
Abstract
Healthy development of infants/toddlers is associated with adequate parent–child interactions, infant sleep patterns, and infant nutrition. In early childhood, learning to fall and stay asleep is essential and can contribute to infants’ self-regulation and to regulating emotions and behavior. Sleep problems in infancy are, however, of significant concern to parents. This study aimed to research the benefit of a face-to-face family education and support intervention concerning ‘Better sleep better well-being’ (FES-BSBW). Six advanced community healthcare nurses provided three sessions of FES-BSBW intervention to the parents. Data were assessed from 35 primary caregivers. The TREND and TIDieR guidelines were used to report findings. The intervention focused on parent–child interactions and normal child development, temperament, parents’ beliefs about the infants’ sleep patterns, and the impact of the infants’ sleep problems on the parents’ quality of life after the intervention. The intervention was delivered over approximately one month. The primary findings showed that mothers reported significantly higher perceived family support, improved sleep pattern beliefs, better physical functioning and longer infants sleep periods on average at nights after the FES-BSBW intervention. These findings are promising and might prevent sleep problems in infants/toddlers from escalating later into more severe health problems.
Keywords
Introduction
Sleep problems among infants involve frequent night waking, inadequate sleep duration, shorter sleep time than age-appropriate duration, sleep loss, and settling difficulties.1–3 Furthermore, sleep problems depend on whether the parents define their infants’ sleep as problematic; however, frequent waking up at nights with crying beyond the age of six months is commonly viewed by parents as a problem. 2 Therefore, sleep problems in infancy and toddlerhood can have negative effects on parents’ well-being and the quality of parent–child interactions1,4 and can contribute to parental distress. 5 Moreover, parents’ concerns about their young child’s problem with sleep have been found to be the major reason for seeking assistance from healthcare providers in the community, such as well-childcare clinics.1,6,7
According to Sadeh and colleagues, 5 between 20 and 30% of infants and toddlers have sleep problems in the first three years of life. Sleep problems in infancy and toddlerhood are associated with children's daytime behavioral issues, parental fatigue, and negative parent–child interactions;1,5 however, the frequency of these problems varies based on the cultural context of the research. In an international study of 29,287 parents of infants and toddlers aged 0–3 years from 17 countries, 52% of the parents from predominantly Asian countries identified sleep problems in their children, and 17% of them reported severe sleep problems. Contrastingly, only 26% of the parents from predominantly Caucasian countries reported that their children had sleep problems, with 2% reporting severe sleep problems. 5 Thus, the authors concluded that cultural variables must be considered when determining parental perceptions of infant sleep problems.
Notably, brief clinical interventions for both healthcare professionals1,6 and families of young children with sleep problems are effective. In a study by Hall and Nethery, 1 23 public health nurses attended and evaluated a training workshop to address gaps in knowledge and enhance interventions to manage infants’ behavioral sleep problems. Furthermore, in the same study, 15 parents attended a pilot sleep workshop, and seven of them indicated their preference for a follow-up intervention involving a telephone support interview. Moreover, Stuttard et al. 8 conducted a pilot study on behavioral sleep problems in young children with neurodisability, where a telephone call intervention for sleep management (eight families) was compared with regular home visits (seven families). The findings indicated that the telephone calls appeared to be acceptable and convenient to deliver sleep support and were positively valued by both parents and healthcare practitioners.
However, interestingly, in a narrative review by Field, 9 where 62 studies with various designs were included, the studies confirmed that parents had explored several educational/behavioral interventions to manage infant sleep problems. Further, some of these studies show improvements and others suggest only short-term or small effects. Moreover, Kempler et al. 10 conducted a systematic review and meta-analysis of randomized controlled trials (RCTs) on psychological sleep interventions, with nine studies in the review. The primary outcome indicated improvement in reported infant total sleep time, but there was no evidence for reducing infant night wakes; there was evidence, however, of maternal mood improvements. Thus, psychosocial sleep interventions appear to impact the amount of sleep that mothers report their infants to have, although they frequently wake up. 10 More research is required to confirm whether sleep-related improvements can be translated into improvements in maternal mood.
