
Abstract
Registered nurses’ (RNs’) perceptions and understanding of the health problems and care needs of patients with chronic obstructive pulmonary disease (COPD) play a crucial role in the quality and continuity of care. This qualitative multiple-case study aimed to explore how RNs identify patients’ problems and care needs during home visits to older adults with COPD. In addition, the study explored the agreement and disagreement between RNs’ and patients’ perceptions and priorities regarding problems and needs. The study followed consolidated criteria for reporting qualitative research (COREQ). Data were collected through observations of five home care visits, interviews with RNs, and mapping forms administered to both RNs and patients. Deductive content analysis of five cases revealed that RNs identified the patients’ problems through observation, dialogue, and direct questions during home visits. RNs and patients had different perceptions of the patients’ problems and care needs, particularly regarding psychosocial and communication-related issues. This knowledge contributes to improvements in patient safety in COPD care.
Introduction
Chronic obstructive pulmonary disease (COPD) is a prevalent and debilitating respiratory condition, particularly among older adults. 1 Patients with COPD often have multiple comorbidities, which can further complicate their care. 1 Therefore, registered nurses (RNs) must observe and identify the health problems and care needs of these patients to be able to provide individualized care and integrate patient preferences into the care planning process.2–4
The ability to recognize patients’ problems is linked to knowledge of their clinical and personal information, which is an essential element of everyday nursing practice.5,6 In addition, studies have emphasized the essential connection between information exchange about the patient and nurse-patient communication.7–9
The concept of ‘knowing the patient’ is widely discussed in the nursing literature as a crucial factor in identifying patients’ problems and has been highlighted as a prerequisite for providing quality care.5,10 In a previous study, 2 we found that familiarity with patients with COPD enabled nurses to detect changes from the habitual state, not only related to disease but also to patients’ well-being and functioning in their daily environment. Knowledge of the patient was an essential component of nurses’ clinical judgment and ability to respond to care needs, as also demonstrated in other studies.11,12
Research has shown that communication between RNs and patients plays an important role in understanding patients’ problems and care needs9,13 and that poor communication affects the outcomes and quality of care. 9 Therefore, RNs’ communication skills play a crucial role in identifying and exploring patients’ problems and have a positive impact on patient outcomes and the delivery of safe patient care. 14 Research has highlighted challenges in communication between healthcare workers and older persons in home care15,16 and pointed out room for improvement in nurse–patient communication in this setting.9,17 The importance of patients’ participation in communicating their perceptions and prioritization of their problems has been recognized for many years. 18 The term ‘patient participation’ is often used interchangeably with ‘patient involvement’.19,20 In this paper, the concept of patient participation refers to patients actively engaging in communication with RNs by expressing their perceptions and prioritization of their problems.
The research is limited regarding the agreement between RNs’ and patients’ perceptions of problems and needs in home care settings. However, some studies have shown that in the context of pain relief in home care, nurses rate pain intensity lower than patients’ self-reports. 21 Moreover, research from hospital settings has shown that patients often report their problems as being more severe than RNs, especially in areas such as nutrition, sleep, pain, and emotions. 22
Our study is based on the knowledge that RNs working in home care use their nursing and communication skills to identify COPD patients’ problems, provide appropriate treatment, and prevent exacerbations. 2 Crucially, these skills influence the RNs’ perceptions and prioritization of problems experienced by vulnerable older patients diagnosed with COPD. To our knowledge, no research has explored perceptions and prioritization among home care nurses and older adults living with COPD.
Our study explored how RNs identify patients’ problems and care needs during home visits to older adults with COPD. In addition, it investigated the agreement and disagreement between RNs’ and patients’ perceptions and priorities regarding problems and needs.
The following research questions guided the study:
How do RNs identify the patient's problems and care needs during home visits? What do the RNs and patients agree/disagree about in terms of perceptions and prioritization of the patient's problems and care needs?
Methods
A qualitative multiple-case study following Yin's 23 framework was conducted to explore the perceptions of patients’ problems within the context of home care visits. A case was defined as a home care visit made by an RN to an older patient with COPD. The study employed non-participatory observations of the RN–patient interaction during the home care visits, individual semi-structured interviews with the RNs, and mapping forms completed both by RNs and patients.
The multiple-case study design allows for an in-depth exploration of phenomena within a natural context, utilizing multiple sources of information. This design facilitates a rich and nuanced understanding of the research topic. It also enables the examination of commonalities and differences within and between cases, even with a small selection of cases. 23 The COREQ 24 checklist was used for reporting.
Setting and participants
In Norway, the provision of long-term care falls under the jurisdiction of municipalities, encompassing nursing homes and home care services. Due to national political initiatives and a growing population of older people with persistent health ailments, such as COPD, municipal healthcare services have assumed a role in caring for patients with complex medical needs. 25 This study took place between October 2017 and October 2018 in four municipalities in central Norway, encompassing both urban and rural areas. In Norway, RNs carry out home care visits based on decisions from the municipal health service concerning the patient's need for care.26,27
The first author distributed written information about the study and a request to conduct research to the health administration in each municipality. This request was then passed on to the home nursing care leaders by the health administration. The home care leaders assisted in disseminating the information and facilitating communication with potential RN participants.
