
Abstract
The majority of healthcare visits in Sweden are within the primary healthcare centres with a wide variety of patients, ranging from children to the elderly, varying from trivial to the most acute. The aim was to describe nurses’ experiences of triaging patients at walk-in clinics at primary healthcare centres. Semi-structured interviews with 12 nurses, analysed using qualitative analysis, were used. The overall understanding was that a physical meeting with the patient gave the opportunity for eye contact and physical examination of the patient’s body. With broad expertise and experience, the informants felt more confident in their assessment. Cooperation between colleagues meant always having someone to consult when the informants felt unsure. The result highlight that triage is a challenging and complex task for informants. In order to be able to triage in an effective way, the informant must possess broad competence through solid knowledge and experience.
Introduction
The objective of the healthcare system in Sweden is good health. 1 Healthcare should be provided on equal terms to the entire population and with respect for the equal value of all people. 1 Swedish healthcare is financed mainly by county councils and municipal tax and city grants. Healthcare is free for all people younger than 20 years and older than 85 years. Adults pay a maximum fee of 110 Euro over 12 months for visits to outpatient care. 2 According to the national healthcare guarantee, when patients turn to the healthcare system, they have the right to contact with primary healthcare services on the day they seek help. An assessment of the patient’s health shall be made, and preference shall be given to patients who are in most need of care. 1
In Sweden, the county council is the principal unit of primary healthcare and is responsible for the basic requirements within medical treatment, nursing, preventative work and rehabilitation that does not require special skills or resources from the hospitals. 3 Primary healthcare is based in primary healthcare centres. This is the primary care facility the patients turn to when in need of healthcare. The patient is given an initial assessment and, if needed, the patients are directed to other care professionals or facilities. There are no exceptions in terms of types of diseases, age or patient groups assessed at primary healthcare centres. 1 The majority of healthcare visits in Sweden are within primary healthcare centres. 2 Reasons for patients to seek primary care can be due to rehabilitation, psychosocial interventions, health improvement, and disease prevention measures. 4 Primary healthcare centres are finding it increasingly difficult to manage the tasks of being first-line care facilities, as they are not always equipped to cope with the demographic challenges of a population that is aging and has an increasing number of chronic diseases and multimorbidity. 5
The assignment of primary healthcare is based on the staff having general expertise within the medical area. In primary healthcare, professions such as doctors, nurses, physiotherapists, occupational therapists, dieticians, counsellors, and psychologists are employed. Nurses are registered nurses with a three-year tertiary level of education with a bachelor’s degree. A community care nurse is a specialist nurse who has studied for an additional year at university level, with a master’s degree in community care. The community care nurse title is a protected specialist designation. 6 Consulting is one of the community care nurse’s specific areas of competence and the community care nurse should be able to assess the patient’s healthcare needs. 7
In primary care, some healthcare centres offer patients a walk-in clinic where the first contact is with a community care nurse who, after triage, sends the patient to the right care area. Here, the community care nurses’ full competence is used by letting the community care nurse work independently in delivering assessments, self-care advice, leadership and lifestyle consulting. 8 Previous research shows that nurse-led triage reduces the number of patient visits to physicians without increased mortality. 9 Overcrowded clinics block patients’ access to doctors, which compromises patient safety.9,10 The community care nurse-led triage in primary healthcare can lead to safer and more effective healthcare when patients, whose healthcare needs are not assessed, do not have to wait for a long time for a doctor. 8 A community care nurse-led walk-in clinic at the primary healthcare centre can improve the availability of healthcare centre for patients. Triage leads to more patients directly being referred to appropriate care areas.
The development of triage in primary care is a challenge because the knowledge community care nurses need to have in order to work at their full potential in primary care has not yet been described. 11 By describing community care nurses’ experiences of triaging patients in walk-in clinics of primary healthcare centres, factors that can benefit or hinder the triage process can be identified and the basis for an improvement plan can be worked out. The aim was to describe nurses’ experiences of triaging patients at walk-in clinics at primary healthcare centres.
Methods
This study was performed using a qualitative approach. Data collection was performed via interviews and analysed using qualitative content analysis. 12
Setting
The majority of healthcare visits in Sweden are within the primary healthcare centres. Some healthcare centres offer patients a walk-in clinic where the first contact is with a community care nurse who, after triage, gives the patient self-care advice and sends the patient home. Otherwise, the patient is directed to other care professionals or facilities. All the nurses in this study were working with triage in a walk-in clinic at a primary healthcare centre.
