
Abstract
Advance Care Planning can be used to engage people with dementia in decision-making about future care. The current study aims to advance the state of knowledge about Advance Care Planning interventions aimed at older people with early-stage dementia and to describe the effects of various interventions as well as the feedback on the interventions from this patient group and their family caregivers. The study is reported in accordance with PRISMA for scoping reviews. The search for studies and reports included electronic databases, websites, books, and reference lists. Data from the selected studies, including publication year, title, purpose, study population, intervention, methods, and results, were extracted. Six full-text articles were identified as suitable for inclusion. The six interventions had differing approaches. A supportive structure was helpful for both people with dementia and family caregivers. The feeling of being listened to and engaged in the care planning seems to be of most importance, not the intervention design itself.
Introduction
Different types of dementia belong to the most challenging issues in current healthcare. A dementia diagnosis is associated with impaired functional abilities, reduced quality of life, psychosocial distress, and social isolation. The number of people with an Alzheimer’s disease diagnosis is estimated to reach close to 110 million in the year 2050. In the absence of prevention strategies and therapeutic interventions, an estimated one in 85 people will be living with Alzheimer’s.1–4 Advance Care Planning (ACP) can be used to engage people with dementia and their family members in decision-making about future care.5,6 In 2017, a large, multidisciplinary Delphi panel of ACP experts reached a consensus on an extended definition and a brief definition of ACP.
6
The brief definition is as follows: Advance care planning enables individuals to define goals and preferences for future medical treatment and care, to discuss these goals and preferences with family and healthcare providers, and to record and review these preferences if appropriate.
6
ACP for people with dementia has received attention in recent years. There are a number of recent studies highlighting barriers and facilitators as well as evaluating efficacy of ACP in dementia care and subsequent effects on end-of-life care. Most of these studies explore issues pertaining to the advanced stage of dementia and/or long-term care settings.6,22,25–30 The field of research in ACP in early-stage dementia is less developed. According to van der Steen et al., 31 the community setting as well as patients’ and nurses’ perspectives are understudied. The need to determine the most relevant outcome measures for evaluating ACP is urgent6,32 and even more so when it comes to ACP for people with dementia.
This study is the first in a PhD project with the aim to develop an ACP model for older people in the early phase of dementia and their family caregivers. The purpose of this study is to advance the state of knowledge about ACP interventions aimed at older people with early-stage dementia, and to describe the effects of various interventions as well as the feedback on the interventions from this patient group and their family caregivers. The research questions are: what type of ACP interventions have been developed for people with early-stage dementia? How have people in the early stage of dementia and their family caregivers perceived and been affected by the interventions?
Design
The method used for the study is scoping review as first described by Arksey and O’Malley 33 and further advanced by Levac, Colquhoun and O’Brien 34 as well as by Peters et al. 35 As ACP program evaluation reports were expected to provide part of the data material for the current study, a scoping review was determined to be the most relevant study method.
Identifying relevant studies
In order to identify relevant studies and reports describing ACP interventions for people with dementia, a literature search was conducted and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) guidelines 36 (supplementary file 1, available online). The following electronic databases were searched: EBSCO (Academic Search Premier), CINAHL, PubMed, SAGE Journals, and FINNA. FINNA is a search service entity providing access to material from Finnish libraries, archives and museums. 37 The search words used were ‘advance care planning dementia’, ‘complex advance care planning’, ‘advance care planning AND early dementia’, ‘advance care planning AND community setting’, ‘advance care planning intervention AND early dementia’. The search words ‘complex advance care planning’ refer to the difference between Advance Directives which can be seen as more straightforward and ‘simple’, while ACP is seen as a more complex and meaningful process.8,38 National ACP program names were also used as search words in combination with ‘dementia’ and ‘intervention’. The search started with a wide perspective in order to gain a broad picture of the field of ACP studies related to dementia care. The search was narrowed with the search words ‘early dementia’ AND ‘intervention’. The reference lists of full-text articles on ACP, ACP program reports, and book chapters were searched manually.
