
Abstract
Large variations in palliative care education across and within countries are reported. Nursing students report that they feel unprepared for palliative care. The present study identified and outlined whether universities integrated learning outcomes on palliative care as described in the national regulation into programme descriptions and course plans after implementation of the National Curriculum Regulations for Norwegian Health and Welfare Education (RETHOS) in the 2020 academic year. A qualitative descriptive design with a document analysis approach was used. The findings revealed variation in the terminology used. Palliative care was differently emphasized in selected learning outcome descriptors, related subjects, and presence in the academic trajectory. It is crucial to emphasize palliative care in nursing education to prepare the future workforce to meet patients’ and their families’ individual needs in a multidisciplinary environment across service levels.
Introduction
Today's health service is constantly evolving and offers increasingly advanced diagnosis, treatment, and follow-up to the public. More people survive and live longer with their advanced diseases. As a result, we have an aging population with a high incidence of heart failure, chronic respiratory diseases and cancer and an increase in comorbidity with need for palliative care. 1 The palliative approach includes optimizing quality of life (QoL) and relieving pain and troublesome symptoms in people with severe diseases regardless of diagnosis and age. 2 As many as 70–80% of all patients need palliative care in their last years or months of life. 3 This care should be tailored to the patients’ and their families’ individual needs, often in a multidisciplinary environment across service levels.2,4,5
People who provide palliative care must be equipped with the necessary knowledge, skills and competence to do so. 4 However, palliative care education is repeatedly identified as a challenge, where lack of training is seen as a barrier to ensuring palliative care for all, and to development of the discipline.6–9 In the field of nursing, students globally report that they feel unprepared for palliative care upon clinical placement.10–12
Back in 2004, The European Association for Palliative Care (EAPC) published a consensus-based guide for the development of nursing education programmes across Europe. 13 The guide proposed a general framework of knowledge acquisition divided into level A (basic), level B (advanced), and level C (specialist). The structure of the levels and the number of hours associated with the educational preparation were left for each country to decide. Nearly two decades later, large variations in palliative care education across and within European countries are reported.1,14 This is particularly reported related to inclusion of palliative care in nursing undergraduate curricula. 14 Palliative care teaching in nursing education is commonly included as a module in another subject and is only taught as a specific mandatory subject in France, Austria and Poland. Few countries offer clinical placements in a specific palliative care unit, and there are still countries that do not offer any palliative care teaching in nursing education at all. 1 A study on nursing education in Sweden, 15 describes that it is up to each university to decide whether to include a compulsory course about palliative care in their undergraduate nursing programmes. Only a few did. Lecturers had to compete with other topics and strived to increase the content of palliative care education. Similar findings are reported from other parts of the world, as well as in other healthcare disciplines.16–18
Although the complexity in palliative care is increasingly recognized within national health policy frameworks, there is a lack of policy guidance on the provision of training to meet this healthcare challenge. 6 In the 2020 academic year, Norway adopted the National Curriculum Regulations for Norwegian Health and Welfare Education (RETHOS, henceforth referred to as the national regulation), which includes palliative care. The purpose of the national regulation is to ensure a nationally equal academic level to produce graduate candidates with a common final competence, independent of the educational institution. 19 Nursing education in Norway is a three-year bachelor's degree programme and consists of 50% integrated clinical placement. The programme is based on the Bologna declaration that generated a consensus to focus on evidence-based education at the bachelor’s, master’s, and PhD levels. 20 The expected final competence is described in the form of learning outcomes for completed candidates. 20 Learning outcomes are defined as ‘statements of what a learner knows, understands and is able to do upon completion of a learning process that is defined in terms of knowledge, skills and competence also described as learning outcome descriptors’. 20 (p.C111/4)
The national regulation presents learning outcomes on palliative care in Chapter 2 ‘Health, disease, and nursing’, which is one of five competence areas. It is described as follows under the learning descriptors of knowledge §4 b: ‘the candidate has broad knowledge of the nurse's health-promoting, preventive, therapeutic, rehabilitative and caring function, including knowledge of palliative care’. The learning descriptors of skills do not include palliative care as a learning outcome, but competence §6a describes that ‘the candidate can plan and carry out nursing care for the acutely and critically ill, chronically ill and people with comorbidity and complex needs in the primary and specialist health services. Furthermore, the candidate must be able to provide nursing care for people in the palliative phase’. The national regulation stresses that the candidate must be able to provide nursing care for people in the palliative phase in primary care and specialist health services. The structure of the education must ensure coherence, progression, and integration between theory and practice in a manner that supports the learning outcome descriptions. 19
The wording ‘nurse's caring function’ is translated from the Norwegian term ‘sykepleierens lindrende funksjon’. Caring is at the core of the nursing profession, which aims to alleviate suffering, protect patient dignity and promote health. 21 The caring function and palliative care are sometimes used synonymously in the Norwegian language. 22 However, the national regulation emphasises palliative care explicitly and this is perceived as an important focus related to nursing care.
