
Abstract
Background
Community nurses play a crucial role in managing pain, a prevalent yet often inadequately addressed symptom in community settings. Persistent knowledge gaps among healthcare providers contribute to inconsistent pain management, potentially compromising patient outcomes.
Objectives
This study is designed as a pre- and post-course observational study aiming to assess baseline pain knowledge among community nurses in Singapore and evaluate the effectiveness of an interdisciplinary pain education programme.
Methods
43 community nurses completed a pre-course questionnaire assessing self-reported clinical knowledge and objective pain knowledge using the Clinical Pain Knowledge Test (CPKT). Following an interdisciplinary pain education programme, 34 nurses completed the post-course questionnaire. Changes in self-reported clinical knowledge and CPKT scores were analysed, and multivariable linear regression was used to identify predictors of post-course knowledge scores.
Results
Baseline pain knowledge among community nurses was modest with a mean pre-course CPKT score of 49.1% (±12.8%). Post-course, there was a significant improvement in overall knowledge scores (mean 58.4% ± 14.1%, p < 0.001). While improvements were observed in most CPKT domains, there was no significant change in the application of knowledge in clinical conditions. Less experienced community nurses demonstrated the greatest improvement post-course.
Conclusion
Structured pain education programmes effectively enhance nurses’ theoretical knowledge, particularly among those with less experience in community nursing. However, translating this knowledge into clinical application remains challenging. Standardised pain education and interdisciplinary training approaches may further strengthen pain management competencies in community settings.
Keywords
Introduction
Community nursing has emerged as a prominent focus of healthcare in recent years, assuming an increasingly significant role in preventive health initiatives and the provision of comprehensive, community-focused patient care.1,2 As frontline healthcare providers, community nurses address a broad range of health issues, with pain being one of the most prevalent and significant symptoms reported by patients—yet it often remains inadequately recognised and managed. 3
Numerous studies consistently identify persistent knowledge gaps among healthcare professionals in the assessment and treatment of pain.3–5 Systematic reviews highlight that nurses’ pain knowledge and attitudes frequently fall below recommended benchmarks.6–8 For instance, one review of 18 studies involving 7942 nurses reported an average knowledge level of 52.9%, 7 which is significantly lower than the desired 80% benchmark. 7 This deficit is not a recent phenomenon as another systematic review examining nursing students’ knowledge over two decades revealed no significant improvement in pain knowledge and attitudes, 9 indicating a persistent educational challenge. Specific areas of concern consistently identified in the literature include inadequate understanding of pain assessment tools, appropriate analgesic administration methods and the application of theoretical knowledge in complex clinical situations.4,5,10,11 Furthermore, nurses’ personal biases and fears regarding opioid addiction often contribute to the undertreatment of pain,5,12 underscoring the critical need for targeted education initiatives.5,13
While general nursing pain knowledge has been extensively explored, a detailed understanding of pain knowledge specific to community nurses in Singapore and the impact of tailored educational interventions in this unique setting remains important. This study aims to provide valuable contribution by assessing the baseline pain knowledge of community nurses in Singapore and evaluating the effectiveness of an interprofessional, multifaceted pain education programme in enhancing competency in pain management.
Methods
Study design and participants
The study was designed as a pre- and post-course observational study involving community nurses in Singapore, allowing for the evaluation of changes in the nurses’ pain knowledge before and after the educational intervention. An ethical waiver was obtained from the SingHealth Centralised Institutional Review Board due to the study’s classification as a service evaluation. Participation was voluntary, with completion of the questionnaire serving as implied consent. A total of 43 nurses participated in the pre-course assessment, of which 34 of these nurses also completed the post-course assessment.
Pain education course
The educational intervention was a structured two-week course designed according to interprofessional education (IPE) principles and best practices in pain management. 14 It addressed the complex, biopsychosocial nature of pain through a multifaceted approach, 15 including virtual and in-person lectures, as well as interactive discussions led by an interdisciplinary team comprising physicians, advanced practice nurses, pharmacists, psychologists, physical therapists and acupuncturists. The curriculum covered key topics such as pain pathophysiology, assessment tools, pharmacological and non-pharmacological treatments, and clinical decision-making. The course concluded with a hands-on session where nurses applied their learning to patient cases, bridging theory and practice — an essential step in enhancing clinical pain management competencies. 16
Data collection
At the beginning of the course, participants were assigned unique identifiers to ensure pre- and post-course responses could be matched while maintaining anonymity. Demographic information was collected, and participants completed a self-reported clinical knowledge assessment and the Clinical Pain Knowledge Test (CPKT) 17 prior to the educational session. At the end of the course, they were required to complete the same assessment. Participants were provided a two-day window before the course to complete the pre-course assessment and an additional two-day window after the course for the post-course assessment.