Similarly, Matthey and Črnčec 11 compared the effectiveness of two treatment strategies for infant sleep problems on maternal mood and infant sleep and emotional health. The two treatment strategies were systematically ignoring with a minimal check, and a new but similar method where parents pretended to sleep in the infant's room before intervening (parental presence with minimal check). The Australian families of 16 infants aged 6–18 months with sleep difficulties were randomly assigned to one of the two conditions. Measurements were taken at baseline and again at three weeks and four months post intervention. Both treatments were effective, with a third to a half of the families reporting decreased infant sleep problems at three weeks post intervention, and nearly all reporting reduced infant sleep problems at follow-up. Likewise, most mothers in both treatments reported improvements in their experiences or mood, and there were no discernable adverse effects on infants’ emotional health. These findings support previous research on the effectiveness of systematic ignoring interventions with minimal checks, commonly known as controlled crying. Interestingly, the study also supported parental presence with minimal check, which was found to be as effective as controlled crying. 11
Specific behavioral interventions targeting severe sleep problems in young children have been developed and tested;2,12 however, little is known about the benefits of advanced nurse-led interventions in the community for families of infants with moderate sleep problems. The family education and support intervention ‘Better sleep better well-being’ (FES-BSBW) was developed and evaluated to assist families in the community to manage infants’ moderate sleep problems, 6 aiming to prevent sleep problems in infancy from developing further into disorders. The FES-BSBW program is based on family systems theory and the Calgary family nursing conceptual framework. The family unit is defined as a group of two or more individuals working together as an interconnected network. They are linked to each other through solid emotional ties and the feeling of belonging, having a genuine interest in one another, and being involved in each other's lives.13–15 The FES-BSBW intervention 16 addresses normal child development, 17 temperament, 18 sleep rhythm, 19 and parent–child interactions. 20
To encounter parents’ requirements for evidence-based material and support them effectively in managing their young child's sleep problems, community health care (CHC) nurses are required to provide education on the etiology of sleep problems to parents and support those who have infants with sleep troubles. 16 Nurses are also required to have an innovative understanding of family nursing21–24 to tailor interventions for sleep problems to parents/families.
Based on the above literature review and the Calgary conceptual framework,13–15 it was hypothesized that parents of infants with moderate sleep problems who received two face-to-face sessions and one telephone call session according to the FES-BSBW intervention would report significantly higher perceived family support, higher sleep pattern beliefs, and higher quality of life, after the intervention compared to baseline. Further, to gain a deeper understanding of the nature of sleep problems among infants, we asked the following specific research questions regarding the parents’ perception of the patterns of their infants’ sleep problems after the intervention compared to before. That is: Is there a significant difference before and after the FES-BSBW intervention in: a) the infant's most extended sleep period at night and; b) the number of the infant's nap periods during the day?
Methods
Data collection took place in 2017. The intervention was offered by advanced practiced nurses (APNs) at six CHC centers in the capital area of Reykjavik, Iceland. Participants answered a set of questionnaires via REDCap (Research Electronic Data Capture software), both pre and post intervention. Families that were concerned about their infants’ sleep and contacted their CHC center for advice or services regarding infant moderate sleep problems were referred to a research assistant, who introduced the study to the parents. After having signed the consent form, the parents received an email with a code for the REDCap program to answer the set of questionnaires and a sleep diary to take home and describe their infants’ sleep patterns. The diaries’ contents were described in our earlier publication regarding the development of the intervention. 6 The parents were asked to bring the diaries back to the first interview at the CHC center. The parents answered the same set of questionnaires again after completing the FES-BSBW intervention.
Data collection and sample
The inclusion criteria for participating in the study were that the parents were required to raise their worries, concerns, and difficulties in handling their infant sleep problems at home with their community healthcare nurse. The parents also felt they required specific support and information to address this moderate sleep problem in their infants. Therefore, the FES-BSBW method was developed to help parents handle their infants’/toddlers’ sleep problems. Further, the parents were required to be able to read and write Icelandic. The exclusion criteria were that the infant/toddler had health problems (e.g. ear infections) or that the parents were unable to read or write Icelandic.
A total of 114 parents (61 mothers and 53 fathers) were introduced to the study after the parents had raised their concerns and difficulties in handling their infant's sleep problems with their community healthcare nurse at the well-child-care unit. Of them, 101 (52 mothers and 49 fathers) provided informed consent and completed the set of questionnaires at baseline. After the second face-to-face (and final) session of the FES-BSBW intervention, 35 mothers and 24 fathers (59 parents) completed the intervention and answered the questionnaire again, resulting in a participation rate of 67.3%. The reason for not completing the intervention, which the parents provided, was that their infants/toddlers had a health problem that was resolved in collaboration with their physician at the community healthcare center (e.g. ear infection), or that they did not have the time to participate (mainly the fathers had work responsibilities). Therefore, in this study, data were analyzed from 35 mothers at CHC centers. Furthermore, the data from the parental dyads (n = 24) will be published in a separate manuscript. The TREND 25 and the TIDieR 26 guidelines which are guidelines developed to report quasi-experimental and intervention research, were used to report the findings in the manuscript.
The advanced CHC nurses who offered the FES-BSBW intervention
The intervention, which involved two face-to-face sessions and a telephone call, was delivered by six advanced CHC nurses trained in the FES-BSBW program through 32 hours of lectures on infant sleep problems as well as individual consultations and a group case report consultation (lasting about 2 hours per family) by an advanced expert nurse in infant sleep problems. 6 Two face-to-face sessions of the intervention were delivered at CHC centers. The APN, who specialized in infant sleep problems, secured the study fidelity by going over the intervention manual in detail with the CHC nurses and by offering them 32 hours of lectures and knowledge about infant sleep problems and individual consultations and group case report consultations. 6 However, even though study fidelity was ensured, the intervention was tailored to each family's requirements. More detailed information about the development of the intervention's manual and content, including its relation to the theoretical foundation that the intervention was based on and how the intervention was offered, is presented in a separate manuscript. 6 The intention to provide the intervention is described in detail below.