Although documents are governing tools, the directives in these documents are not automatically realised as intended. When nursing education institutions in Norway implemented the national regulation, each local education programme developed programme descriptions and course plans that provided an outline for the bachelor's level. Universities have some flexibility in the design of their educational programmes, but the national goals must be met. 23
Based on the literature review, there seems to be variation internationally in the implementation of palliative care into educational programmes. Thus, we find it of interest to explore how a country that has recently implemented policy guidelines that emphasise palliative care, integrates this subject into nursing education.
Study aim and research question
The aim of the study was to identify and outline whether learning outcomes for palliative care were integrated into programme descriptions and course plans in nursing education in Norway as described in the national regulation.
The following research question was addressed: What are described as learning outcomes for palliative care in programme descriptions and course plans in Norwegian bachelor's nursing programmes?
Methods
Document analysis
A qualitative descriptive design with a document analysis approach was used.24,25 Document analysis, as a qualitative research method, is a systematic procedure for reviewing and evaluating documents to gain understanding and empirical knowledge. 26 The method may be used in a variety of ways, including to track change and development. Excerpts, quotations, and entire passages are used to yield data by organizing these items into major themes, categories, and case examples specifically using qualitative content analysis. 26
Summative qualitative content analysis
Documents in the present study were analysed using a summative qualitative content analysis approach inspired by Hsieh and Shannon. 27 This method allows counting and comparisons and was used to identify and outline whether learning outcomes for palliative care were integrated into programme descriptions and course plans. Public nursing education in Norway was selected from university websites and reviewed for inclusion during Autumn 2021. Nine of 11 universities were included. Table 1 lists the inclusion and exclusion criteria.
Inclusion and exclusion criteria.

The selected universities are presented as University A, B, C, etc. through to the letter I. When extracting information from the selected sources, we used a deductive content analysis approach described by Elo and Kyngäs. 28 The national regulation was used as the data source to define the categories when comparing the selected programme descriptions and course plans. The analysis process had three main phases: preparation, organizing, and reporting. 28
Preparation phase
The selected university programme descriptions and course plans were reviewed to identify and select units of analysis. A unit may be a word, theme, sentence, or portions of pages. 24 The chosen units of analysis in the present study were programme descriptions and course plans describing learning outcomes for palliative care. Because palliative care may be described using different words, we included associated words, such as end-of-life care, death, terminal care, symptom relief, and caring nursing. Table 2 provides the entire list.
Words or phrases used to describe learning outcomes on palliative care in programme descriptions and course plans.

Organizing phase
To make sense of the data as a whole, we developed a structured categorisation matrix, 28 in which the identified categories were based on recommendations in the national regulation. Categories one, two, and three are presented in Table 3. The table describes whether palliative care was included verbatim or modified in programme descriptions and course plans and explicit words that were used. Modified indicates that minor changes were made to the wording of the learning outcome. Table 4 provides an overview of categories four, five, and six. Category four presents the academic year in which palliative care was presented. Category five describes the subjects. The subjects were divided into the following subcategories: basic nursing, acute and critical care, comorbidity/homecare, pathology, or teamwork. The matrix indicates whether the subject was theoretical or clinical. The categories reflect the national regulation requirement to include palliative care in primary care and specialist health services, and the structure of the education programme must ensure coherence, progression and integration between theory and practice in a manner that supports the learning outcome descriptions. 19 The national regulation describes palliative care under the learning outcome descriptors of knowledge and competence. Therefore, the learning outcome descriptors used by universities are presented in category six.