Study selection
In order to be included, papers and reports had to be in English and had to describe ACP interventions aimed at older people with dementia in a community setting. The study focused on older people with dementia as prevalence increases with age 39 and young-onset dementia presents different challenges. 40 The studies had to include feedback on the intervention from the people with dementia themselves. The papers had to have been published between January 2006 and June 2019. Studies in a non-Western context and studies focusing on specific ethnic groups were excluded. Studies focusing on Advance Directives only were also excluded. The wide perspective search of the electronic databases retrieved 4799 records after duplicates were removed. The titles of the records identified were screened by the first author for perceived relevance to the focus of the study. Three hundred and five abstracts were reviewed and evaluated independently by two of the authors. Seventy full-text articles and abstracts were assessed for inclusion in the review. In cases of ambiguity, all authors assessed the articles for inclusion to ensure ethical credibility. In the end, six eligible studies were identified as describing ACP interventions for early-stage dementia patients from the person with dementia’s point of view and thus were included. A flow chart describing the process is included in Figure 1.
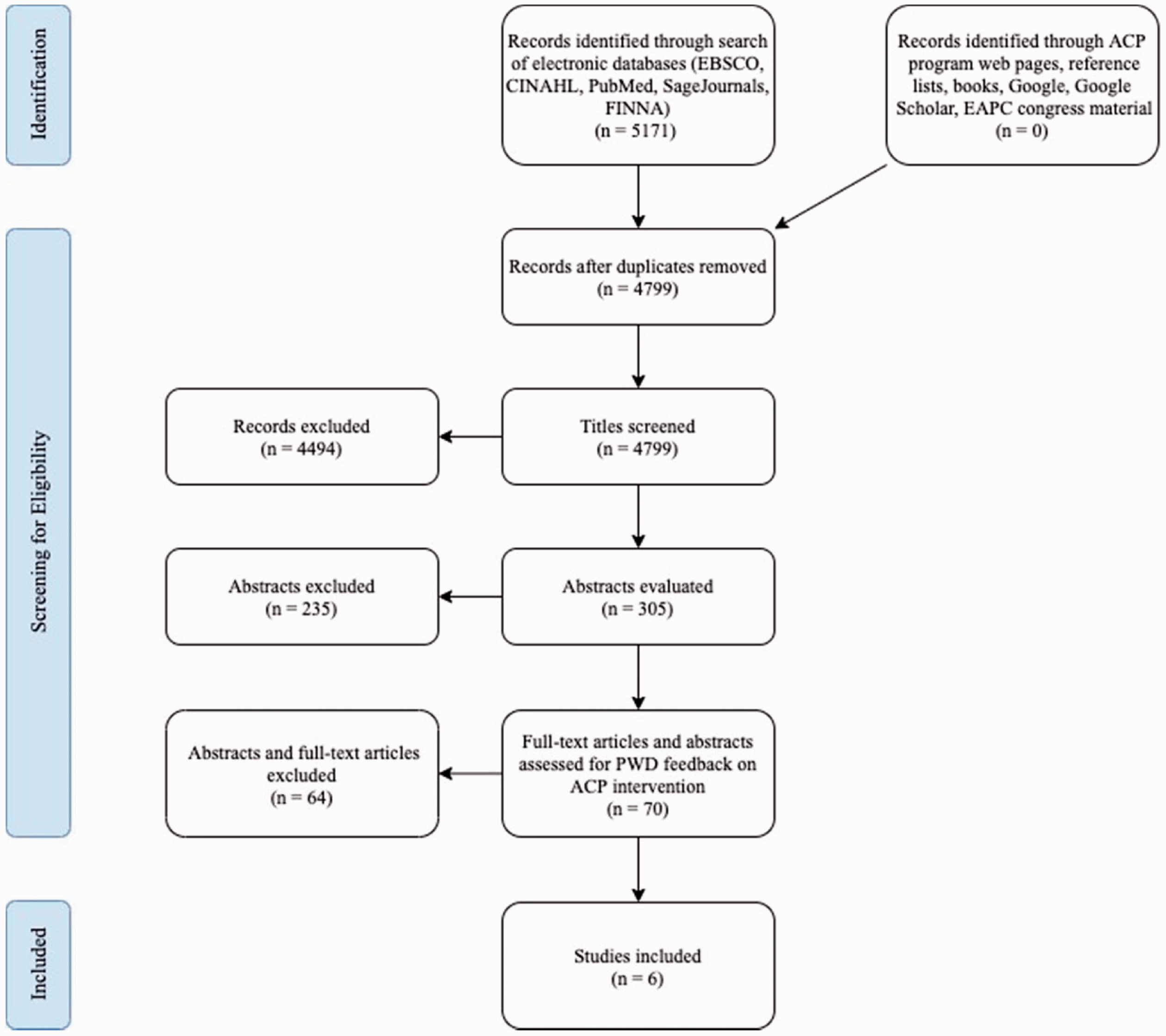
Flow chart of the study selection.
