
Abstract
Background
Digital health technologies (DHTs) promise enhanced health for older people, yet the digital divide hinders adoption and utilization. This study aimed to identify DHTs that can help older people in chronic disease management, specifically the facilitators, barriers, needs, and scenarios.
Methods
We searched PubMed, Embase, Cochrane Library, Web of Science, Scopus, and IEEE for studies published in English between 2000 and 2024. Analysis of included articles included descriptive synthesis and thematic analysis.
Results
Forty-seven studies were included, yielding 148 DHTs classified as Medical services and support (n = 94) or Self-management (n = 54). Experience of Use and Interpersonal Support were the main facilitators of the use of DHTs. Awareness of Competence, Technological Factors, Sense of Security, and Individual Factors are barriers. Needs can be categorized into Service Functions and Subjective Needs, and the main scenarios include Home, Community, and Hospital.
Conclusions
Digital health technologies are widely used, especially in developed countries, but challenges remain in developing countries and among specific patient. Future studies should focus on addressing concerns about DHT availability, security, and reliability in older people, actively incorporating feedback, providing personalized service, and fully mobilizing positive social factors to promote DHTs.
Introduction
Population aging has become an important challenge shared by the whole world, with developed countries entering into heavily aging societies, developing countries experiencing a demographic transition to low fertility and low mortality.1,2 Chronic noncommunicable diseases pose a serious threat to human life and health. 3 Health care for older people with chronic diseases is no longer a single individual's behavior but requires the concerted efforts of the entire society. 4 The rapid development of information technology has continuously revolutionized and driven the traditional chronic disease care model to a new stage of digital health, enriching the chronic disease management model.5–7 In personal health management, DHTs (digital health technologies) are even more valuable for older people with chronic diseases. 7
Countries around the world are focusing on the strategic layout and innovative practices in the field of digital health, promoting the in-depth integration of technology, products and operations, and digital health in the field of elderly chronic disease has been deeply explored and researched.8,9 One review compiled information concerning the development of DHTs and categorized them as five big PHC functions, but lacked details about the distribution characteristics of DHTs. 10 Obviously, many studies have highly affirmed the prospect of DHTs which is considered to have a significant value in improving the health of the elderly.11–13
However, the digital divide is becoming more pronounced among older adults with chronic diseases. Due to their physical weakness, language barriers, financial challenges, and low educational background, it is becoming more difficult for older adults to adopt and use DHTs, and the risk of digital divide is increasing.14,15 Good digital health literacy can lead to better acceptance and use of DHTs among older adults, lack of digital health literacy often leads to a higher likelihood of developing chronic health conditions. 16 Shin found that digitally stored health data and information creates a validity bias in the public perception of digital health, and that patients who have difficulty applying them will have difficulty meeting their health needs. 17 Older people with chronic diseases who actively participate in health resource sharing through DHTs are able to sustainably improve their emotional fulfillment and self-efficacy, which further strengthens their social interactions and healthiness of life. 18
Many studies have shown that the utilization and frequency of mHealth technology is not high, and there are significant challenges to the acceptance of DHTs, especially among the older age groups. 19 Widespread use of new technologies cannot be separated from the in-depth research on the factors influencing individuals’ adoption of new technologies. However, we found that the majority of reviews on similar topics focus on the effectiveness of DHTs for older adults, such as feasibility, cost, adherence, and health outcomes.12,20,21 Some studies focuses on the opportunities and challenges of using mobile health in elderly self-care, but the scope of the population is too broad, and the type of DHTs is relatively simple, conclusions don’t have good representativeness for elderly people with chronic diseases, who are particularly vulnerable and need care.22,23 This further proves the importance of our research, we provides valuable insights into the adoption of DHTs among older people with chronic diseases.
This study aims to evaluate recent literature, with a focus on the current use of DHTs in older people with chronic diseases, particularly the relevant influencing factors (facilitators, barriers, needs, scenarios). Through this assessment, the study aims to propose support strategies to improve their services in a targeted manner and propel progress in this critical domain of health care.
Methods
Search strategy
The protocol for this review can be accessed at the Open Science Framework. 24 We strictly followed the guidelines of Preferred Reporting Items for Literature Review and Meta-Analyses 25 (see Appendix A for the PRISMA Checklist).