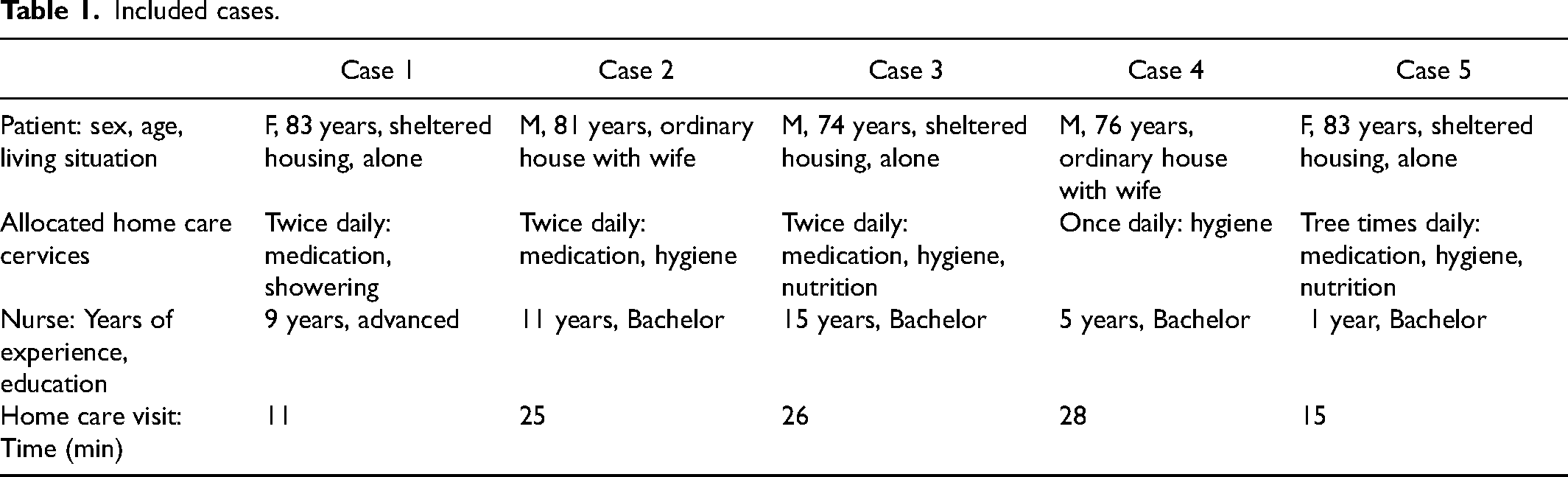
The inclusion criterion for the RNs was a minimum of 6 months of employment in home care services. A total of five RNs were included in this study. The participating RNs were requested to identify suitable patients who were receiving home care services for inclusion in the study. The inclusion criteria for patient participants were a diagnosis of COPD, age 70 years or older, residence in a sheltering house or ordinary home, receipt of daily home care services, and the ability to complete the mapping form. Three male and two female patients were included in this study. All patients received multiple daily home care services, which encompassed supervision and assistance with hygiene, medication management, and nutritional needs (Table 1).
Included cases.
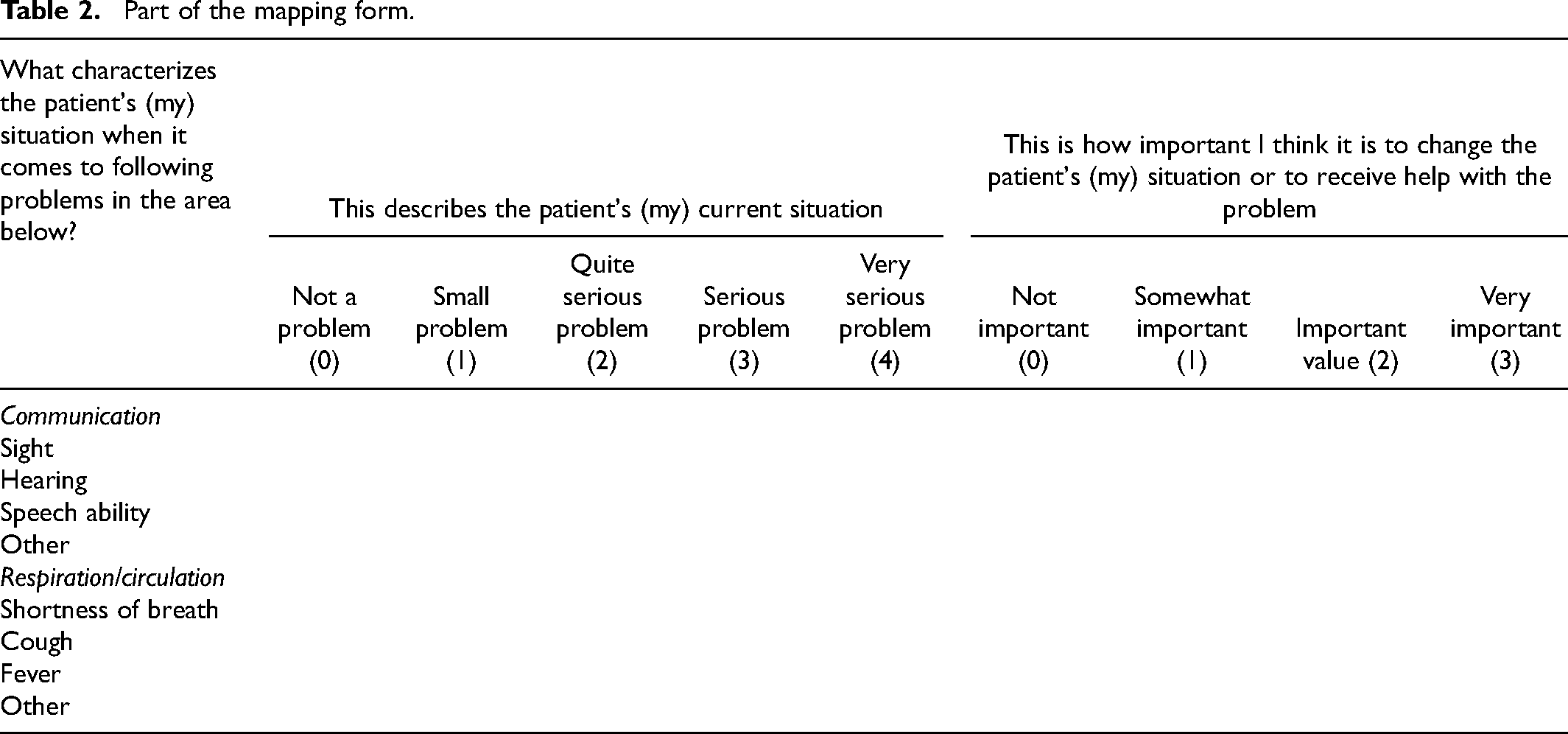
Part of the mapping form.
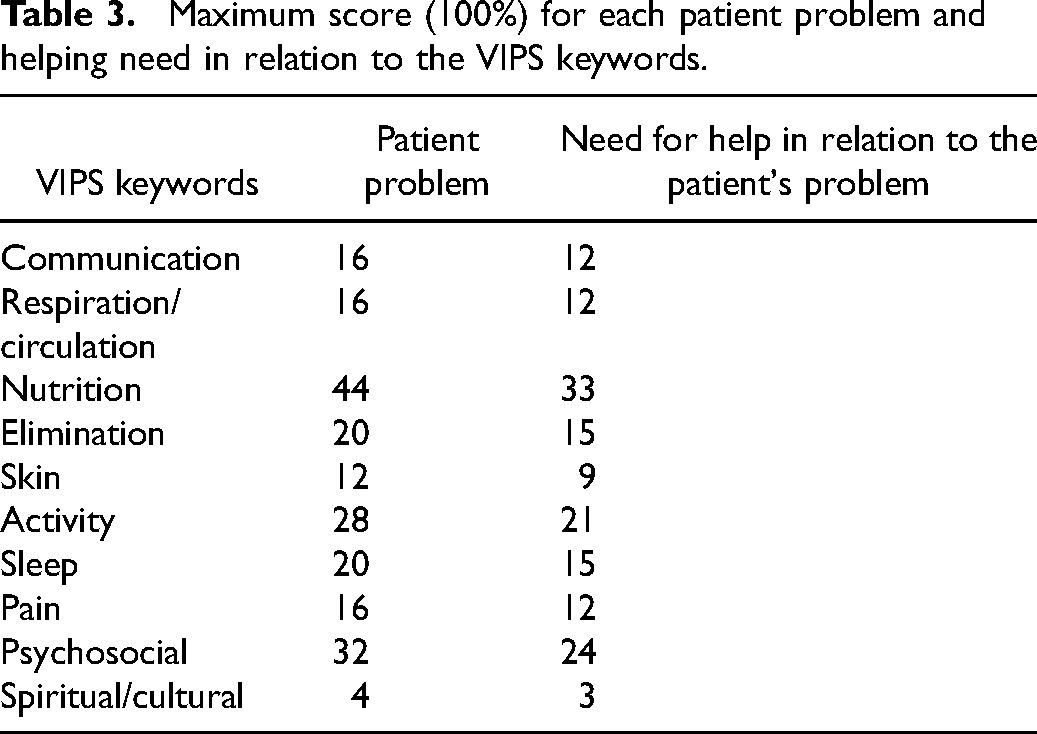
Maximum score (100%) for each patient problem and helping need in relation to the VIPS keywords.
Data collection
Data were collected through non-participatory observations of RN–patient interactions during routine home visits and individual semi-structured interviews with the RNs, conducted by the first author immediately after the visits. In addition, mapping forms were completed by both the RNs and the patients right after the visits to answer the second research question.
Observation
The non-participatory observations were performed by the first author during five home care visits and involved observing the RNs’ and patients’ interactions. The RNs were encouraged to vocalize their thoughts according to the think-aloud method to facilitate the examination of communication concerning patient problems and care needs in each case during the home care visits. 28 The think-aloud method is recognized as an effective technique for collecting qualitative data during problem-solving processes29,30 and has been employed in several nursing studies. 31 Each home care visit was audio-recorded and later transcribed verbatim by the first author. Field notes were taken as supplements.