Charting the data and extracting the results
The full-text articles identified as suitable for inclusion in the scoping review (n = 6) were reviewed by all authors to ensure ethical credibility. Data including publication year, title, purpose, study population, intervention, methods, and results were charted and extracted (supplementary file 2, available online). After data charting and extraction, the data were summarized to provide answers to the research questions.33,35 In this review, external stakeholders were not involved in the data search, data extraction, nor in the publication process.
Ethical considerations
This scoping review is the first sub-study in a PhD research project with the aim to develop an ACP model for older people in the early phase of dementia and their family caregivers. The PhD research project has been approved by the ethical committee of Åbo Akademi University University. Ethical approval was not required for the scoping review.
Results
In the search for studies and reports describing ACP interventions for people with early-stage dementia, six scientific studies41–46 were found (supplementary file 2). The six studies focused on the ACP intervention, the results of the intervention, and included feedback from the people with dementia on the ACP process. Despite the low number of studies identified, the studies describe a relatively wide range of intervention types.
In-home sessions with trained facilitators
Three of the ACP interventions for people with early-stage dementia included in-home sessions with facilitators, such as experienced research assistants trained to complete the assessments 41 and trained counselors with dementia expertise.43,46
The Preserving Identity and Planning for Advance Care (PIPAC) intervention 41 implemented a two-group comparison design using blocked randomization stratified by gender and race to assign 19 dyads to either a multicomponent intervention group using trained interventionists or a minimal support phone contact comparison group. The dyads consisted of a person with mild dementia and a family contact. The PIPAC intervention focused on the identity of the person with dementia by combining identity-maintaining activities with an ACP discussion. The intervention consisted of four in-home sessions over 4–6 weeks. Trained interventionists combined one future planning component, one reminiscence-based component, and the Cohen-Mansfield Identity Interview. The aim was to enhance well-being and quality of life and to maximize coping in the early phase of dementia. 41 Acceptability and feasibility data were collected through a variety of methods, including a treatment implementation documentation and a program satisfaction measure. Hilgeman et al. 41 used validated instruments to assess quality of life, meaning in life, emotional support and connectedness, health-related quality of life, perceptions of uncertainty in choosing future medical care, and symptoms such as depression and anxiety.
In the Early Diagnosis Dyadic Intervention (EDDI), Whitlatch et al. 46 used trained counselors with dementia expertise to lead sessions in a feasibility trial. Thirty-one dyads participated in the study. The EDDI focused on viewing both members of the dyad as partners. The intervention consisted of nine sessions performed both jointly and one-on-one with care receivers and family caregivers. The aim of the sessions was to help participants express preferences and concerns and to strengthen the relationship bond. Intervention tools and materials such as notebooks, worksheets, diagrams, and magnetic manipulations boards were designed and used during the sessions. Data were collected through the completion of evaluation forms after each season.