Categorization matrix for categories 1–3; the selected universities’ implementation of learning outcomes for palliative care in the programme and course plans, and the explicit words used.

Note. LO: learning outcomes; PC: palliative care.
Categorization matrix for categories 4–6; academic year, subject and learning outcomes descriptors where palliative care is described at the selected universities.
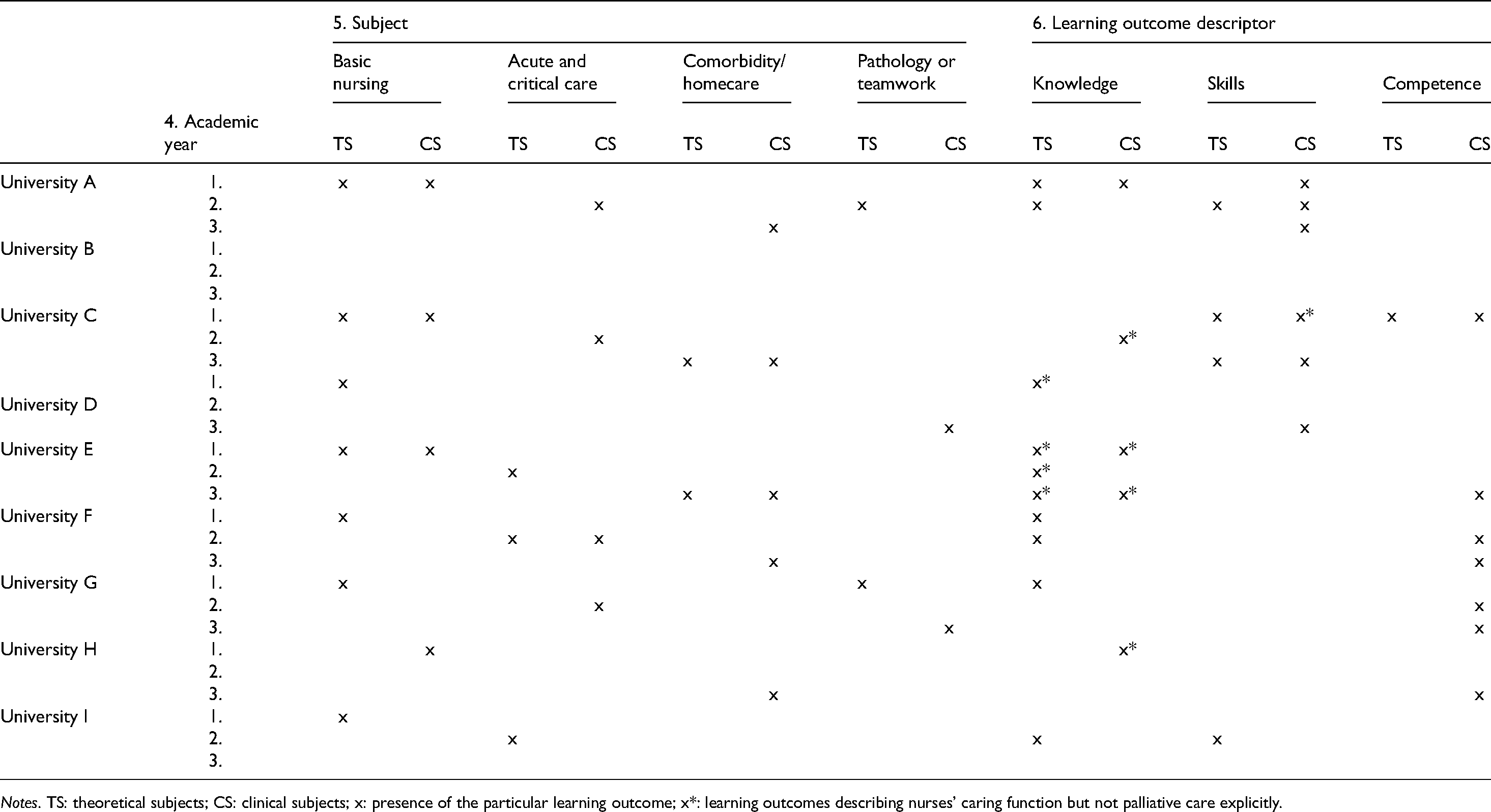
Notes. TS: theoretical subjects; CS: clinical subjects; x: presence of the particular learning outcome; x*: learning outcomes describing nurses’ caring function but not palliative care explicitly.