Interviews
All interviews with the RNs were conducted face-to-face immediately after each home care visit in the RN's company car or office. The interviews followed a semi-structured format, which included follow-up questions. Each interview lasted 10–15 min. The RNs were asked about their impressions and knowledge of the patients, including their thoughts on important aspects of the patient's health condition to report according to the visit. The interviews were audio-recorded and later transcribed verbatim.
Mapping forms
To determine the concordance between the RNs’ and patients’ perceptions of the patients’ problems and care needs, an identical mapping form was administered to both the RNs and the patients immediately after each visit. The mapping form was inspired by a questionnaire created by Florin, Ehrenberg and Ehnfors 22 and consisted of 52 items organized into 10 categorical labels based on the VIPS model for documenting nurse care, developed by Ehrenberg et al. 32 These labels, as applied to needs and problems, are communication, breathing/circulation, nutrition, elimination, skin/integument, activity, sleep, pain/perception, psychosocial, and spiritual/cultural. Each of these VIPS labels was further divided into sub-labels via graded questions, allowing for an exploration of the severity of the patients’ problems. Every VIPS key label had 2–10 sub-labels and a maximum score. In addition, to assess the perception of the importance of help needed for each patient problem, graded questions regarding the need for help were integrated into the same mapping form. The answer options in the mapping forms were designed to address the patient's health problems. For each label, the answers were graded as follows: 0 = not a problem; 1 = a small problem; 2 = quite a serious problem; 2 = a serious problem; and 4 = a very serious problem. Similarly, the answer options for the importance of help connected to each patient problem were graded as follows: 0 = not important; 1 = somewhat important; 2 = important; and 3 = very important.
Data analysis
A deductive approach was employed for the data analysis. All authors participated in the analysis process. The first author performed the initial analysis, which was followed up by the other authors. The VIPS model32,33 served as the overarching theoretical framework to guide the assessment and categorization of the text for both the observations and the interviews. Since Krippendorff 34 states that content analysis allows researchers to look for both the meaning and quantity of registrations in a communication, this method was chosen to answer the first research question. The software NVivo 12 was used to organize text from the observations and interviews.
In the analysis of the transcripts from the observations, interviews with the RNs, and field notes, data related to 10 VIPS keywords corresponding to the labels used in the mapping forms were identified. The statements from each case formed clusters corresponding to the VIPS keywords. Content analyses were conducted on the text for every VIPS keyword, resulting in the emergence of categories. The extracted statements were organized into a matrix according to the VIPS model for both each case and all cases together to obtain an overall impression of the results. Since the multiple-case study design according to Yin emphasizes both within-case and cross-case analysis, the with-in analysis was used in every case and cross-analyses were applied to compare and identify patterns across cases.
The next step in the analysis was to make the mapping form responses from the RNs and patients comparable. Using Microsoft Excel, the response statements from the mapping forms were converted into numeric values and graphs, with two graphs per case: one showing the perceptions of the patient's problems (both RN and patient) and the other showing the perceptions of the patient's need for help (both RN and patient), as a percentage of the maximum score for each label. These graphs revealed consensus and deviations in the reported severity of the patient's problems, as well as the reported importance of care needs associated with each reported patient problem in each case, as shown in Figure 1.
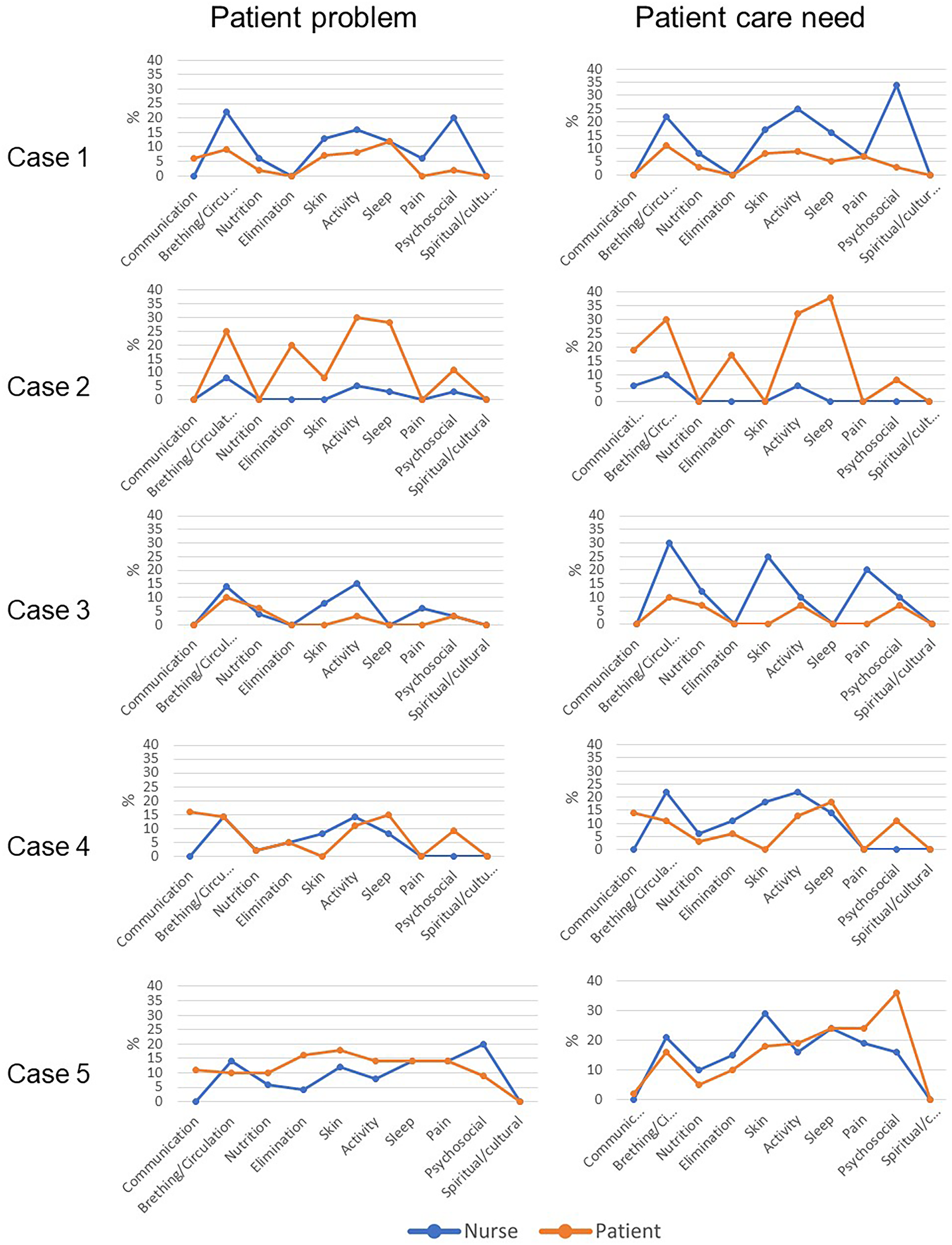
Nurses’ and patients’ perceptions and priorities of patients’ problems.
Finally, the results from the qualitative analysis and the descriptions of the mapping forms were compared case-by-case to examine the expressions of the patient's problems and care needs during the home visits, as well as to assess how the RNs identified these parameters.