For the Support, Health, Activities, Resources, and Education (SHARE) intervention, 43 extensively trained counselors were used to implement and evaluate a counseling-based care planning intervention for 40 early-stage dementia care dyads. The intervention focused on empowerment and self-efficacy. The intervention consisted of seven structured sessions where care values and preferences were assessed, specific material covered, and a care plan developed. The SHARE approach focused on self-efficacy and empowerment for both the person with dementia and the family caregiver. Person with dementia and family caregiver comments were analyzed and themes coded. Baseline data from the Care Preference Scale were compared to the post-intervention data. 43 It should be noted that the SHARE intervention 43 is a more recent and re-named version of the EDDI, 46 both of which have been included in this study. During the EDDI study, it was noted that some of the original domain names and tools were too challenging and required simplification. An overlap of material led to a reduction in the number of sessions from nine to seven. Since few dyads completed the homework between sessions, the homework was eliminated. In addition, a pre-session was added in order to gather information and assess appropriateness. 46
Patient choices in a clinical setting
The remaining three interventions all had differing approaches conducted in clinical settings. Lewis et al. 42 introduced ACP to people with recently diagnosed dementia or mild cognitive impairment in a three-stage project over a period of eight months through a specialist memory clinic. The intervention was based on the Respecting Patient Choices program, which incorporates appointment of enduring powers of attorney, refusal of treatment certificates, and statement of choices used to guide future treatment. 47 Specialist memory clinic clients received a survey in the mail. The survey assessed completed documentation for future care, the understanding of ACP, and interest in further information about ACP. Those participants who were interested in further information were invited to a seminar and provided feedback afterwards. Seminar participants were then invited to complete ACP documentation together with an ACP clinician. Participants in this third stage provided an evaluation of the stage. The initial survey was mailed to 97 clients and 92 carers. In the third and final stage, three clients and two carers remained to complete ACP documentation. 42
Poppe et al., 44 in turn created a structured ACP tool in order to structure and facilitate the discussion at two memory services. A theoretical model or framework underpinning the ACP tool was not mentioned. The tool included questions such as ‘What would you like to know about your care and treatment, how much information do you normally like to have? Are you the sort of person that likes to have all of the information, or would you prefer not to know too much?’ People with dementia were identified through two memory services, either from the case load of cases or during the diagnostic assessment. Post-intervention data were collected through in-depth interviews with 12 people with dementia, eight family caregivers, and six care staff members. The interviews were qualitatively analyzed through the constant comparison method. 44
Lastly, Volandes et al. 45 used a video decision support tool in four primary care clinics (two adult medicine and two geriatric). The effects of the tool were evaluated on preferences for future medical care if advanced dementia were to develop. In the study, a theoretical model or framework underpinning the ACP tool was not mentioned. Participants were recruited during clinic visits that were part of their usual care. In the randomized controlled trial, a group of 94 people received a verbal description of advanced dementia while the other group of 106 people viewed a two-minute long video depicting a patient with advanced dementia in a nursing home setting. In the group receiving a verbal description, 12 people (11%) had a dementia diagnosis. The video description group had six people (6%) with a dementia diagnosis. The study was included despite not all participants being people with dementia as the number of people with dementia participating was relatively large as compared to the number of participants in the other included studies. The study did not mention a difference in response between people with dementia and people with no dementia diagnosis. Before and after the intervention, data were collected through structured questionnaires where participants chose between options for preferences for goals of care. 45
Post-intervention effects: Participant perspective
Almost all family caregivers and people with dementia felt comfortable discussing with their dyad partner, which indicates that a supportive structure is helpful when having difficult discussions with each other.43,44 Overall, there were no significant differences between post-intervention effects reported by people with dementia and family caregivers. However, the importance of staff style and skill was especially noted by family caregivers.43,46 Both people with dementia and family caregivers suggested that properly trained staff could advise on the right time in the dementia progression to begin the ACP intervention and to initiate the ACP discussions as well. 44
The post-intervention effects reported by people with dementia included fewer depressive symptoms, increased quality of life (on the Bath Assessment of Subjective Quality of Life in Dementia measure), less overall conflict or discomfort with ACP, as well as feeling more supported in decision-making and having more coping strategies. Family caregivers also experienced fewer symptoms of depression. 41 Other effects included opportunity to express thoughts and feelings and overall satisfaction with having completed the full intervention.42–44,46 The ACP intervention affected family dynamics in that some person with dementia–caregiver dyads experienced an improved relationship and overall relief from having discussed the future.42–44 Post-intervention family caregivers felt more confident that the necessary future decisions made would reflect the patient’s wishes. 44 The majority of person with dementia–family caregiver dyads felt better prepared for the future, more confident about decision-making, and felt more in control of the situation. 43 In the study evaluating the video support tool, patients who viewed the video were more likely to choose a comfort-oriented approach compared to patients in the control group who received a verbal description instead. The choices of the group using the video decision support tool were also found to be more stable over time. 45
Only one of the studies 41 reported a number of neutral effects post intervention; the intervention did not appear to affect self-reported anxiety, social engagement, meaning, anticipated and emotional support, and quality of life as measured by the Quality of Life in Alzheimer’s Disease scale. Negative effects on well-being post intervention were reported in one study 44 and included feeling dispirited and finding the topic difficult to discuss. In the six studies included in this review, most respondents (people with dementia and family caregivers) indicated satisfaction with the interventions used. The feeling of being listened to and engaged in the care planning seems to be of most importance, not the intervention design itself. The effects of the ACP intervention as well as the factors associated with a positive or negative intervention impact provide a structure for the optimal ACP discussion.