Participants and recruitment
The primary healthcare centres that offered walk-in clinics led by nurses, a total of 14 centres in one geographical area, were asked to participate in the study. The managers of the primary healthcare centres were contacted and given an information letter, informing them of the purpose of the study. Following the approval of the managers, they were then asked to provide email addresses for all registered nurses who met the inclusion criteria. The purposive sample provides participants who are knowledgeable experts within the area of the study. 13 The nurses who met the inclusion criteria were then contacted via email with information about the study. There were 12 nurses from five different health centres who agreed to participate in the study, and all came to be included.
Participants’ characteristics.
RN: registered nurse; CCN: community care nurse.
Data collection
Data were collected via interviews performed with one participant at the time during the spring of 2019. Ten interviews were performed at the participants’ workplaces during work hours and two interviews were performed in the participants’ homes. All 12 interviews were conducted by the two first authors (MG and ACP) in order to achieve consistency. 13 One author carried out the interview and the other author focused on audio taping the interview. During the interviews, an open-ended question was used: ‘Can you describe when you triaged a patient in the walk-in clinic?’ Two pilot interviews were conducted, no changes were made, and the pilot interviews were included in the material. 13 All interviews were recorded and lasted between 11–24 minutes (mean 16 minutes). All interviews were transcribed verbatim by the two first authors (MG and ACP).
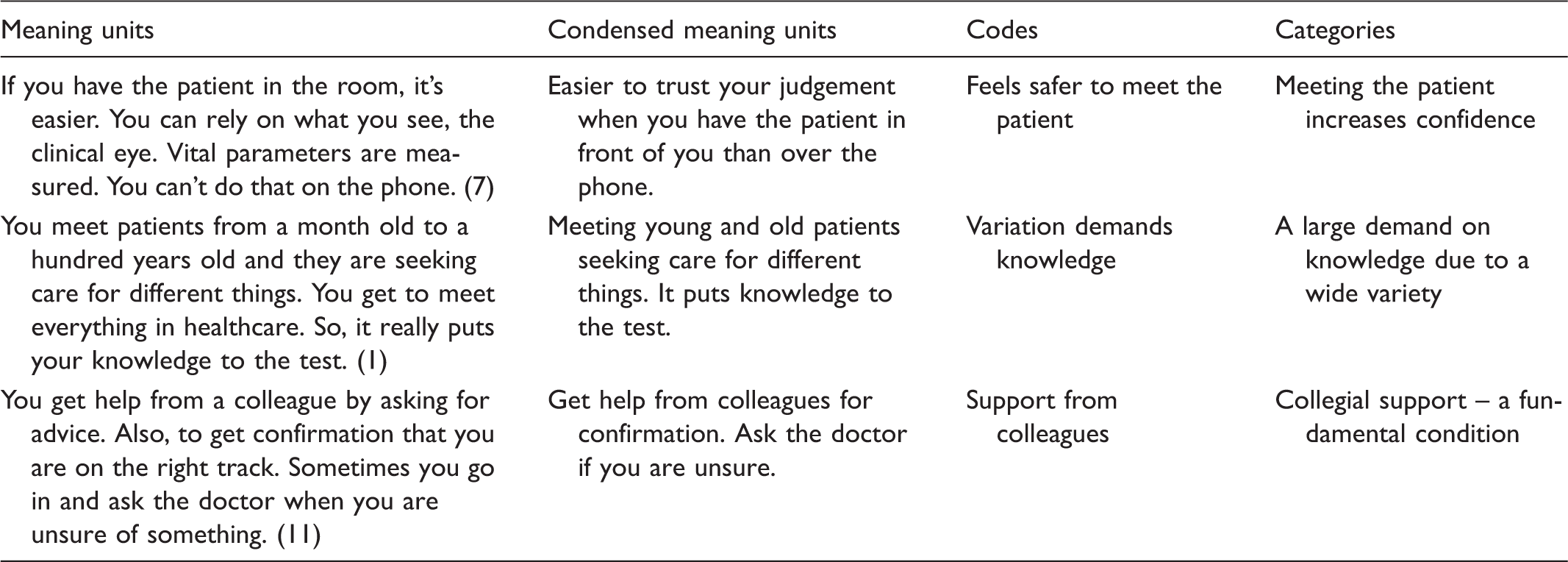
Data analysis
Text representing and reflecting the process of analysis.
