardized order sets with a decision tool can be developed and integrated within the electronic health records to improve the consistency and safety of insulin and dextrose administration during hyperkalemia treatment. These order sets would include clear and predefined protocols for insulin dosing, dextrose supplementation, and blood glucose monitoring times. The order sets should be tailored to the patient’s risk profile, such as prior history of renal disease, and specify the necessary actions depending on the patient’s condition, such as the frequency of glucose monitoring and insulin or dextrose administration adjustments. This helps ensure that each patient receives appropriate care based on their needs. Clinicians could factor in risk factors such as renal function when prescribing insulin and adjust dosages accordingly, possibly using lower doses or more frequent monitoring to mitigate the risk of hypoglycemia. The integrated decision tool can automatically populate patient-specific factors and recommend the appropriate insulin and dextrose doses with tailored glucose monitoring schedules. Real-time alerts can also be integrated for clinicians, particularly in high-risk cases so that the system can issue a prompt to increase monitoring frequency or adjust the insulin dosage. Alerts could also be set for when a patient with persistent hyperkalemia receives multiple insulin doses, ensuring clinicians are more aware of the cumulative risk of hypoglycemia in these cases.
Education for healthcare professionals is key to improving awareness of the potential for hypoglycemia, especially in high-risk patients such as those with renal insufficiency. 36 Ensuring awareness of rebound hypoglycemia can help prevent such episodes and improve patient safety.
Conclusion
Hypoglycemia is a significant and common complication associated with the use of intravenous insulin for hyperkalemia management in hospitalized patients, with a noted higher incidence in those with kidney-related conditions. Early monitoring within the first 2 hours after treatment is critical, as most hypoglycemic events occur during this period. Intensive blood glucose monitoring and standardized treatment protocols based on patient risk factors, such as renal history, are essential to enhance patient safety and minimize hypoglycemia. Further research is needed to refine these protocols and assess their effectiveness across diverse patient populations and clinical settings.
Footnotes
Acknowledgments
We would like to thank all the nurses in the inpatient wards who had been involved in the implementation of the revised blood glucose monitoring regimen used for this study. We would also like to acknowledge Ms Tan Kai Hui and Ms Stephanie Shuk Tyng Chong for their expert advice in the study design process.
Author contributions
Five authors contributed to the completion of this manuscript. Lim Siew Hoon: Conceptualisation, Methodology, Data collection and review, Writing-original draft preparation, reviewing and editing. Ang Shin Yuh and Fazila Aloweni: Conceptualisation, Methodology, Writing-Reviewing and Editing. Teh Ming Ming: Conceptualisation, Methodology, Writing-Reviewing. Siti Namira Binte Abdul Wahab: Data collection and data review. All authors have agreed on the final version and meet at least one of the following criteria (recommended by the ICMJE*):
1) substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data;
2) drafting the article or revising it critically for important intellectual content.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.