Evaluation of interventions
In the intervention structure, attention has been given to the number of sessions, session length, session structure, as well as to the material provided and topics discussed. Several different types of interventions were tested in the included studies: seminars, in-depth interviews, counselor sessions, and a video decision support tool.41–46 A structured design was found to help ground the care dyad to the present, thus enabling a future case discussion in a supportive and safe way. 43
In five of the six studies, a family caregiver had been included, and the intervention was performed in a person with dementia–family caregiver dyad.41–44,46 Two of the studies included feedback from care staff in the form of nurses 30 and session counselors 46 in addition to the feedback from the person with dementia–family caregiver dyad. One of the studies was qualitative, using in-depth interviews to evaluate the intervention 44 while the other studies used both quantitative and qualitative methods to evaluate the interventions. Only one of the studies used a randomized controlled trial (RCT) design. 45 The sample sizes were also relatively small, from 18 people with dementia in the RCT study 45 to 80 people with dementia and family caregivers (40 dyads) in the Orsulic-Jeras et al. 43 study.
Discussion
People with diminishing cognition is a group seldom heard and engaged in the research process. 48 In dementia care, an approach that incorporates a human-centered design 49 with an understanding of the challenges faced by patients and care staff is important to improve quality of care and vital to the development of ACP interventions for people with dementia and their family caregivers. In this scoping review, six studies describing ACP interventions for early-stage dementia patients have been charted and summarized. The studies describe a relatively wide range of intervention types such as counselor sessions,43,46 seminars, 42 and video images, 45 among others. The majority of the respondents (people with dementia and family caregivers) indicated satisfaction with the interventions used. This satisfaction can be seen in how the ACP interventions affected participants in mostly positive ways. People with dementia and family caregivers indicated satisfaction with the type of intervention used despite the significant differences between the interventions tested in the included studies.
When describing lessons learned from a pilot study of the patient-centered ACP interview, Briggs 50 states that ‘listening is the intervention’. The person with dementia-family caregiver dyads experienced relief from having discussed the future as well as an improved relationship.42–44 One of the ACP interventions explored the concept of family caregiver burden and ways of reducing that burden in a meaningful way. 43 Family caregivers felt increased confidence about decision-making and felt better prepared for the future.43,44 On the other hand, some of the people with dementia found the ACP discussion disheartening and some felt that it was difficult to discuss the future without knowing what the future will bring. 44
Several studies have highlighted barriers to end-of-life care planning. Dening, Jones and Sampson 19 and Jones et al. 18 found that successful participation in an ACP intervention is affected by the ability of the person with dementia to consider their future and how life may change as the illness progresses. People with dementia may experience trouble when considering their future selves and make assumptions about retained independence. People are also reluctant to think about their own death or the death of loved ones. 51 Hirschman, Kapo and Karlawish 26 identified remediable barriers to ACP discussions, including not knowing what to talk about, when to talk, and waiting until it was too late.