Our review was conducted in six databases: PubMed, Embase, Cochrane Library, Web of Science, Scopus, and IEEE, with a publication period from January 1, 2000, to December 1, 2024. Search strategy was developed by two professional researchers (CL and LZ) with the help of librarians, mainly based on three selected keywords: “Digital Technology,” “Chronic Diseases,” AND “Elderly.” We didn’t distinguish whether elderly suffer from a single or multiple chronic diseases, and strictly followed the International Classification of Diseases to classify chronic diseases, which improved the clarity of the review. 26 The query searched the title and abstract fields. All search fields were searched for the of IEEE Explore database because limiting the search fields to the titles and abstracts would result in no articles. The complete search strategy is provided in Appendix B.
Eligibility criteria
All literature was managed using NoteExpress software, two professional researchers (CL and HW) independently completed an initial literature screening according to inclusion and exclusion criteria (see Textbox 1), a third senior researcher (AO) made a comprehensive determination if the screening results were divergent. We had a three-step selection process: screened titles and abstracts to identify eligible studies, assessed the full text to determine relevance, and ensured that only studies aligned with our objectives were included. In addition, we excluded publications in any language other than English, reviews were excluded because we have objectively discussed relevant reviews on the same or similar topic in the background.
Inclusion and exclusion criteria
Inclusion criteria:
The type of study design was quantitative, qualitative, or mixed; Patients were 60 years of age or older (including all genders, regions, and ethnicities); Diagnosed with one or more chronic diseases; The topic of the study was about the facilitators, barriers, scenarios, and needs for DHTs;
Exclusion criteria:
Duplicate literature; Digital health intervention technologies that do not target people aged 60 years or older or chronic diseases; Studies that deviate from the research topic; Review, gray literature, protocols, conference papers, letters, and other literature without full text;
Data extraction and analysis
We created an Excel spreadsheet form to use in data extraction. Descriptive data of all the included literature were extracted and integrated in this study, including title, author, country, time of publication, type of study, study perspective, and type of chronic disease covered. Keywords of the included literature were visualized and presented using CiteSpace software.
We used NVivo 12 to create a coding scheme under four thematic categories: (1) facilitators, (2) barriers, (3) needs, and (4) scenarios. The complete article was imported into NVivo 10 as a pdf file and was coded back-to-back by two professional researchers (CL and YJ). Firstly, researchers read and encoded all texts that met the themes sentence by sentence to extract concepts, then, continuously analyzed the internal logic between concepts and condensed them into categories, finally, further explored the attributes of different categories to integrate them into scheme, and calculated the proportion of each category in the corresponding scheme. The controversial content will be discussed and identified with the other two professional researchers (LS and YC).
Results
Overview
Through initial search, we obtained 2117 articles. After removing 1204 duplicates and reading the titles and abstracts, 168 articles were considered. Upon full-text review, the final 47 articles were eligible for inclusion. This process is shown in Figure 1.

PRISMA flow diagram for the scoping review.
Keyword co-occurrence network
In Figure 2, by mapping the keyword co-occurrence for the abstracts of 47 literatures through CiteSpace, we found four main Key words: care, digital health, technology, and older adults, which almost matched the search themes we identified. In addition, we found the keywords with high frequency including COPD, mobile health, barriers, communication, e-health literacy, acceptance, perception, experience, education, support, and behavior, which provided important help for the thematic analysis we then carried out.