After creation of the structured categorization matrix, the first author reviewed the units of analysis several times and coded for correspondence with the identified categories. The entire team discussed the findings. The reporting phase is presented in the Findings and Discussion sections.
Ethical considerations
Ethical approval was not required for this work because the data were retrieved from open websites. The universities are not identifiable.
Findings
Inclusion of palliative care or associated words in programme descriptions and course plans
Table 3 provides an overview of categories one, two and three based on recommendations in the national regulation and the codes from the document analysis. Universities presenting a programme description online, including palliative care or words associated with the term as learning outcomes, were available in three of nine universities: A, G, and H. When describing learning outcomes for palliative care in course plans, modified text was common. Only universities F and G used the description from the national regulation verbatim. When analysing the data for explicit words used to describe palliative care, several words associated with the term emerged, including end-of-life care, death, terminal phase, symptom relief, and caring nursing. Table 2 provides an overview of explicit words and phrases used and how often the different terms emerged in the units of analysis. The analysis revealed that different course plans within the same university used different terms to describe palliative care. The number varied from one, as in universities F and G, to eight in University A. Several universities described ‘that the candidate has broad knowledge of the nurse's health-promoting, preventive, therapeutic, rehabilitative and caring function’ but excluded knowledge of palliative care.
Academic year, subject and learning outcomes descriptors where palliative care is described
When analysing whether learning outcomes for palliative care were represented in academic years 1, 2, or 3, we found that the term was represented throughout the three years in most of the education programmes (Table 4). However, there were exceptions. Universities D and H did not include palliative care in year 2, and University I did not include it in year 3. Learning outcomes for palliative care were not included in any year in University B. Notably, some of the included learning outcomes used the term ‘nurses’ caring function’ or ‘symptom relief’ without associating these terms with palliative care, and whether the learning outcome was related to palliative care or the nurses’ caring function in general was not clear. These issues are marked with a star in Table 4.
Basic nursing was the course plan where all universities, except University B, included learning outcomes for palliative care, several universities included this in both theoretical and clinical subjects. Other categories exhibited greater variation. Most universities included learning outcomes for palliative care in theoretical and clinical subjects, but there were exceptions, such as University H, which only included the term in clinical subjects.
Universities C, E, and I included relatives and the needs of the bereaved associated with palliative care. None of the universities included palliative care in course plans describing mental health or paediatrics.
The national regulation describes learning outcomes for palliative care under the learning outcome descriptions of knowledge and competence. Analysis of the course plans revealed that the learning outcomes description of knowledge was used by six of the nine universities in theoretical subjects, and in four of the nine universities in clinical subjects. The learning outcomes descriptor ‘skills’ was used in theoretical subjects by Universities A, C, and I, and Universities A, C, and D included skills in clinical subjects. Competence as a learning outcome descriptor was only used by University C in theoretical subjects, but it was included in Universities C, E, F, G, and H in clinical subjects.
Discussion
These findings demonstrated variation in the integration of palliative care into programme descriptions and course plans. Palliative care was emphasized differently across learning outcome descriptors, related subjects, and academic years. The following discussion centres on the terminology used and the universities’ integration of learning outcomes for palliative care.