Assessment instruments
The self-reported assessment evaluated each participant’s perceived confidence and competence in various aspects of pain management. Participants rated their responses on a five-point Likert scale (1 = Not at all confident/knowledgeable, 5 = Very confident/knowledgeable), evaluating their confidence in using standardised pain assessment tools, ability to identify different pain types and perceived knowledge of pharmacological and non-pharmacological pain management strategies including the risks and side effects of commonly used pain medications.
Additionally, the Clinical Pain Knowledge Test (CPKT) 17 served as a validated instrument to assess the nurses’ knowledge of pain management. This 23-item multiple-choice questionnaire, designed with a single-best-answer format, evaluates knowledge across four core domains: the multidimensional nature of pain, pain assessment and measurement, pain management strategies, and the application of knowledge in clinical practice. Each question was weighted equally, with incorrect responses scored as zero and correct responses scored as one.
Statistical analysis
Baseline characteristics were reported using descriptive statistics: categorical variables as numbers and percentages, normally distributed data as mean ± standard deviation (SD), and non-normally distributed data as median with interquartile range (IQR). These statistics were presented for the overall group of nurses and stratified by whether they completed the post-course questionnaire. To examine differences in the self-reported clinical knowledge of pain assessment and management pre- and post-course, the Wilcoxon signed-rank test was used for each question.
To determine the pre- and post-course clinical pain knowledge among community nurses, CPKT domain and total scores were calculated as [(no. of correct responses)/(total no. of questions in domain)]*100, to give the percentage of questions with correct responses. Both the median (IQR) and mean ± SD CPKT domain and total scores were reported. The Wilcoxon signed-rank test and paired t-test were used to determine if there were differences in the post- versus pre-course CPKT domain and total scores, respectively. The exact McNemar’s test was used to determine if there were differences in the correct responses for individual CPKT items post- versus pre-course as the number of discordant pairs were less than 25.
Univariable linear regression with robust standard errors was used to explore the baseline characteristics associated with the post-course and pre-course CPKT total score. Multivariable linear regression with robust standard errors examined if these associations persisted after adjusting for potential confounders. Potential explanatory characteristics were selected a priori and forced into the multivariable model simultaneously to minimize bias in the estimated coefficients. 18 The unadjusted and adjusted B coefficients with 95% confidence intervals (CIs) were reported. The Box-Tidwell test assessed if there was evidence of non-linearity between the CPKT total score and continuous covariates. Statistical tests were two-sided with a 0.05 significance level. All analyses were conducted using Stata 18 (College Station, TX: StataCorp LLC).
Results
Baseline characteristics of community nurses overall, and by whether they took the post-course clinical pain knowledge test.

CKPT: Clinical Pain Knowledge Test; IQR: Interquartile range; SD: Standard deviation.
aCategories are not mutually exclusive.
bCPKT total scores are calculated as [(no. of correct responses)/(total no. of questions)]*100, to give the percentage of questions with correct responses.
Self-reported assessment
Self-reported clinical knowledge of pain assessment and management pre and post pain education course.