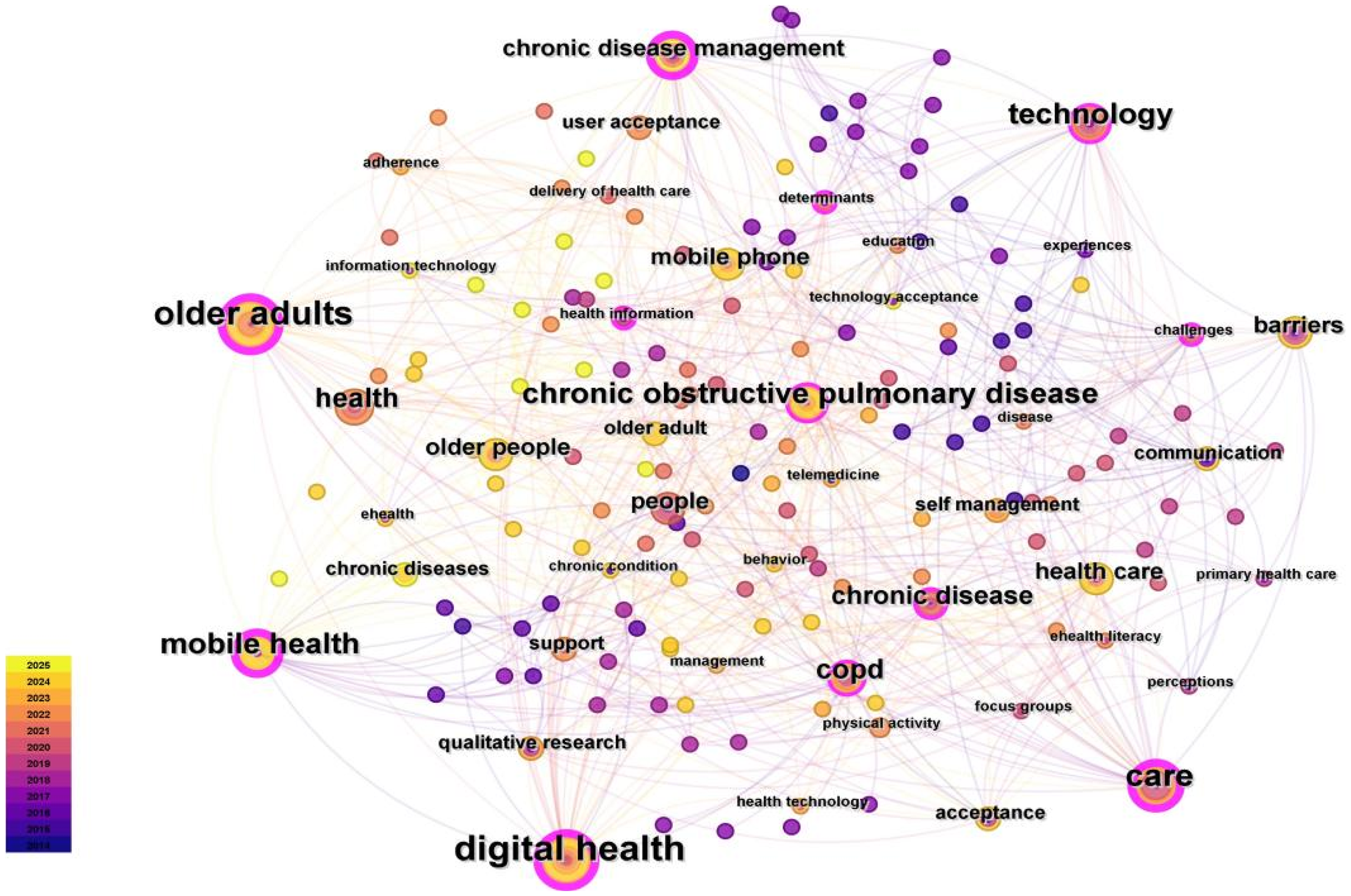
Keyword's main themes and concepts.
Data summary
We provide a summary of each included study in Supplementary Table 1 (see Appendix C). The number of studies published in 2024 was the highest. By region, 20 studies were from Europe, 14 from North America, and 13 from Asia, with the highest number of published regions being Canada (n = 8). By type, there were 10 quantitative studies, 33 qualitative studies, 4 mixed studies. By the study perspective, there were 34 studies based on the perspective of older people with chronic diseases, 5 studies from the physician perspective, and 8 studies covering both perspectives.
Overview of the facilitators for older people with chronic disease using DHTs.
By type of chronic disease, 14 studies did not specifically describe the type of chronic disease, 16 studies focused on a single chronic disease, and 17 studies focused on multiple chronic diseases, all included studies cover 16 chronic diseases, among which COPD (n = 20), type 2 diabetes (n = 10), heart failure (n = 6), and hypertension (n = 4) are the most concerned. Dementia is a chronic disease that requires great attention, due to poor understanding ability of the elderly, it greatly increases the difficulty of interviews or surveys, so many studies did not consider these people. Since there are many kinds of chronic diseases, we will analyze the distribution characteristics of DHTs mainly based on above four chronic diseases.