The use of terminology
Palliative care and associated words were revealed in our analyses of the programme descriptions and course plans. Although the associated words described in Table 2 are part of palliative care, we perceived these words as inadequate because the palliative care approach includes more than care for the dying.2,4,5 Zaman et al. 29 drew attention to the distinction between ‘palliative care’ and ‘end-of-life care’. End-of-life care refers to care for a patient with a terminal condition, while palliative care is recommended from the time of diagnosis to the end of life for all life-limiting illnesses. In Norway the term palliative care was not included in national regulations regarding nursing education until 2020. The focus was to ‘relieve suffering and help the patient to a dignified death’. 30 Palliative care may be an unknown word to students, and the words used by universities are perhaps easier to understand. However, a systematic review by Hui et al. 31 stressed that the exact meanings of ‘end of life’ and ‘terminal care’ were not clear. Their findings revealed a paucity of references conceptualizing or defining the terms. Thus, modification of the descriptions used in the national regulation increases the possibility of changing the content and intention. Therefore, it is unfortunate that different words and phrases are used to describe learning outcomes for palliative care between and within universities. We recognized that University B did not include palliative care or associated words and that Universities D, E, and H only included palliative care explicitly as a specific topic in one of their course plans. The absence of the term might indicate that the learning outcomes were general and hidden as a topic. Palliative care may appear in syllabi, lectures, or tasks, but the findings in this study suggest that the topic is omitted. Other studies indicate that palliative care often is included as part of other subjects,1,15,16 and that end-of-life care is the topic most emphasized. 32
However, the national regulation explicitly uses the term palliative care when describing ‘the candidate has a broad knowledge of the nurse's health-promoting … and caring function, including knowledge of palliative care’, and similarly under competence. Palliative care includes more than a nurse's caring function. Caring is the core of the nursing care process 21 and includes the knowledge, skills, and competence that nurses need when caring for all people. As several universities include the nurse's caring function but exclude using the term palliative care in their learning outcomes, our interpretation was that the national regulation was not followed.
What happens in the transformation from legal text to programme descriptions and course plans when palliative care is modified extensively, and other words are used in learning outcomes? We argue that there is a risk of the universities losing their opportunity to ensure a nationally equal academic level and graduate candidates who have a common final competence in palliative care, independent of the educational institution.
Integration of learning outcomes on palliative care
The national regulation uses knowledge and competence as the learning outcome descriptors when describing palliative care. The candidate must be able to provide nursing care for people in the palliative phase in primary care and specialist health services. The present study found that universities did not systematically follow the national regulation. Our organization of the data into the structured categorization matrix (Tables 3 and 4) identified variations in the integration of the topic of palliative care and the academic year. These results reveal a shortcoming in the implementation of the national regulation and recommendations describing palliative care tailored to the patients’ and their families’ individual needs in a multidisciplinary environment across service levels.2,5,7 Lack of integration of palliative care into nursing education, as described in this and several other studies,15,16,33 is considered as a barrier, across country borders, to enhancing palliative care for all people.1,9 According to the national regulation, the structure of education must ensure coherence and progression. As shown in Table 4, learning outcomes for palliative care were represented in academic years 1, 2, or 3 in five of the nine universities. However, with the exclusion of the course plans with general wording which clouded whether the outcome was related to palliative care or the nurses’ caring function in general (marked with * in Table 4), only Universities A, F, and G met the recommendation. Smeby and Heggen 32 revealed that programme coherence had a significant impact on theoretical knowledge and practical skills. Because of the complexity of palliative care and the call for increased emphasis on palliative care in nursing education,1,9 the presentation of palliative care throughout all three years is beneficial.
The integration of theory and practice in a manner that supports the learning outcome descriptions is emphasized in the national regulation. Some universities, such as A and E, had course plans that integrated the two learning environments. However, palliative care was commonly added to course plans that described either theory or practice. Palliative learning outcomes were linked to theory in 14 course plans and clinical placement in 15 courses. Arias-Casais et al. 1 and Jeong et al. 34 describe that a theoretical approach is most common as a teaching method when teaching palliative care. In addition there are few opportunities for nursing students to learn palliative care in the clinical setting, particularly in specialist palliative care placements. 35 This finding is supported by Valen et al., where the nursing students experienced that healthcare personnel acted as gatekeepers for entering palliative care situations and thereby affected the students’ learning outcomes. 36 Thus, there is a risk that these issues will affect the students’ progression in the field, especially since palliative care skills and competence development is a continuous process, and knowledge and skills become internalized and manifest while practising. 32 The learning outcome descriptor skills was used in connection with palliative care by Universities A, C, D, and I, but not in the national regulation. We argue that palliative care requires nursing skills that may be developed through nursing education. 37 The systematic review and meta-analysis by Donne et al. 12 revealed that palliative care education improves health professional students’ knowledge about and attitudes towards palliative care, but more research is required to draw conclusions about the students’ skills development. We therefore call for national regulations and course plans that include both knowledge, skills, and competence in palliative care.