These factors of the care dyad and future care discussion begin to paint a picture of the optimal ACP structure. Findings show that dyads that are able to work together are able to create a preliminary care plan that is based on the care values of the person with dementia, and is balanced and realistic. 43 The person with dementia may be able and willing to talk about future care with their family caregiver, but these talks do not always take place.26,43,44 Dickinson et al. 22 noted that life-long conversations led to a confidence in unspoken knowledge to help inform future decision-making. However, according to research, family caregivers may lack full comprehension of what people with dementia see as important and how it relates to care.43,52
The optimal structure for discussions of future care has been seen as the person with dementia–family caregiver dyad working as a team, supported by the work of e.g. Wilson, 53 Kitwood, 54 and Keady and Nolan. 55 Harrison Dening 9 suggests that, in dementia care, a person-centered approach is not enough as it may cause conflict with the perspectives and preferences of a family caregiver and vice versa. Harrison Dening 9 goes on to suggest that a relationship-centered approach may be more appropriate. In a relationship-centered approach, the whole family may be included. Nolan et al. 56 suggest a relationship-centered dementia care model where the nurse works together with the person with dementia and the family caregiver in a triad, in order to promote senses of belonging, security, continuity, purpose, achievement, and significance. A relationship-centered ACP intervention is also supported by the results of the Advanced Care Planning in Early Dementia (ACP-ED) intervention study by Poppe et al. 44
Research has looked into various tools to be used in ACP in order to assist facilitators in achieving the optimal ACP structure. In their report, Butler et al. 57 describe ACP decision aids as supportive of certain key components of the process, such as learning about what to expect, care options, reflecting on care options, and communicating preferences for future care. Butler et al. 57 call for easily accessible, understandable, readable tools appropriate for patients working across various settings and with various facilitators. Volandes et al. 45 conducted ACP research with the help of video images; a tool often conveying more understanding than a text describing the same phenomena. In the study which evaluated the video support tool, patients who viewed the video were more likely to choose a comfort-oriented approach compared to patients in the control group who received a verbal description instead. The participants also indicated that the video support tool was highly acceptable. 45
There are several ethical challenges in in the ACP process for people with early-stage dementia. In March 2015, during the First WHO Ministerial Conference on Global Action Against Dementia, the importance of paying attention to people with dementia from a human rights perspective was emphasized. The dignity, needs, and wishes of people with dementia are to be respected in all phases of the illness. 58 One of the ethical challenges is overcoming the traditionally paternalistic attitudes of healthcare workers. Community expectations for increased community care and improved palliative care for patients with chronic conditions have grown, leading to shifts in general ethical principles underlying healthcare decision-making. There is an increased respect for patient autonomy when it comes to making decisions about medical treatment and healthcare. 59 However, Gastmans 23 argues for an approach that goes beyond the principles of autonomy, nonmaleficence, beneficence, and justice, principles that are dominant model in medical ethics. Gastmans 23 introduces a dignity-enhancing ethical framework where the vulnerability of people with dementia is seen as an extraordinary vulnerability, requiring carers to have the ethical attitudes of responsibility and competency.
Studies indicate that nurses and nurse practitioners are well positioned to initiate and lead ACP discussions as well as suited to participate in the development of ACP processes and models. In two of the studies included in this scoping review, it was suggested that outpatient memory clinics with properly trained and resourced staff were suitable for the initiation of ACP discussions.42,44 However, the role of nurses and nurse practitioners was not explicated. In a scoping review of experiences of ACP for people with dementia conducted by Jones et al., 18 it was found that community nurses and palliative care specialists had the most experience of discussing and developing ACP and were therefore the most confident in initiating ACP. Yeun-Sim Jeong, Higgins and McMillan 60 highlight the role of the nurse in ACP when describing the clinical nurse consultant role as a broker who acts as an intermediary in decision-making (between family and doctors), collects information, initiates interventions, educates clients and peers, and acts as client advocate. Cotter et al., 14 in turn, state that nurse practitioners have a responsibility to facilitate the ACP discussion with people in the early phase of dementia. However, a recent systematic review by Blackwood et al. 61 found that there is a need for increased focus on the training and education required for both nurses and other healthcare staff for ACP to become a routine part of clinical practice.