Ethical considerations
The research was approved by the Norwegian Centre for Research Data (No. 54983), and authorization for data collection was obtained from the health administration in the municipality. Participants were informed about the study and gave written consent before data collection. The participants were notified in advance about the audio recording of home visits. Participants were assured that their involvement was voluntary and that they retained the right to opt out of the study at any time.
Results
Three approaches emerged in how the RNs identified the patients’ problems and care needs during the home visits: direct questions; dialogue; and observations.
Direct questions refer to questions asked by the RN that could be answered with a ‘yes’ or ‘no’. These also included questions that had no follow-up but remained with a simple ‘good’ or ‘not bad’ answer.
Dialogue means that the RN was communicating with the patient in a transmitter-receiver conversation where the RN and the patient participated equally.
Observations in this study refer to the RNs’ observations of the patient's physical, psychological, and emotional well-being in relation to VIPS keywords, looking for deviations in the patient's state of health.
The mapping forms gave insight into the patients’ and RNs’ perceptions of the patients’ problems and their severity and need for help related to these problems. Figure 1 shows the differences and similarities in these perceptions. Neither RNs nor patients responded to questions regarding patient problems and care needs for spiritual/cultural issues. The main findings and disagreements are presented as a summary of each case. Case 1: An 83-year-old woman living alone in sheltered housing
The RN who had a longstanding relation to the patient utilized observation, direct questions, and dialogue to identify the patient's problems and needs, with observation as most prominent. During the visit, the RN observed the patient's appearance and posture, surroundings, and asked direct questions and engaged in dialogues with the patient. Direct questions about the patient's respiration appeared as ‘…but you haven’t become worse than you were before the weekend? Yes?… No?… Same as before? – not as bad as this summer?’ The patient replied just: ‘No’.
The RN observed and guided the patient through the nebulizer treatment through dialogue with the patient. The RN reported that she could gauge the patient's psychosocial well-being by observing the twinkle in the patient's eye and the patient's ability to make jokes. However, the patient invited the RN to a dialogue of a psychosocial nature by saying, ‘It's sad sometimes…. many times, I wish I could let go’. The RN responded with a simple ‘hmm’, without responding to the patient's concerns in a dialogue. The RN also described the same patient as ‘a very cautious lady’. The RN did not ask direct questions to the patient related to psychosocial matters during the visit. The mapping form revealed differences between the RN and the patient in the reports of patient problems; the largest difference was in the perception of psychosocial issues, with the RN assigning higher scores. The patient reported sleep as her primary issue, while the RN reported breathing/circulation as the main problem. In terms of help needed for patient problems, the patient prioritized assistance with breathing/circulation, activity, and skin, while the RN emphasized the importance of help related to psychosocial, activity, and breathing/circulation (Figure 1). Case 2: An 81-year-old man living in an ordinary house with his wife
Observation, dialogue, and direct questions were used to identify the patient's problems and needs, with dialogue and direct questions being most prominent. The RN looked for deviation in the patient’s health condition, based on knowledge of the patient’s ordinary health condition. ‘It is essential to know the patient, in relation to recognizing the situation as normal,’ the RN said. However, some direct questions asked by the RN were not pursued, such as, ‘Do you notice worsening of the disease yourself?’ The patient replied, ‘Yes’. ‘You have challenges that you live with?’ ‘Yes,’ the patient said. During the visit, the RN and the patient engaged in a dialogue when the RN prepared the nebulizer. This dialogue was about the patient's nutrition and breathing issues and included the patient's wife, indicating a familiar relationship. Serious issues, such as the reversibility of the illness, were also discussed, although the patient did not engage in this part of the conversation.