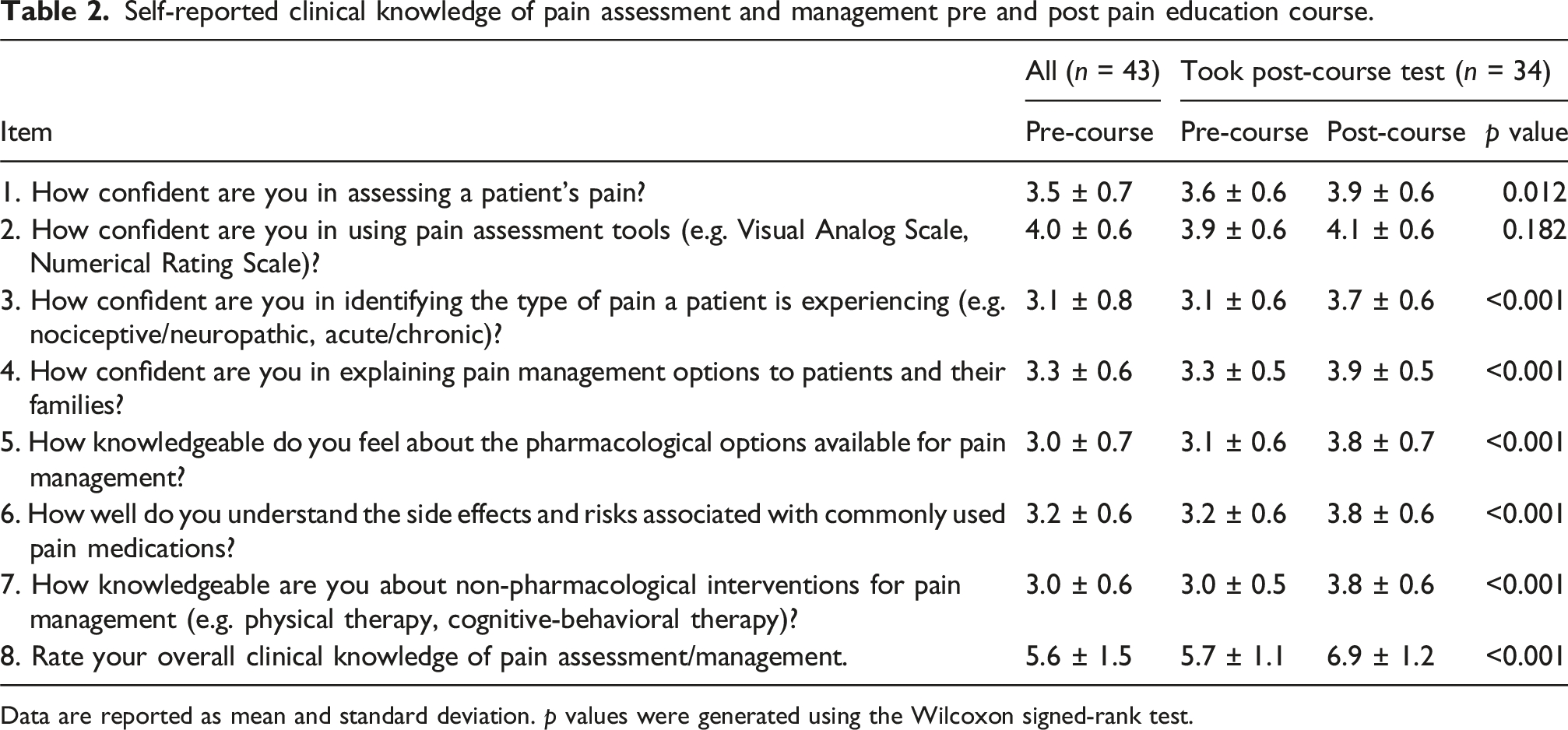
Data are reported as mean and standard deviation. p values were generated using the Wilcoxon signed-rank test.
Clinical pain knowledge test
Clinical pain knowledge pre and post pain education course.

CPKT domain and total scores are calculated as [(no. of correct responses)/(total no. of questions in domain)]*100, to give the percentage of questions with correct responses. The median (25th percentile, 75th percentile) scores and mean ± standard deviation domain and total scores are reported. P values were generated using the Wilcoxon signed-rank test for CPKT domain scores and paired t-test for CPKT total scores.
CPKT: Clinical Pain Knowledge Test; IQR: Interquartile range; SD: Standard deviation.
aItem 1–4 in CPKT.
bItem 5–10.
cItem 11–19.
dItem 20–23.
Characteristics associated with clinical pain knowledge
Baseline characteristics associated with post-course clinical pain knowledge.