Ethics
The study followed the ethical principals of the World Medical Association 14 about confidentiality and integrity. No personal information was collected or stored. The transcribed material was stored in a locked location at the university where only the researchers had access to it. Ethical approval was not needed according to Swedish law. 15 Informed consent to participate was obtained from each participant and they were also informed about the purpose of the study and their right to withdraw at any time14.
Results
The results present the informants’ experiences of triaging patients at walk-in clinics in primary healthcare centres in five categories: Meeting the patient increases confidence, A large demand on knowledge due to a wide variety, The necessity of a broad competence to meet the patients’ demands, Collegial support – a fundamental condition, and Stressful conditions.
Meeting the patient increases confidence
The informants’ experience reflected that triaging gave the opportunity to meet and confirm the patient. Furthermore, they had the opportunity to make full use of their triage skills during their meeting with the patient. Meeting the patient physically and being able to make a visual assessment led to a sense of safety compared to assessments made over the phone. The physical meeting gave the opportunity for eye contact and physical examination of the patient’s body, which facilitated the assessment. If you have the patient in the room, it is easier. You can form the clinical view, see and take vital parameters. You cannot if you have them on the phone. (3) Seeing the patient in front of you is easier in every way. Both being able to talk to the child himself and being able to show me his injuries. Instead of the parents trying to explain something they think is serious. (5) We visit the waiting room at regular intervals to do a quick scan of all patients. Not all patients say something even if they need help. It feels safer so you don’t miss a patient. (6)
A large demand on knowledge due to a wide variety
The informants’ experience reflected that the work involved a great variety, both in terms of which patients were seeking medical care and for what reason. The patients they met could be everything from sick children to fragile, multimorbid elderly, and causes for seeking medical care ranged from the trivial to the most acute. Also, patients could seek medical care for several different reasons at the same time, which further complicated the assessment. With this wide variety, the informants saw the importance of possessing both experience and knowledge. Assessments were made based on the level of the informant’s knowledge and this could vary depending on how long the informant had worked in primary care. There are both those of us who have been working for many years and those who are new. It is clear that we make different assessments based on how long we have worked in primary care. (8) You need to be able to do a bit of everything; surgery, orthopaedics, paediatric and primary care. If you have worked for a while, you will be able to do it. (11)
The necessity of a broad competence to meet the patients’ demands
The informants experienced that patients desired to get help quickly, which led to the informants trying to streamline their work by asking fewer questions. At the same time, the informants emphasized the importance of asking a lot of questions and thus not getting stuck in a specific diagnosis. The patients need to be cooperative because I ask a lot of questions. And many patients may think it just takes a lot of time. (4) It can be good to use the decision support sometimes. I can identify things even when there are circumstances that make it difficult or easier to triage. (12)
In the situations where the informants had experience, they felt more confident in their assessment, which resulted in more patients going home with self-care advice instead of seeing a doctor. When I know I have the knowledge. Then I feel calm and have the situation under control. I can be responsible for sending the patient home. (10) … I have done the assessment at this point of time. You do not have pneumonia. But I can’t say what happens in three days. (1) With the patient being triaged, you can never read up in advance. You cannot prepare for things you do not have the knowledge for. You bring the patient into the room and ask the patient: How are you? (9) It requires a lot of knowledge from the nurses because it is a reflection over every patient. Sometimes it is easy and sometimes it is difficult. But there must be resources. Some patients should see a doctor. (5)
Collegial support – a fundamental condition
A prerequisite for ensuring that triaging was correct was that the informants experienced good cooperation between colleagues at the healthcare centre and had someone they could consult when they felt uncertain. Sometimes there was a doctor who was directly linked to the walk-in clinic, which was very helpful to the informants. We have a doctor on site. You can consult and get support from the doctor. (2) When the system works and there are doctors to consult, reservation times at the physiotherapist and occupational therapist, the walk-in clinics are the absolute best solution. The patient receives a qualified medical assessment and we guide them to the correct care. (12) You have some freedom when you really need help. You go to a colleague with expertise in a certain area or a doctor and explain. Now I am in the middle and do not really know what to do. (7) We are much quicker to let children see a doctor right away. They get a better triage than when we do it. They do not have to sit and wait either. (3)
Stressful conditions