The mapping form revealed disparities between the RNs and the patient's report. The patient prioritized activity as the primary issue, followed by sleep and breathing/circulation, while the RN identified breathing/circulation as the main problem, followed by activity and communication. The most pronounced difference in perceptions was for activity and sleep, which the patient prioritized. Activity and sleep issues were not discussed during the visit. The patient expressed a need for help with sleep, which the RN did not prioritize. Conversely, the RN reported breathing/circulation as the patient's most important need for help; the patient scored this need higher than the RN. In addition, the patient reported needing help with psychosocial and elimination, which the RN did not report as a problem (Figure 1). Case 3: A 74-year-old man living alone in sheltered housing
In this case, the RN's direct questions, such as inquiring about the patient's preference for coffee or water, were most prominent. The RN posed follow-up questions to gather detailed information about the patient’s health status: ‘Are you still in pain after you fell?’ to which the patient replied ‘No’. The RN followed with: ‘Not at all?’ Then the patient said: ‘Yes, I do, in the shoulder’. In the interview, the RN related that the patient has challenges with toilet hygiene, resulting in development of wounds, which the patient ignored. The RN explained that this matter therefore requires attention.
The RN conveyed her familiarity with the patient, indicating a longstanding relationship between the two of them. The RN demonstrated an understanding of the patient's history and emotional state. The interaction revealed a shared sense of humor: The RN said ‘You don’t have strawberry jam as you wanted!’ ‘I know,’ the patient replied, laughing, pleased to fool the RN.
The mapping form indicated small differences between the RN's and the patient's perceptions of the patient's problems and needs. However, the RN reported larger problems compared to the patient's own report, with the greatest difference shown in activity, skin, and pain. The patient prioritized breathing/circulation, nutrition, activity, and psychosocial as primary problems and help needs, aligning with the RN's report, except for the issues related to skin. These issues were all highlighted by the RN in the visit (Figure 1). Case 4: A 76-year-old man living in an ordinary house with his wife
The RN used all three approaches to identify the patient's problems and needs. Dialogue appeared as most prominent. Mostly, the patient seemed to control the dialogue. The RN said about this patient ‘He tells how he wants things, and in what order’.
The RN asked the patient: ‘Do you use oxygen at night?’ To which the patient replied: ‘yes’. There were no follow-up questions from the RN. The dialog between the RN and the patient was filled with humor and jokes and revealed an established relation. The RN did not report psychosocial problems like those reported by the patient in the mapping form. The RN described: ‘He is so easy to get along with, and he has such a great sense of humor’.
The largest discrepancy was shown in communication, followed by psychosocial, which the RN did not report as problems. The patient's primary expressed concern was communication, followed by sleep, while the RN reported breathing/circulation and activity as the patient's main issues. The patient reported a need for help with psychosocial, whereas the RN did not perceive this as a problem. The most important problem in terms of help needed reported by the patient was sleep, whereas the RN prioritized breathing/circulation and activity over sleep (Figure 1). Case 5: An 83-year-old woman living alone in sheltered housing
The RN had known this patient for 1 year. The RN approached the patient through observation, dialogue, and direct questions, where dialogue appeared to be the most prominent. The RN said she was looking for changes in the patient's health condition, such as skin tone or edema. She said, ‘looking for problems… that's why I just talk a little about it, because she gets anxious quickly’. The RN asked the patient ‘Are you doing well?’ The patient replied: ‘Yes’. Then the nurse asked: ‘Have you slept well?’ and the patient answered: ‘I have been sleeping well to 5 or 6 o’clock. Then I got tendon strain.’ Then, a conversation about the weather started. The patient responded to the RN's statement that not all days are the same by saying: ‘Yes, it's something one should be grateful for on the days one can have… but not all days are equally bad’. The RN did not pursue the patient's statement. The RN said later about the patient, ‘There is a reason why she takes Sobril, she is very anxious. Her anxiety is strongly connected to her breathing.’
The patient's problems that were prioritized in the mapping form were not communicated during the visit. The largest disparity was shown in elimination, where the patient reported high concern, and psychosocial, where the RN gave the highest score. They differed in concern about communication, with the patient expressing higher concern. The patient reported skin as her biggest problem, while the RN reported psychosocial as the patient's primary issue. The patient prioritized the need for help related to psychosocial followed by communication and sleep. The RN reported skin issues as most important, followed by sleep, then breathing/circulation. The greatest difference was in communication and psychosocial, with the patient giving them a higher score (Figure 1).