Before the first session of the FES-BSBW intervention, about one week earlier, the parents completed a set of questionnaires at home and then received the first face-to-face session of the intervention at the CHC center lasting 60–70 minutes for each family. One week later, the advanced CHC nurses offered the families the telephone call session of the intervention, which lasted for about 20–25 minutes for each family. About one week after the phone session, the CHC nurse offered the family the third and last session of the FES-BSBW intervention, namely the second face-to-face session at the CHC center lasting 60–70 minutes. About one week after the previous session, the families answered the questionnaires again (post intervention). The intervention lasted approximately 4–5 weeks.
The FES-BSBW intervention
The FES-BSBW program was initially developed at the Children's Hospital at the University Hospital in Iceland.15–20,27–31 The program was adjusted and revised to fit families of young children with moderate sleep problems at CHC centers. 7 The FES-BSBW intervention program is based on the Calgary family models 15 and the Family Strength Oriented Therapeutic Conversation intervention. 32 The FES-BSBW intervention includes two main components: the child's behavioral component and the parent–child interactional component. The aim of the FES-BSBW program was to educate families on typical child development, 17 temperament, 18 sleep rhythm, 16 parent–child relationship 20 as well as empowerment, motivation, and behavioral and environmental issues 16 (i.e. behavioral component). Additionally, the program trained the parents to use their knowledge regarding infant sleep problems in various interactional situations (i.e. parent–child interactional component) 16 (see the content of the FES-BSBW intervention in Box 1).
The content of the first, second and third sessions of the FES-BSBW intervention.
In the first session, the advanced CHC nurse met the families at the CHC center and went over the sleep patterns described in their infants’ sleep diaries. The mothers took the sleep diary with them to the first session, so the advanced CHC nurse could check it and discuss the infant's sleep patterns with the parents. The nurse then asked the parents to share their experiences of the infant's sleep difficulties and habits and the family's daily life. The nurse then informed the parents about what could disturb the infant's sleep patterns and how sleep difficulties in infancy could be handled. Subsequently, the parents and nurses discussed what intervention would best fit the family. They considered, for instance, the timing of sleep and waking periods, infant and parent intimacy (both father and mother). Further, they considered the infant's self-soothing capability at daytime and nighttime, the parents’ reaction during night awakening, and nursing interventions based on the infant's age and how they could be applied. The psychology of sleep, normal arousal, nutrition, sleep, and the importance of using the family support network were also discussed.
In the phone-call session, the advanced CHC nurse obtained feedback on the parents’ work from the first session and how the family had progressed. The nurse used the parents’ motivation and empowerment to keep up with what they felt was working to manage the infant's sleep difficulties. The nurse evaluated the intervention and discussed whether some modifications or changes were required.
In the last session of the intervention, the advanced CHC nurse assessed the progress from the phone-call session and evaluated and mirrored the infant and parents’ reactions. This session's focus was explicitly on family relational practices, 15 on the child's self-soothing capability, and on supporting and securing the parents’ skills regarding the infant's regular sleep rhythm. The nurse encouraged parents to express how things were going and how they felt and showed empathy and understanding. The session aimed to help parents understand the possible causes of sleep disorders and what could interrupt the infant's sleep, such as sickness or family life changes in order to increase parental knowledge about sleep disorders and help them cope.
Further, through motivation and empowerment, the nurses discussed the progress in infant sleeping patterns and changes that might have occurred in family life. Thus, this session focused on family relations, how the parents felt they were handling the sleep problem, and whether they felt the interventions were working. Furthermore, the nurse offered some suggestions for the following months regarding parental expectations regarding the infant's sleep patterns.
Measures
Demographic information, such as participants’ age, education, employment, income, and marital status, and data regarding the child's sleep patterns over the day and night were collected. The participants completed three questionnaires (see Box 2).
The instruments used in the FES-BSBW intervention study.
The ICE-PFSQ is a 14-item questionnaire with two subscales: cognitive and emotional support. Scores range from 1 (low) to 5 (high). The instrument is both valid and reliable and has been psychometrically tested. Cronbach's alpha was 0.96 for the total scale, 0.87 for the cognitive support subscale, and 0.94 for the emotional support subscale subscales, respectively. 33 The instrument also measures perceptions of family support provided by healthcare professionals.