The workload at a walk-in clinic could vary, and the informants’ experiences revealed how it could be stressful to see a lot of patients in the waiting room. When the informants experienced that everything was running smoothly, they were able to cope with the situation. The experience of stress was greater when a patient took a long time to assess while there were many patients in the waiting room waiting for an assessment. It can feel quite stressful when many patients are waiting. Especially if you have a patient who takes a long time. (2) You triage one patient at a time, and you try to have structure. I think it’s fun not knowing what’s coming. You get to meet the patient directly and may or may not have a patient journal on the side. (6) How I handle the stress depends on my personal condition for that day. Your personal life plays an important role, especially if everything is ok at home. When I have a good day, I see one patient at a time, and I am doing a good job. (10)
Discussion
The informants highlighted that it was easier to triage and make patient-safe assessments at walk-in clinics versus over the telephone. Triaging over the telephone may be limited by the possibility that information can be obtained only verbally, and it is the patients’ interpretations of problems that are communicated. 16 It has emerged from previous research that this restriction can be experienced as a patient safety risk. 17 To triage patients at a walk-in clinic where a meeting takes place can increase patient safety versus traditional triage over the telephone. The results showed that it was considered necessary to quickly identify which patients were acutely ill to avoid long waiting times before receiving an assessment. Often it was the informants who scanned the waiting room. Previous research has described that it is common for nurses to browse the waiting room and make a first assessment based on their intuition. 18 However, it can be discussed whether it is possible to make an initial assessment without obtaining any information and there is a risk that the nurses have an overconfidence in their intuition. In other words, it is necessary to set out guidelines for how patients who are acutely ill are quickly identified in a safe and effective way.
The informants highlighted the importance of having experience in order to make competent assessments. This is also demonstrated in other studies where the nurses describe how experience facilitates the assessments and makes them feel confident. 18 Depending on the informant who triaged the patients and what knowledge she possessed, assessments were different, which could result in patient safety being jeopardized. Hitchcock et al. 19 confirm in their study that assessments varied depending on how much triage experience the nurse had. In order to ensure patient safety in a walk-in clinic, it is therefore advisable that triage is conducted by experienced nurses. It is also necessary to create clear guidelines on the requirements that should be placed on nurses working with triage at walk-in clinics. Similar findings have been made in Wolf et al’s 18 study, where they conclude that recently graduated nurses without clinical experience were not suitable for triage.
In addition to experience, continuous training was something that informants considered necessary in order to make correct assessments. Clinical knowledge is the basis for feeling a sense of satisfaction and confidence in the profession as well as for performing the right assessments. 20 As triaging poses a challenge, nurses need to improve their clinical skills through theoretical and practical training. Regular training in triage increases the ability of the nurses to cope with stressful situations and develop an ability to identify the severity of the patients’ symptoms and determine the appropriate diagnoses. 21 For maintaining effective triage, it is necessary to have continuous education. Accurate triage will also avoid straining medical resources as it ensures the efficient use of resources. 22
The informants described that it was a challenge to triage elderly multimorbid patients as their needs were often complex. The proportion of severely ill elderly is increasing and the National Board of Health and Welfare 23 states that all healthcare professionals who encounter these patients should possess specific geriatric skills. To be able to triage based on the elderly’s unique needs, knowledge is needed as they can exhibit atypical symptoms, have other reference values in terms of vital parameters and have a different metabolism of drugs than the general population. 24 If the nurse at triage does not possess specific knowledge about the health of the elderly, these patients run the risk of being wrongly assessed. Some healthcare centres in this study had a specific clinic for elderly patients helping with the triaging as well. This can also be a way of ensuring patient safety for the elderly.
The results showed that decision support in the form of a handbook was not always used in the assessments. When the informants expressed having a solid level of experience, they stated that they used decision support to a lesser extent. The use of decision support is a way to standardize assessments, and studies show that standardized care is important to reduce trust in memory and thus generate better care.25,26 Research shows that decision support, in combination with experienced nurses who feel they have plenty of time and a well-functioning organization, contributes to increased patient safety and streamlined triaging where the sickest patients are identified faster. 23 Using decision support to a lesser extent can, therefore, be seen as a risk for patients’ safety. More extensive use of decision support minimizes the risk of patients having different assessments.