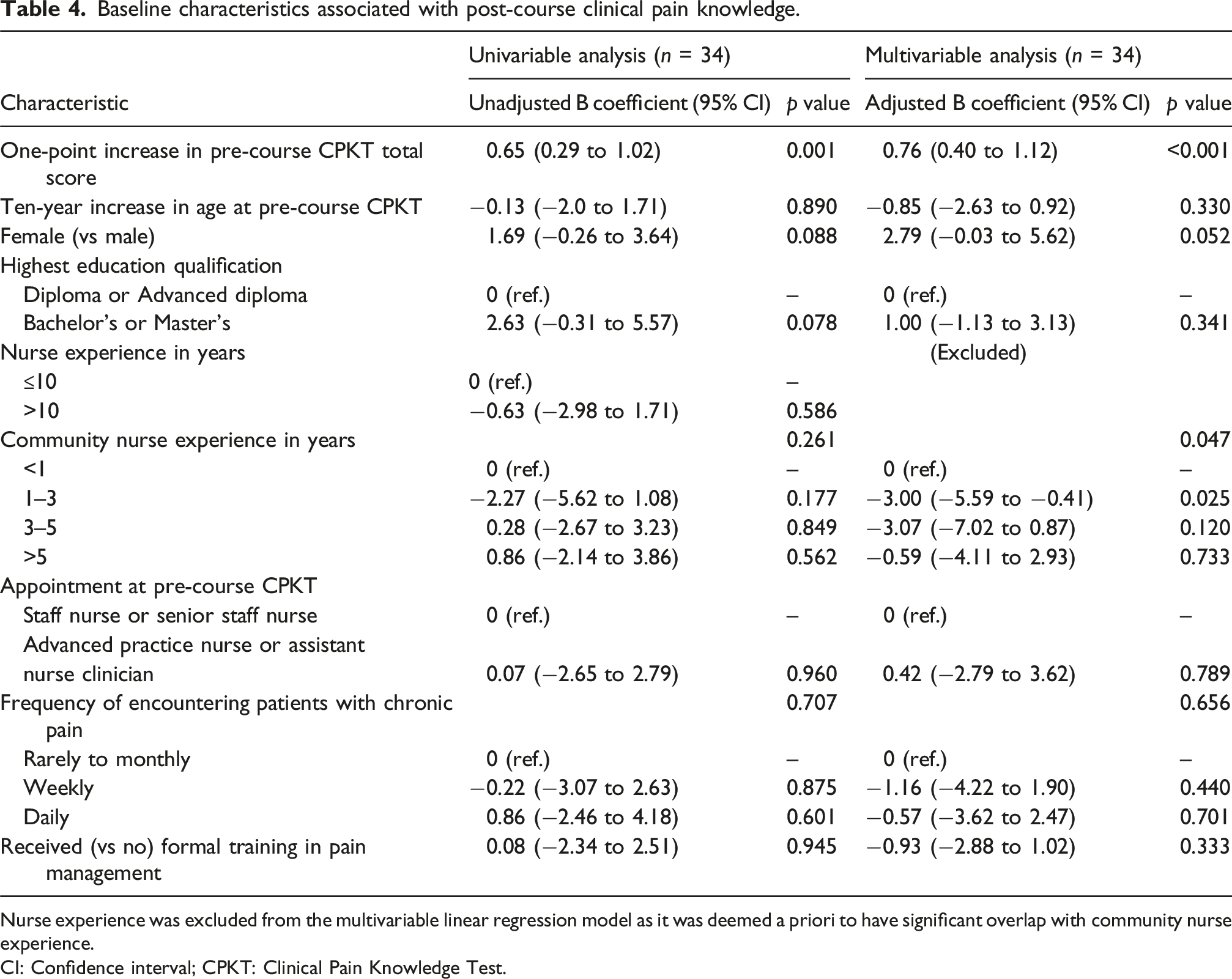
Nurse experience was excluded from the multivariable linear regression model as it was deemed a priori to have significant overlap with community nurse experience.
CI: Confidence interval; CPKT: Clinical Pain Knowledge Test.
Among 34 nurses who took the post-course test, multivariable linear regression showed that a one-point increase in pre-course CPKT total score was independently associated with a 0.76 higher (95% CI 0.40 to 1.12; p < 0.001) mean post-course CPKT total score.