The ICE-FIBQ is a seven-item valid instrument that measures beliefs among family members regarding individuals with health problems. 34 It measures sleep pattern beliefs (1–5 range), regarding causes of sleep problems, effect, control, support, and suffering. Parents can be overwhelmed by difficult feelings and hindering beliefs, such as worthlessness and hopelessness. Beliefs may hinder adjustment, healing, and or recovery. Higher scores indicate greater assurance about a family member's beliefs. Cronbach's alpha for the questionnaire was 0.79. The instrument has been reported to be valid and has adequate test-retest reliability. 34
PedsQLTM is a 36-item instrument which was developed to evaluate pediatric health situations’ and its impact on quality of life for the family. It contains eight subscales that evaluate functioning in the following areas: physical, emotional, social, cognitive, communication, worry, daily activities, and relationships in families. This instrument has been validated, and Cronbach's alpha was 0.97. 35 Higher scores indicate better quality of life.
Data analysis
The study had a pre-post quasi-experimental design. 36 The Kolmogorov–Smirnov statistic 37 indicated normality of the data. In the findings, n varied based on the number of responses on each outcome variable (n differs because of incomplete data in some of the questionnaires). The missing data were not treated with a mean score, and only the true responses from each participant were used to calculate the sum score of the outcome variables. Descriptive analysis was conducted to sum the participant characteristics. 37 Paired t-tests were conducted to evaluate the differences between baseline and post-intervention scores 37 on family support, sleep pattern beliefs, quality of life, and postpartum depressive symptoms as well as mothers’ perception of infants’ longest sleep periods at nights, and number of nap periods during the day. IBM SPSS Statistics (version 24.0; IBM, Inc., Armonk, NY, USA) was used for data analysis. Differences were considered statistically significant at p < 0.05. 37
Ethical considerations