Although a gap was identified in palliative care health services between the guidelines and practices for the needs of relatives and the bereaved,38,39 we found it surprising and insufficient that only three of the nine universities included relatives in learning outcomes associated with palliative care. When searching for units of analysis 28 containing palliative care or associated words in the selected course plans, we found no connection to mental health or paediatrics. Palliative care is supposed to be provided for all life-limiting illnesses and for people of all ages including patients’ relatives. 2 The EAPC atlas on palliative care in Europe 2019 draws attention to the fact that only 16/51 countries included palliative care in paediatric nurses’ curricula. The health workforce’s capacity to provide care to neonates, children and adolescents including support for their families, needs to be strengthened, and education is seen as a key to such competence development.1,7 Another concern in our study is that the number of credits in the included course plans varied from three to 20. The national regulation gives no directions for the credits required to meet the learning outcome in palliative care, nor do other directives.6,13 Variation in the number of teaching hours and clinical practice within and among countries will likely affect the degree of palliative care. The university course plans often included learning outcomes for acute and critically ill patients, which leaves the impression that nurses’ health-promoting, preventive, and therapeutic functions are more important. Pressure on time is reported as a barrier to include palliative care.16,18 One question is whether the universities present learning outcomes consistent with strategic plans. Another is whether it depends on enthusiasts in palliative care to ensure that this topic is emphasized. Findings by Hagelin et al. 15 and White et al. 18 indicate that ‘champions’ advocating for palliative care often are the case, and an advantage.
The national regulation in Norway was implemented in the 2020 academic year and was new for the universities when they developed the selected programme descriptions and course plans. This novelty may have influenced the emphasises of learning outcomes for palliative care. However, many countries do not include palliative care as a compulsory course, and the subject is normally a module within other subjects. 1 There are gaps regarding teaching time content, assessment and teaching staff dedicated to palliative care.14–18 We are concerned whether these factors limit the ability of education programmes to convey the complexity of palliative care.
Hagelin et al.’s 15 study finds that lecturers experienced that the most challenging aspects for students were to provide an understanding of the palliative care approach, promote good communication skills and identify the patients’ existential concerns.
We emphasize that palliative care must be taught explicitly. Only then can the learning outcomes in the final competence description be achieved and documented. By providing explicit description of palliative care in the course plans and curricula, nursing faculties have the unique opportunity to improve care for patients with palliative care needs and their families.
Today, palliative care education is highlighted in political plans, guidelines, and research.2,19 The present findings suggest that there is still work to be done before universities anchor palliative care in programme descriptions and strategy plans to ensure that their graduates have a common final competence in palliative care, independent of the educational institution. We recommend development of national programme to prepare the future workforce with the necessary knowledge, skills and competence to provide palliative care, such as the Palliative Care Curriculum for Undergraduates programme in Australia that has been well established since 2003, 4 or the End-of-Life Nursing Education Consortium (ELNEC) developed by the American Association of Colleagues of Nursing. 9 National programmes should be in line with international educational goals, such as the Bologna process in Europe, as competence levels from A to C can create confusion compared to recommended learning outcome descriptions and education levels from bachelor’s to PhD level. 40
Strengths, limitations, and trustworthiness
Document analysis is efficient because the data of many documents are available online without the authors’ permission. Therefore, document analysis is cost-effective. 26 However, one limitation is that documents are sometimes hard to retrieve. Two of the 11 Norwegian universities were excluded from our study based on the lack of online access. An incomplete selection of documents may lead to ‘biased selectivity’. 26 Another advantage is that documents are stable, exact, cover many events, settings, or a long time span, and are unaffected by the data collection process. However, documents often include insufficient details to answer a research question because they are produced for other reasons. 26 To ensure trustworthiness in the present study, the authors worked systematically to achieve confirmability in all of the steps throughout the study. Credibility or confidence in the truth of the data 28 is emphasized by the inclusion of most Norwegian universities offering nursing education. All programme descriptions and course plans were reviewed to identify suitable units of analysis that described learning outcomes for palliative care. We worked systematically to cover all data and organized the data into a categorization matrix 28 based on recommendations in the national regulation. The first author coded the text and developed the categorization matrix, and the other authors assessed the adequacy of the analyses and commented on possible complements. The findings may be biased because private institutions offering nursing education were excluded. These universities are affiliated with religious foundations in Norway, which may affect the emphasis on palliative care.