A challenge in dementia care is the lack of continuity in the contact with care professionals. As the dementia progresses and the care needs of the person with dementia increases, the place of care changes from outpatient memory clinics to assisted-living facilities and nursing homes. In this type of dementia care structure, the person with dementia and his/her family caregiver will encounter many nurses and doctors along the illness trajectory who are not necessarily familiar with the person with dementia and his/her family and their care preferences and wishes for end-of-life care. A focus on the re-structuring of dementia care to ensure care contact continuity is essential.
In summary, initiatives to develop a standardized, semi-structured, and simple tool for systematic ACP discussions with this patient group and their family caregivers are required. Furthermore, the professional group responsible for these discussions should be explicated. The number of studies identified that have included feedback from people with dementia was low. This indicates the need for further studies that include people with dementia in the early phase of the illness trajectory. The gaps also include a lack of validated tools to evaluate ACP intervention feasibility and acceptability from the perspective of the people with dementia themselves. Studies that focus on outcome and process evaluations are equally essential; however, there is a lack of validated evaluation tools. Examples of ACP outcome evaluation studies include a randomized controlled trial where Detering et al. 62 investigated the impact of ACP on end-of-life care in legally competent elderly patients. The primary outcome measure was whether the patient’s end-of-life wishes were known and respected. Other outcome evaluations such as monitoring emergency admissions to hospital after ACP in a nursing home setting have been conducted as well. 63 Klingler et al. 64 studied the cost implications of ACP and the associated ethical conflicts. In dementia care, ACP outcome evaluations which focus on the satisfaction of the family caregiver should be emphasized as the person with end-stage dementia is no longer able to communicate his or her satisfaction with the care.
The current study’s strengths are the description of ACP interventions aimed at older people with early-stage dementia as well as its focus on the experience of the person with dementia and, in extension, his/her family caregiver. The number of included studies was low due to the stringent inclusion criteria, which limited the studies to those where the feedback from the people with dementia themselves was reported. The studies were also limited to English-speaking, Western countries. The number of participants in the identified studies was low as most were qualitative studies. Pilot interventions were tested and evaluated. Only one of the studies had a randomized controlled trial design, 45 while another had a two-group comparison design. 41
Conclusion
There is a general consensus that ACP in dementia care can be a valuable way to alleviate suffering for both people with dementia and family caregivers. ACP for dementia patients provides an opportunity for relationship-centered triad care that includes the person with dementia, the family caregiver, and professional care staff. Staff competence is of great significance in ACP for all patient groups; even more so in dementia care where the diminishing cognition, reduced decision capacity, and extraordinary vulnerability associated with the illness provide significant ethical challenges. The ACP process should be organized as a continuous collaboration between care professionals, people with dementia and their family caregiver. The ethical challenges, the complexity of ACP program or intervention implementations in early-stage dementia care, and the development of process and outcome evaluation measures need further study. The results of the scoping review provide a starting point for healthcare organizations, such as memory clinics, to develop a structure for ACP discussions with people with dementia and their family caregivers.
Supplemental Material
sj-pdf-1-njn-10.1177_20571585211014005 - Supplemental material for Advance Care Planning interventions for older people with early-stage dementia: A scoping review
Supplemental material, sj-pdf-1-njn-10.1177_20571585211014005 for Advance Care Planning interventions for older people with early-stage dementia: A scoping review by Annika Tetrault, Maj-Helen Nyback, Heli Vaartio-Rajalin and Lisbeth Fagerström in Nordic Journal of Nursing Research
Footnotes
Acknowledgements
The authors would like to thank Nadia Tetrault for English language checking and academic proofreading.
Author contribution
All authors, Annika Tetrault, Maj-Helen Nyback, Heli Vaartio-Rajalin, and Lisbeth Fagerström meet the criteria for authorship. All authors contributed to the conception and the design of the study, acquisition of data, and the selection of studies. All authors participated in the review of data, analysis and interpretation of data, and critical reading and revision of the article. Annika Tetrault wrote the first draft of the manuscript. All authors have read and approved the final manuscript.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by a general PhD student grant (1 year) from Åbo Akademi University and by a stipend from the Finnish Nurses Association. The sponsors had no role in conducting the research and no involvement in decision-making regarding article submission.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.