The ethical principles delineated in the Declaration of Helsinki guided the research. 38 This study was carried out with approval from the Ethical Committee of the CHC Centers in the Capital area and the National Bioethics Committee of Iceland (VSN-17-062). Potential participants received an information letter regarding the purpose of the study. The data are stored at the University of Iceland in a secure place at the Statistical Department, until the data have been analyzed. Only the researchers have access to the data.
Results
A total of 35 mothers who were the primary caregivers of infants with sleep problems participated in this study. The mothers’ ages ranged from 21 to over 36 years, but most of them (n = 24; 68.6%) were between 26 and 35 years old. Most mothers had university education (n = 25; 71.4%) and were married or cohabiting (n = 33; 94.3%). Most infants’ age ranged from 5–12 months (n = 28; 80%). Most infants were boys (n = 21, 60%). About one-third of the mothers were exclusively breastfeeding their child (n = 12; 34.3%), another third were only bottle feeding (n = 12; 34.3%), and a similar proportion were both breastfeeding and bottle feeding (n = 11; 31.4%) (Table 1).
Demographic characteristics of mothers of children with sleep difficulties (N = 35).
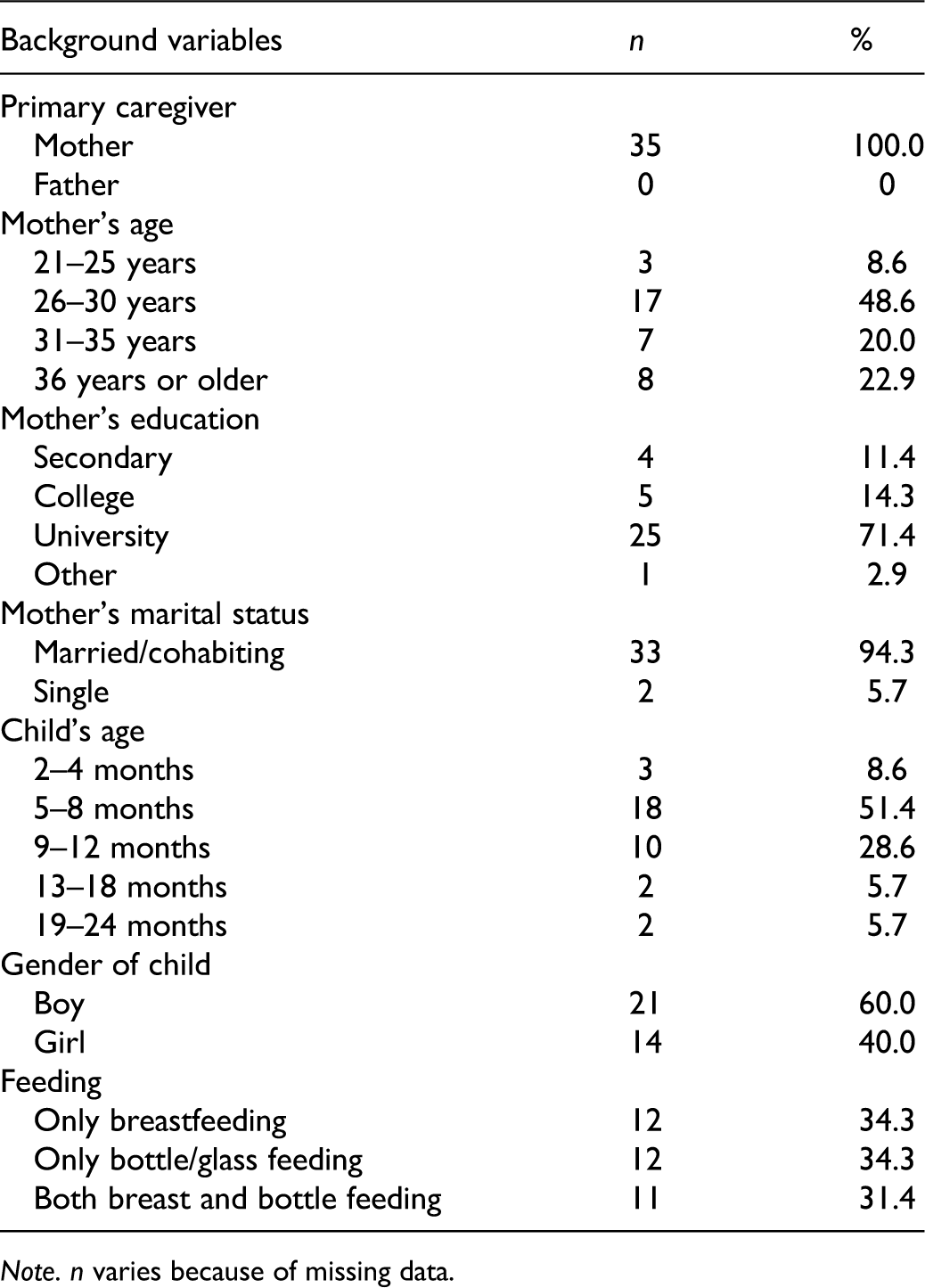
Note. n varies because of missing data.
Outcomes of the FES-BSBE intervention
A significant difference was found in mothers’ perceived family support after the FES-BSBW intervention (T2) compared to baseline (T1), when considering the total The Iceland Perceived Family Support Questionnaire (ICE-PFSQ) score (T1 mean = 32.40, T2 mean = 41.80; t = −3.94; p = 0.000), the cognitive support subscale (T1 mean = 14.61, T2 mean = 17.48; t = −2.73; p = 0.010), and emotional support subscale (T1 mean = 17.26, T2 mean = 24.16; t = −4.27; p = 0.000) (Table 2). Similarly, the mothers’ beliefs regarding their infants’ sleep patterns (Icelandic Family Illness Beliefs Questionnaire [ICE-FIBQ] scores) were found to be significantly different after the FES-BSBW intervention compared to baseline (T1 mean = 20.71, T2 mean = 25.11; t = −6.49; p = 0.000) (Table 2). Therefore, mothers