To increase credibility reliability, the analysis process was described in detail. Tables 2, 3, and 4 provide connections between the data and the findings.
Throughout the analysis and discussion, we worked on our objectivity to ensure confirmability. The first and last authors are particularly aware that their background as teachers in palliative care may have influenced their interpretations. Because different words are used to describe palliative care in Norwegian and English, some of the content of the description may have changed in the translation. The selected universities present their programme descriptions and course plans differently, which made these factors difficult to compare. Some universities had a list of different subjects that described the content of the course plans. Although palliative care was mentioned in several subject lists, these lists were not included because the aim of the document analysis was to identify and outline learning outcome descriptions. If we had included the lists, compulsory reading, and teaching schedules, a different impression of how the universities emphasize palliative care may have been found. Trustworthiness includes the question of transferability, which refers to ‘the extent to which the findings can be transferred to other settings or groups’. 41 However, it is the reader's decision whether or not the findings can be transferable to their own context. To facilitate transferability, Graneheim and Lundman 41 suggested giving a clear description of culture and context, selection and characteristics of participants, data collection and the process of analysis and documentation. Thus, we have given a vigorous presentation of the findings that can serve as background for reflection to other contexts and settings, and thereby enhance transferability.
Further research
The findings in this document analysis only provide information from the universities’ programme descriptions and course plans. Research on how learning outcomes on palliative care are integrated into compulsory reading and teaching schedules is recommended. Investigating whether nursing students attain learning outcomes in palliative care requires other research strategies. It would also be of interest to identify and outline how learning outcomes in topics other than palliative care are described in the national regulation and integrated into programme descriptions and course plans from universities in Norway. In Europe, where we have the consensus on descriptions of learning outcomes corresponding to the three education levels (bachelor’s, master’s and PhD), comparisons between countries in the northern and southern parts might be interesting to emphasize since the healthcare service structure and family responsibility varies geographically. From such perspectives, research may give rich knowledge on dealing with palliative care in different settings within Europe. Internationally, comparing curricula from countries where palliative care is highlighted in white papers and explicitly documented in nursing course plans and curricula, might shed light on different approaches to enhance palliative care competence.
Conclusion
This document analysis from the Norwegian nursing education demonstrated that palliative care, as described in the national regulation, was not systematically integrated into the selected universities’ programme descriptions and course plans. A variation was revealed in the terminology used, and palliative care was emphasized differently in selected learning outcome descriptors, related subjects, and academic years.
Explicit use of the term palliative care should be included regarding learning outcomes in knowledge, skills, and competence, in both theoretical and clinical subjects. Coherence and progression throughout the learning trajectory must be emphasized to prepare the future workforce with the necessary palliative care competence to meet the patients’ and their families’ individual needs in a multidisciplinary environment across service levels. To ensure that graduated candidates have a common final competence in palliative care independent of the educational institution, national regulations and educational programmes explicitly addressing palliative care are recommended.
Footnotes
Author contributions
Study design: KV and EKG. Data collection: KV. Data analyses and discussion: KV, ALH, KTJ and EKG. All authors approved the final manuscript.
Data availability statement
The analysed documents were obtained from publicly accessible sources from the selected university websites.
Ethics approval
Ethical approval was not required for this work because the data were retrieved from open websites. The universities are not identifiable.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
The authors declared receipt of the following financial support for the research, authorship, and/or publication of this article: Our respective institutions funded the work on the article based on the authors’ research times.