Collegial support was considered to be a prerequisite for being able to triage patients safely. Some walk-in clinics had a doctor who was available for the informants to consult and this was perceived positively. Studies suggest that patient safety increases when nurses are supported by other colleagues. 22 Experienced nurses also perceive themselves as having better qualifications for providing safe care compared to younger nurses with less experience. 27 In order to provide safe care, a nurse must be aware of his or her limitations and take on the expertise of other staff. 25 There should, therefore, be doctors and specialist staff covering in the areas of expertise where the triaging nurse does not possess enough knowledge or the skills to be able to make a patient-safe assessment. It can be elderly patients, children or patients with mental illness.
The informants experienced it as stressful when triaging at walk-in clinics in situations where their competence was not sufficient enough. Stressful conditions at triage may constitute a patient safety risk. 17 Yoder-Wise 11 points out the potential of well-prepared, experienced and self-confident advanced practice registered nurses in primary care. Yoder-Wise means that the nurse in primary care is underused and to use their talent to function to their full capacity would enhance care. But they must be prepared appropriately which is an issue in clinical settings.
Methodological considerations
There are some limitations in this study. The interviews have only been conducted within one geographical area which can be seen as a weakness since it may have affected the results as the variation in socio-economic conditions and the size of the geographical coverage may vary. 13 A further consideration may be that only women participated in the study. However, the purpose of the study was not to shed light on any differences between the sexes. Instead, it can be a strength that a purposeful sampling of participants reflects the clinical situation. 28 Primary healthcare centres are female-dominated workplaces. Thus, the sample can be said to represent the wider population of professional care providers’ at primary healthcare centres.
In this study, qualitative content analysis was considered appropriate due to the data collected. In content analysis, there is the risk that data will be reduced so that the overall meaning changes. 13 Trustworthiness, that is, dependability, credibility and transferability, have carefully been achieved in accordance with Elo et al. 29 Dependability, the stability of data over time and under different conditions, is ensured by the criteria used to select participants being well described so that other researchers may follow the decision trail. Also, detailing the participants’ main characteristics enables the transferability of the results to other contexts to be assessed. To achieve credibility, it is important to evaluate how well categories cover the data and to identify any similarities within and differences between categories. A detailed descriptions of the analysis process and the use of a table to explain the categorization process in this study enables an assessment of credibility. 29 To enable further assessment of the trustworthiness of the data processing, representative quotations have been used in the presentation of the results. Some minor adjustments have been made to the presentation of the results to ensure the participants’ confidentiality. A strength in this study was that discussions of the analysis were conducted in a critical and open dialogue among the researchers (ACP, MG and AA) regarding the design of categories to determine trustworthiness. 29
Conclusion
A clinical implication in this study is based on the profile of the triage nurse presented. With the wide variety of patients, having prior experience of triage is imperative. Furthermore, having a broad knowledge of different clinical areas, such as diseases, injuries, diagnoses and treatments, is of great importance and value. Experience and knowledge depend on the time worked in primary care and are thus vary between nurses. A broad experience and knowledge are described as advantageous because this results in the nurse being self-sufficient in often complex triage.
In their work at walk-in clinics, the experienced nurses continuously scan the waiting room for an assessment of all waiting patients. Any patients in acute need of care are immediately identified. During triage, to make a visual assessment of the patient is to be prepared for the next step in the patient care. Both experience and knowledge enhance the triage nurses’ ability to anticipate what to expect. This results in a sense of safety and of being in control of the situation, in comparison to an assessment made over the phone.
Another clinical implication in this study is based on the description of how conditions can be improved for the triage nurse. Continuous skills development and keeping their basic education up to date improves the conditions for effective triage. It also increases triage nurses’ confidence during assessments. Confidence results in having control of the situation and therefore being able to handle stress.
Written decision support in the form of a triage handbook must be easy to navigate, in order to be used. Otherwise the nurses will rely on their own knowledge which will vary dependent on the nurses’ own experiences. When the triage nurse has access to consult expertise in different clinical areas, the nurse can triage all sorts of patients in a correct and effective manner.