reported being more knowledgeable about sleep disorders and experiencing more cognitive and emotional support from the advanced practice nurse after the intervention. Furthermore, the mothers also reported significantly more confidence in understanding the cause of sleep disorders and their impact on the family and what healthcare professionals offered to cope with the sleep disorder experience.
Comparison of mothers’ perceived family support, sleep patterns beliefs and family quality of life, before and after the family educational and support intervention ‘Better sleep better well-being’ (FES-BSBW) (N = 35).
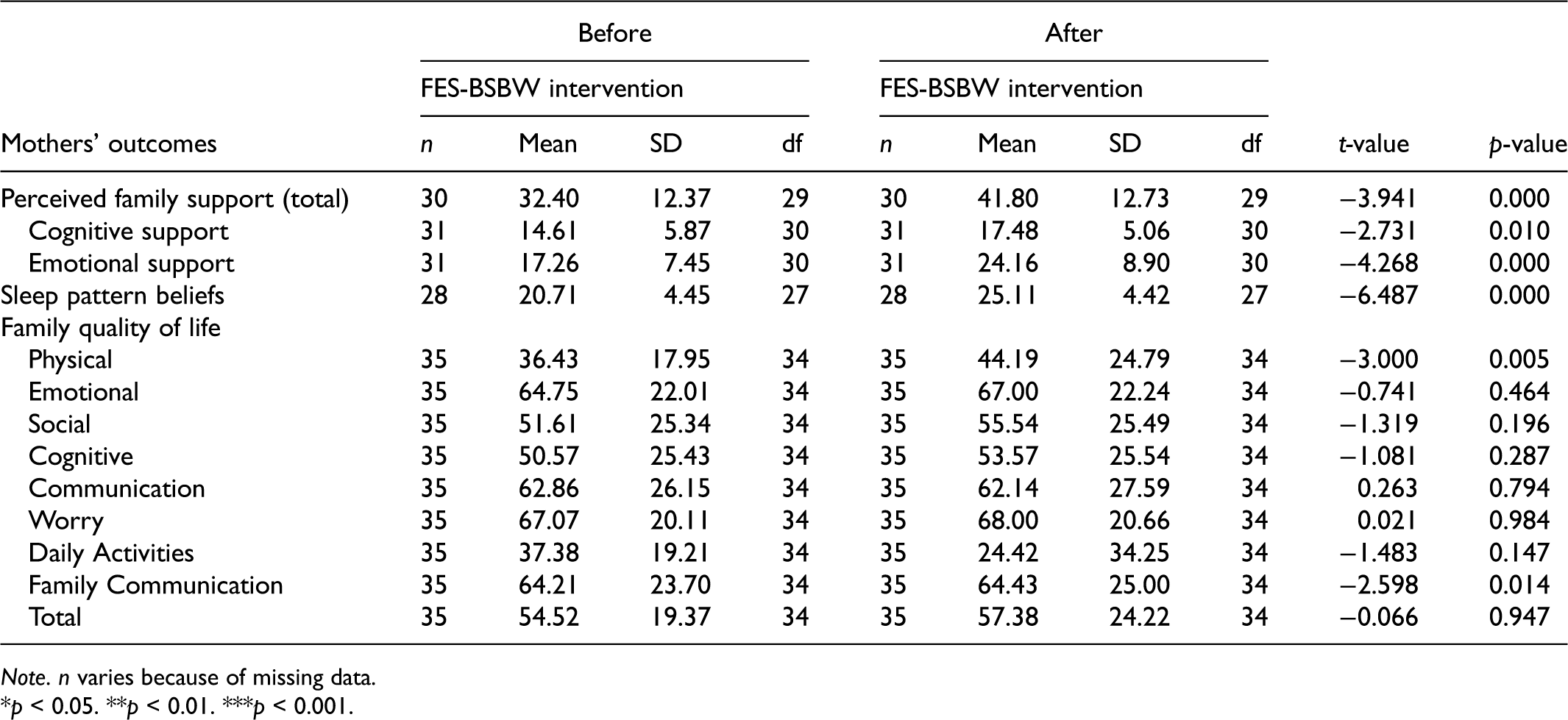
Note. n varies because of missing data.
*p < 0.05. **p < 0.01. ***p < 0.001.
The mothers rated their physical function (physical function subscale score) through their family quality of life scores (PedsQLTM – Family Impact Module), which was significantly better after the FES-BSBW intervention than before (T1 mean = 36.43, T2 mean = 44.19; t = −3.00; p = 0.005) (Table 2). However, there was no significant difference in any of the other subscale scores (i.e. emotional functioning, social functioning, cognitive functioning, communication, worry, daily activities, family communication) or the total score between baseline and after the FES-BSBW intervention (Table 2). Further, there was no difference between the mothers’ post-intervention scores for postpartum depressive symptoms and their baseline scores (Table 2). Nonetheless, all mothers had low scores (<12) before and after the intervention, indicating infrequent depressive symptoms.
Though the mothers’ perception of infants’ longest sleep period at night was perceived to be significantly longer per night after the FES-BSBW intervention compared to baseline (T1 mean = 3.62 h, T2 mean = 5.24 h; t = 3.47; p < 0.01) (Figure 1), the mothers also reported significantly lower number of infants’ nap periods per day after the FES-BSBW intervention than before (T1 mean = 2.66, T2 mean = 2.17; t = 3.37; p < 0.01) (Figure 2).
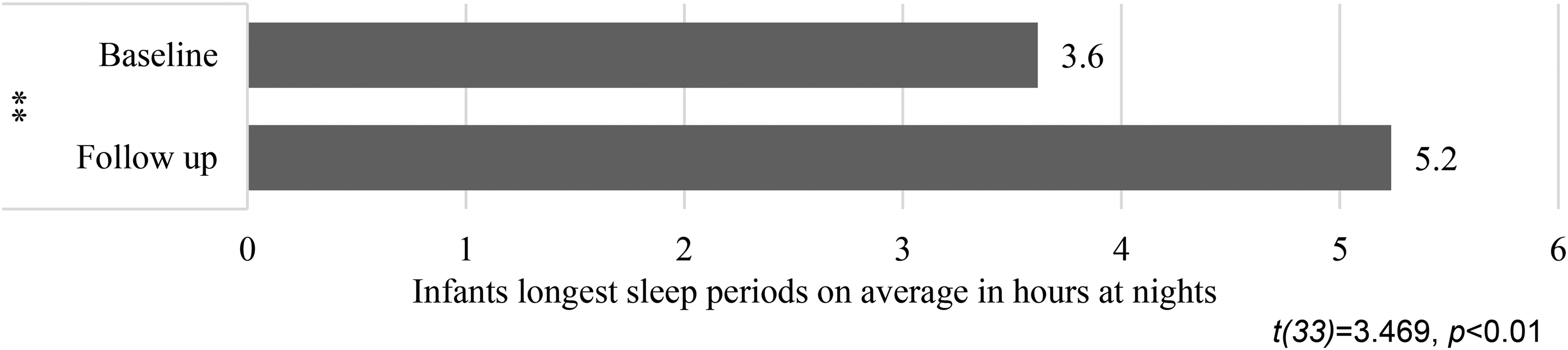
Mothers’ perceptions of infants’ longest sleep periods at nights.