Discussion
The aim of the present study was to explore how RNs identify patients’ problems and care needs during home visits to older adults with COPD, as well as the agreement and disagreement between RNs’ and patients’ perceptions and priorities regarding patients’ problems and needs.
Our findings revealed that RNs utilized observation, dialogue, and direct questions to identify the patient's problems and needs. Some patients’ problems, such as psychosocial issues, were not communicated during the visits. The RNs claimed to know the patients but were unaware of the patient's prioritized problems. The mapping forms reflected individual perceptions of the patient's problems, revealing disparities in the reported severity of problems and perceptions of care needs between RNs and patients. However, there was substantial agreement between RNs and patients regarding breathing/circulation problems.
Identifying the patient's problems and care needs during home visits
As shown in our earlier research, the RNs observed the patients to detect changes in the patients’ problems and needs based on their professional knowledge and familiarity with the patients’ health status. 2 The observed communication patterns involved dialogue between the RNs and the patients, as well as direct questions from the RNs to identify the patients’ problems and care needs during home visits. Communication patterns in nursing play a crucial role in the delivery of quality care. 35 Earlier research showed that RNs’ communication skills are crucial in involving older patients in their care in healthcare settings. 36 Another study emphasized the importance of communication that addresses the need for trust, predictability, and responsiveness to patients’ existential needs. 15 Kuluski et al. 37 showed that older patients value being heard and appreciated and feeling comfortable; this emphasizes that improved communication and increased patient participation can give patients the confidence to share their problems, which, in turn, requires healthcare personnel to listen when patients share. 38
Studies have highlighted the connection between ‘knowing the patient’ and good communication between RNs and patients. 39 In our study, RNs’ knowledge of the patients appeared to be ‘locked’ into a specific perception of the patients’ condition in some cases (cases 1, 4, and 5). This suggests that knowing the patient does not necessarily lead to effective communication about the patient's problems.
RNs’ and patients’ agreements and disagreements regarding perceptions and prioritization of the patients’ problems and need for help with the problems
Agreements
Both RNs and patients reported patient problems related to breathing and circulation (such as heavy breathing and coughing) as two of the three main patient problems in all cases. COPD's primary effects on breathing and circulation, which affect various aspects of patients’ lives as issues connected to activity, are well known both through RNs’ professional knowledge and patients’ knowledge and experience of the disease. 40 In this study, these problems and the need for help with them occupied varying positions within the major three ranks, as reported by both patients and RNs. This indicates that the degree of breathing/circulation issues has various implications for patients’ daily lives.
Disagreements
Across the mapping forms, the largest discrepancy between the perceptions of the RNs and patients was found in relation to psychosocial, activity, and communication problems. Breathlessness, a common symptom of COPD, engenders feelings of fear and anxiety. 40 Challenges related to psychosocial problems in patients diagnosed with COPD are well-documented. 41 In line with these studies, our research reflects these problems and highlights the potential neglect of patients’ psychosocial issues. Although RNs in this study observed the mood and expressions of patients and sensed the atmosphere surrounding them, they did not directly inquire about patients’ psychosocial problems or follow up on their invitations to discuss their concerns. This finding aligns with an earlier study on older patients’ expressions of emotional cues during home healthcare visits, which revealed that needs were only implicitly communicated. 42 In case 1, the RN did not pursue the patient's invitations to discuss her psychosocial challenges, which could be an indication of the RN's familiarity with the patient. The RN may also have recognized that this type of conversation requires a significant amount of time, which might not have been available. 43 These variations may correlate with home care RNs who exhibit a more task-focused or clinically focused approach in the context of the patient's allocated home healthcare. 44
In case 4, where the patient was in an exceptionally good mood, the RN did not ask the patient about psychosocial challenges. The patient's psychosocial challenges were not visible and therefore not questioned. This is noteworthy in view of claims that home care communication involves more socio-emotional communication rather than task-oriented communication between older patients and RNs. 45 This insight may underscore the need for tailored communication strategies and a patient-centered approach to care in the context of home care.
Overall, our study reveals shortcomings in home care visits regarding communication with the patient about their psychological challenges in daily life. This could also indicate that psychosocial problems are less apparent than somatic problems, making them difficult to express and address during home care visits despite the RNs’ familiarity with their patients. It is important for patients to feel comfortable sharing their problems even if they are related to psychosocial factors.
Mobility is a well-known challenge for patients with COPD. 40 In addition, COPD is known to cause discomfort and limitations in relation to activities in daily life. 46 In this study, both the patients and the RNs reported the patients’ problems with activity as one of the patients’ most serious challenges. However, the findings showed a difference in scores between the RNs’ and patients’ reports, which may be individual. In case 1, the RN gave higher scores for activity in relation to both the patient's problem and care needs. On the other hand, in case 2, the patient reported both a greater problem and a greater need for care in relation to activity. The RNs observed the patients’ limitations, as well as what they could do, by observing the patient and their context. The patients were asked about activity-related issues, but more specific questions about activities were not posed.