Among 9 nurses with <1 year of community nurse experience, there were a mean 13.6 correct responses post-course compared to 9.6 pre-course (paired t-test p = 0.014). Among 7 nurses with 1–3 years of experience, there were a mean 11.3 correct responses post-course compared to 10.3 pre-course (p = 0.198). Among 6 nurses with 3–5 years of experience, there were a mean 13.8 correct responses post-course compared to 13.3 pre-course (p = 0.518). Among 12 nurses with >5 years of experience, there were a mean 14.4 correct responses post-course compared to 12.2 pre-course (p = 0.004). After adjusting for all covariates including pre-course CPKT score, compared to nurses with <1 year of community nurse experience, nurses with 1–3 and 3–5 years of community nurse experience may have a 3.00 lower (95% CI −5.59 to −0.41) and 3.07 lower (95% CI −7.02 to 0.87) mean post-course CPKT total score, respectively (p = 0.047).
While there was a lack of evidence that various baseline characteristics were associated with the mean pre-course CPKT total score, we could not exclude the possibility that greater community nurse experience may be independently associated with a higher mean pre-course CPKT total score (Supplemental Table 2). Box-Tidwell tests did not show evidence of non-linearity for any of the multivariable linear regression models.
Compared to male nurses, female nurses had similar pre-course CPKT score but had a 2.79 higher (95% CI -0.03 to 5.62; p = 0.052) mean post-course CPKT total score
Discussion
Nurse characteristics and baseline pain knowledge
The median age of nurses was 36 years, with the majority possessing over a decade of total nursing experience. Additionally, approximately one-third had more than 5 years of community nursing experience. The pre-course Clinical Pain Knowledge Test (CPKT) scores among community nurses in this study were moderate, with a mean total score of 50.3% (±12.2%). This aligns with findings from previous research, where nurses’ pain knowledge has been reported to range between 40–60%,19–22 depending on clinical setting and prior education. Baseline characteristics between nurses who completed the post
Influence of educational qualifications and prior training experience
The majority of nurses held a bachelor’s or master’s degree (81.4%), with the minority holding diplomas (18.6%). While higher educational qualifications are generally expected to correlate with greater clinical knowledge and competence, our regression analysis did not reveal a significant association between education level and baseline CPKT scores. This finding challenges a common professional expectation and suggests that comprehensive pain education may not be consistently or sufficiently emphasised within standard nursing curricula, reinforcing the need for specialised, targeted courses to address this specific knowledge domain.
Furthermore, less than a third of nurses reported having received formal pain management training. Although nurses with prior clinical experience in specialties such as Surgery or Palliative Care would possibly have had more exposure to pain management in their practice, this exposure did not translate into significantly higher baseline knowledge scores in our regression analysis. This observation suggests that informal and experience-based learning, while valuable, may not provide the systematic and evidence-based foundational knowledge in pain management that structured educational programmes offer. Therefore, even nurses with relevant specialty experience may significantly benefit from dedicated pain education to reinforce and formalise key concepts, bridging the gap between practical exposure and comprehensive theoretical understanding.
Influence of community nursing experience
Multivariable linear regression analysis revealed that pre-course CPKT total score was the strongest independent predictor of post-course CPKT performance. Although nurses with more community nursing experience tended to have higher pre-course scores, their post-course scores demonstrated less improvement than those with less than 1 year of community experience, after adjusting for all covariates (Table 4). This suggests that targeted pain management courses are likely to be most valuable for newer community nurses.
Influence of gender
Although most participants were female (86%), gender was not significantly associated with baseline CPKT scores. However, female nurses exhibited a trend toward higher post-course scores, with borderline statistical significance (p = 0.052). This trend aligns with prior research suggesting that female nurses may demonstrate higher pain knowledge or more positive attitudes towards pain management in certain contexts.9,12 Further research could explore potential gender-based influences on pain knowledge.
Post-course improvements in clinical pain knowledge
The significant improvement in overall CPKT scores following the course (increase from mean total score of 49.1% to 58.4%, p < 0.001) reflects the effectiveness of the pain education program in enhancing community nurses’ clinical knowledge. However, the domain-specific results provide a more nuanced understanding of the outcomes. Nurses demonstrated improvements in three of the four core CPKT domains: the multidimensional nature of pain, pain assessment and measurement, and pain management strategies. In contrast, no improvement was observed in the domain of knowledge application to clinical conditions. This suggests that the programme successfully strengthened theoretical knowledge but also highlights the challenge in translating that knowledge into clinical decision-making. Pain management in community settings often involves navigating patient-specific complexities, logistical constraints and evolving care protocols — factors that may be difficult to address through didactic learning alone. These findings highlight the need for supplementary hands-on training, case-based discussions or follow-up sessions to reinforce practical skills and to bridge the gap between knowledge acquisition and clinical application.