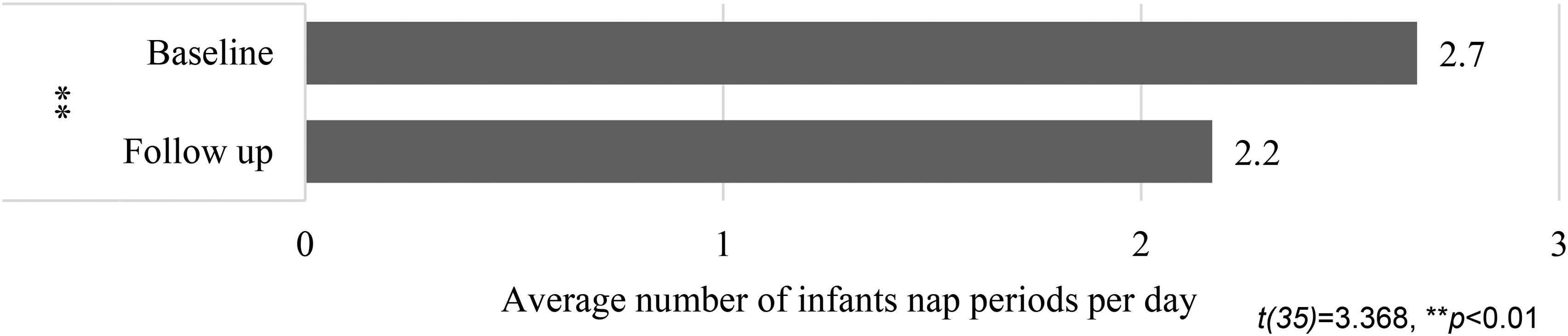
Mothers’ perceptions of number of infants’ daytime nap periods.
Discussion
The study hypothesis that the mothers of infants with moderate sleep problems who received the FES-BSBW intervention would report significantly higher perceived family support, improved sleep pattern beliefs and quality of life after the intervention compared to baseline was partly supported. This finding is new in that mothers felt their family was better supported both cognitively and emotionally. They perceived themselves to be more confident in handling their child's sleep problems and felt their physical functioning was better after the FES-BSBW intervention compared to baseline. Further, this finding emphasizes the requirement for advanced CHC nurses working in well-child-care units to offer the FES-BSBW intervention to families of children with moderate sleep difficulties. Moreover, it is noteworthy that the FES-BSBW intervention, which is evidence-based, 32 was delivered through advanced nursing practice within CHC centers. Thus, the FES-BSBW intervention was found to be beneficial to families and effectively applicable to well-child-care units.
Children with sleep problems rely on their parents recognizing their sleep problems and seeking appropriate support and healthcare practitioners’ interventions. In a systematic review of eight studies (four descriptive studies and four educational interventions), McDowall et al. 3 found that parents’ knowledge of child sleep was generally poor. However, more knowledgeable parents were more likely to report that their children exhibited healthy sleep practices. Moreover, small interventions demonstrated increased parental knowledge in the short term, but the effects were not maintained in the follow-up assessment. 3 Further, Field 9 reported in a review article with a variety of designs, where the main focus was on RCT studies, systematic reviews and meta-analyses, 9 that the study confirmed several educational/behavioral interventions. These interventions had been explored to manage infant sleep problems, such as consultations on sleep physiology and strategies to improve infant sleep, group teaching along with support calls, teaching sessions on destruction and bedtime fading (e.g. self-settling skills, no physical contact during crying, bedtime routines, such as bathing, cuddling), internet-based interventions and bedtime massage by parents, with some interventions showing improvements and other suggesting only short-term or small effects. However, out of 11 studies that addressed the impact of behavioral interventions during the first six months of life, eight studies showed improvement, highlighting the efficacy of early interventions. 9
Infants require support from their parents for their normal development, such as support for healthy sleep patterns, nutrition, and appropriate parent–infant interaction. Therefore, it is notable that both behavioral and relational (i.e. parent–child interactional) components of the FES-BSBW intervention were found to have a post-intervention impact on infants’ sleep patterns. This finding is interesting for advanced nurses practicing within CHC centers. It is in line with the findings of Hall and Nethery, 1 who used the Canadian Niagara Region Public Health and Emergency Services website to conduct a pilot study with 15 parents regarding key information about preventing and managing infant behavioral sleep problems. The authors found that parents actively used the tools and information offered, and about half of them wished to have follow-up telephone support from a public health nurse. 1
Although behavioral sleep interventions for infants with sleep problems have been on the rise and have been found to improve infant sleep problems, few studies have focused on both parents' involvement. Hall et al. 12 conducted a secondary data analysis of an RCT with 455 Canadian parents of healthy infants aged 6–8 months with sleep problems who received a behavioral sleep intervention. The experimental group received information about managing infant sleep problems, and the control group received information about managing infant safety risks. Assessments were conducted at six weeks post intervention and at follow-up at 24 weeks post teaching session. The main results indicated that at follow-up, most of the mothers (72.3%) reported their infant’s sleep as not a problem or a mild problem (72.3%), while at baseline, most of the mothers (81%) had identified a moderate–severe sleep problem.