Regarding the patients’ problems with communication, such as hearing difficulties, the results revealed a discrepancy between the reports of RNs and patients. The RNs did not report problems or acknowledge the need for care in relation to the patients’ reported communication difficulties. In this study, the patients’ communication problems were specifically linked to sight or hearing problems. It is reasonable to assume that these problems were not considered significant by the RNs as the patients were using hearing aids and/or glasses to address them. However, these communication challenges were not effectively communicated or addressed during the home visits.
Communication between RNs and patients affects the perception of the patients’ problems and need for help
This study highlights a lack of communication during home visits regarding some patients’ problems and reveals potential contributing factors. It also identifies instances of missed communication and barriers hindering the visibility of patients’ problems, especially psychosocial ones. Importantly, the findings suggest that knowing the patients does not always lead to a better understanding of their challenges. Our study emphasizes the importance of effective communication and the significance of asking the right question in the right way, given that person-centered conversations often have different underlying perspectives and should therefore concentrate on perspective. 47 Asking the right questions in the right way in communication can therefore be considered in relation to having an understanding of the related underlying perspective in person-centered communication. This accentuates the importance of communication as a dialogue with perspective in nursing practice and highlights its use as a means to engage in equal participation with patients to identify their problems and address their care needs.
It is possible that certain questions are not being asked appropriately or that the questions asked are not conducive to open communication. In addition, our findings may reflect a culture or tradition wherein patient participation is not emphasized. Patient participation in nursing means involving the patients in their care and listening to their problems, which provides valuable guidance for nursing. 38
Our findings could also be an indicator of health literacy and/or cultural factors affecting the patients’ ability to communicate their problems and challenges, making it difficult to articulate their problems and needs. A study conducted in a hospital setting demonstrated that targeted health literacy interventions for individuals with COPD led to improved communication and understanding of health information. 48
The World Health Organization 49 emphasizes investments in health literacy and empowerment so that patients have the necessary knowledge to communicate their health needs and challenges.
In addition, our findings indicate that patients may respond individually to the descriptions of their problems and care needs. It is also plausible that patients may exhibit behaviors to avoid disclosing their problems if the nurse does not ask the right questions, as shown in case 4. 50
Conclusions and implications
Older patients with COPD receiving home healthcare often have multiple and complex health problems. RNs must have a clear understanding of these problems to provide appropriate care. Differences in the perceptions of patients’ problems and care needs between RNs and patients can influence patient care. Deficient communication between RNs and patients can also jeopardize patient safety. In addition, this study sheds light on the importance of patients being knowledgeable about the implications of COPD.
Communication that results in a lack of perception of patients’ problems can potentially jeopardize patient safety. Therefore, we advocate improvements in how RNs communicate with patients, particularly when addressing mental health issues. It may be necessary to develop guidelines or provide training courses to better address patients’ psychosocial problems. In addition, following up with patients through questionnaires could be beneficial. The available references indicate a lack of specific documentation addressing disagreements between RNs and patients with COPD in reporting problems during home visits. Further research focusing on these disagreements is crucial to bridge the gap between RNs’ and patients’ perceptions of problems and care needs, particularly regarding patients’ psychosocial issues.
Strengths and limitations
The purpose of case studies is not to generalize, but to generate knowledge about unique conditions and experiences in specific contexts. 23 Although the number of cases is small, this study has triangulated methods, employing both qualitative and quantitative approaches to obtain nuanced and detailed insights, 51 which are further reflected in the analysis and illuminated by theory and previous research. 52 This allows us to see the microscopic as macroscopic and enables knowledge to be transferred to larger contexts. 53 To ensure trustworthiness, we have striven for a clear description of the context and transparent renderings of recruitment, data collection, and analysis. 54 The findings are presented exemplified with quotes and records made by patients and nurses. Adherence to the COREQ checklist 24 also ensured transparent reporting, enhancing the credibility and trustworthiness of the study findings.
We consider it a strength of our study that both patients’ and RNs’ perceptions were examined during the same home visits. However, it is important to acknowledge that the presence of the researcher during the home care visits may have influenced RN–patient communication, particularly regarding the patients’ psychosocial problems, because of ethical considerations. To address this potential influence, follow-up questions were asked of the RNs during the interviews after the home visits. Concerning the mapping forms, the participants were given the same questions based on the VIPS keywords, which strengthened the stability of the responses.
The first author was responsible for data collection, but all authors actively participated in the data analysis and article-writing process as an ongoing collaboration, with regular discussions throughout the research process, which constitutes a strength of the work.
The authors’ existing understanding and experience in geriatric nursing in both hospital and community care can be considered both a strength and a limitation. The interpretation process can be seen as both promoted and hindered by the authors’ preconceptions.
Footnotes
Acknowledgments
The authors would like to thank the participants for their kind contributions.
Author contributions
Study design: RØ, SAD, IE, and RMO. Data collection: RØ. Data analysis: RØ, SAD, IE, and RMO. Manuscript preparation: RØ, SAD, IE, and RMO. Critical review of the manuscript: RØ, SAD, IE, and RMO. All authors approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Nord Universitet.