A similar trend was observed in the self-reported assessment, which demonstrated improvements across most domains and closely aligned with the objective CPKT results. However, confidence in using pain assessment tools remained unchanged. This may be attributed to the relatively high baseline confidence levels reported in this area which could have resulted in a ceiling effect, limiting the potential for measurable improvement. While the course effectively enhanced conceptual understanding, translating this knowledge into clinical confidence may require sustained practice, mentorship and repeated exposure to real-world patient interactions.
Limitations
Methodological limitations
The pre- and post-course questionnaires were not completed under observed and timed conditions which may have influenced participant responses. However, allowing nurses to complete the questionnaires at their convenience likely better reflect mastery of content, as compared to time-restricted formats. 23
Additionally, nine participants (21%) were lost to follow-up, resulting in missing data that may introduce the potential for selection bias as nurses who completed the post-course questionnaire may have been more engaged or motivated to learn, potentially inflating the perceived effectiveness of the course. However, the remaining sample still comprised 79% of the initial participants, preserving a substantial portion of the study population. Sensitivity analyses or strategies to minimise dropout could strengthen future studies.
Validity and generalisability
The study was conducted at a single centre with a relatively small sample size which may limit the generalisability of the results to other community nursing settings. Additionally, we did not include a control group which limits our ability to attribute improvements solely to the intervention. However, the primary aim was to assess the impact of the course on participating nurses, rather than to compare it against alternative interventions.
The CPKT, while validated in other contexts, has not been specifically validated for community nursing practice in Singapore, potentially affecting the relevance of the assessment. Adaptations or a localised validation of the tool could enhance the assessment’s relevance to this specific population. However, it remains a rigorously developed questionnaire for assessing pain knowledge among nurses, having four core domains which cover essential competencies, making it a reasonable proxy for evaluating foundational knowledge.
Despite these limitations, our study provides important insights into the baseline pain knowledge and the effectiveness of pain education among community nurses in Singapore.
Conclusion
This study highlights that baseline pain knowledge among community nurses in Singapore is modest but that structured pain education programmes can significantly enhance understanding. In particular, less experienced community nurses may benefit most from such educational interventions. Standardising pain education within nursing curricula could further ensure consistent foundational knowledge across all nurses. Furthermore, interdisciplinary pain education programmes, exemplified by the approach taken in this study, provide a multifaceted perspective on pain management and reinforce a comprehensive approach to treatment.
Translating theoretical knowledge into clinical practice, however, may require more hands-on approaches, such as real-life case scenarios, decision-making simulations and ongoing mentorship. Future research could include longitudinal follow-ups to assess knowledge retention and determine whether educational improvements translate into better clinical practices and patient outcomes.
Supplemental Material
Supplemental Material - Assessing pain knowledge among community nurses in Singapore: A pre- and post-education course study
Supplemental Material for Assessing pain knowledge among community nurses in Singapore: A pre- and post-education course study by Luo Huiyi Joanne, Koh Xuan Han, Marlinda Ali, Rafidah Binte Abdul Rahim, Prit Anand Singh and Lydia Li Weiling in Proceedings of Singapore Healthcare
Footnotes
Acknowledgements
The first author gratefully acknowledges Mr. Vincent Mingyi Luo for his valuable insights and guidance in the preparation of this manuscript.
Ethical considerations
An ethical waiver was obtained from the SingHealth Centralised Institutional Review Board due to the study’s classification as a service evaluation.
Informed consent
Verbal informed consent was obtained from all subjects before the study. Written informed consent was not obtained because participation was voluntary, with completion of the questionnaire serving as implied consent.
Author contributions
LHJ and LLW conducted the literature review and conceptualised the study design. KXH performed the data analysis. MA and RBAR contributed to participant recruitment, protocol development, and delivery of the education course. LLW and PAS provided oversight and supervision of the course implementation. LHJ coordinated ethical approval. LHJ and KXH wrote the manuscript. All authors contributed to the review and critical revision of the manuscript and approved the final version for submission.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analysed during the current study are available from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.