Furthermore, the findings in this study from the FES-BSBW intervention are in agreement with those of the following studies: Hall et al. 12 who found that most mothers in the intervention group reported that their infant's sleep was not a problem or a mild problem after the behavioral sleep intervention relative to baseline; Matthey and Črnčec 11 who found a third to a half of parents who received an infant sleep problem intervention reported decreased infant sleep problems three weeks post intervention; Hall et al. 2 who found that parents who received a behavioral intervention for infant sleep problems reported an improvement in infant sleep difficulties compared to parents in the control group.
The strength of the FES-BSBW intervention is that it benefits families of infants and toddlers with moderate sleep problems through relational practices and educational and therapeutic conversations, delivered face-to-face at well-child-care units and via phone calls. The findings from the present study are also in line with those of Stuttard et al. 8 who found phone interventions for child sleep management to help parents. They are also compatible with those of Field 9 who found educational and behavioral interventions for infant sleep problems (e.g. strategies to improve infant sleep) to be effective.
Limitations
The main limitation of the study is the small sample size which limits the generalizability of the study. 36 Another limitation is the short follow-up measure which limits knowledge about possible long-term effects of the intervention. A third limitation is that only data from the mothers’ responses are reported in this study. The fathers or their partner caregivers were, in some cases, at work when the mothers attended the intervention sessions. Studies focusing on the benefit of the FES-BSBW program on the dyad or both mothers’ and fathers’ experiences are required. Further, the study design was a quasi-experimental, single-group study, limiting further the generalizability of the findings. Research with a larger sample size and an experimental or randomized control trial is required to determine the effectiveness of the FES-BSBW intervention.
Conclusion
Early interventions are beneficial for families to prevent sleep problems in infants and toddlers from escalating into more serious health problems later on. The FES-BSBW intervention, delivered at well-child-care units within CHC centers by advanced CHC nurses, is extremely valuable because of the improvements identified after this short-term intervention. The intervention contributed to better family health, as mothers reported higher family support, more positive sleep pattern beliefs, and enhanced physical functioning, which is vital for managing their infants' sleep difficulties. Although further research is required regarding the positive effects of the FES-BSBW intervention using a larger sample and an RCT design at CHC centers, the findings reported here regarding the benefits of the FES-BSBW intervention are promising.
Supplemental Material
sj-docx-1-njn-10.1177_20571585211044503 - Supplemental material for The ‘Better sleep better well-being’ intervention for parents of infants with moderate sleep problems: A quasi-experimental study
Supplemental material, sj-docx-1-njn-10.1177_20571585211044503 for The ‘Better sleep better well-being’ intervention for parents of infants with moderate sleep problems: A quasi-experimental study by Arna Skuladottir, Anna Olafia Sigurdardottir and Erla Kolbrun Svavarsdottir in Nordic Journal of Nursing Research
Supplemental Material
sj-docx-2-njn-10.1177_20571585211044503 - Supplemental material for The ‘Better sleep better well-being’ intervention for parents of infants with moderate sleep problems: A quasi-experimental study
Supplemental material, sj-docx-2-njn-10.1177_20571585211044503 for The ‘Better sleep better well-being’ intervention for parents of infants with moderate sleep problems: A quasi-experimental study by Arna Skuladottir, Anna Olafia Sigurdardottir and Erla Kolbrun Svavarsdottir in Nordic Journal of Nursing Research
Supplemental Material
sj-docx-3-njn-10.1177_20571585211044503 - Supplemental material for The ‘Better sleep better well-being’ intervention for parents of infants with moderate sleep problems: A quasi-experimental study
Supplemental material, sj-docx-3-njn-10.1177_20571585211044503 for The ‘Better sleep better well-being’ intervention for parents of infants with moderate sleep problems: A quasi-experimental study by Arna Skuladottir, Anna Olafia Sigurdardottir and Erla Kolbrun Svavarsdottir in Nordic Journal of Nursing Research
Footnotes
Acknowledgements
The authors want to thank the families that participated in the study for their contribution.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Icelandic Nursing Association and the scientific fund at Landspitali University Hospital (grant number LUH).
Conflict of interest
The authors declare that there is no conflict of interest.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.