Types of DHTs
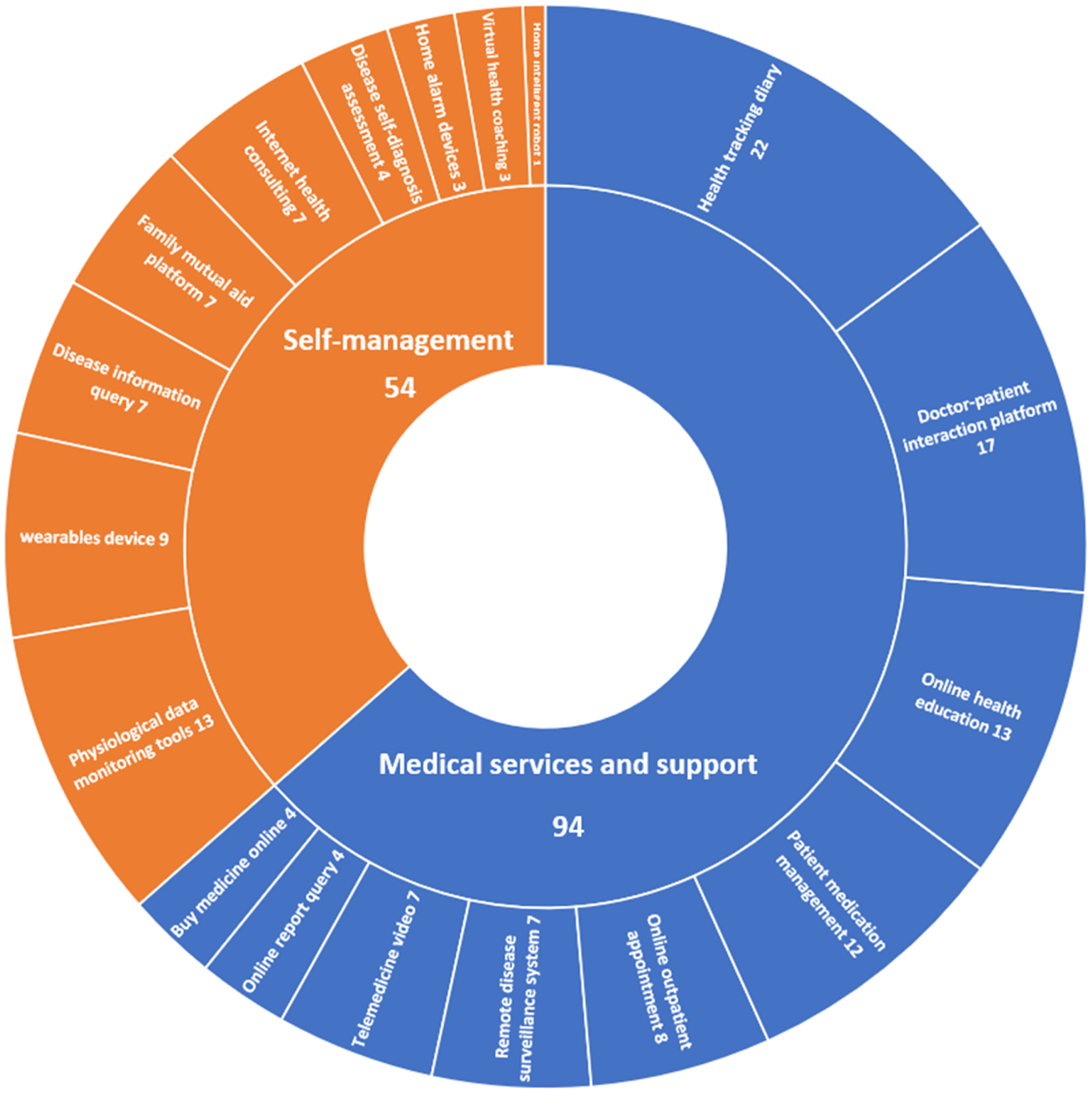
In Figure 3, the functions of DHTs can be generally categorized as Self-management and Medical services and support. In Medical services and support, DHTs is an effective tool to help older people with chronic diseases more conveniently access healthcare services and meet their medical needs and to help healthcare providers optimize the process of healthcare services and improve the efficiency of healthcare services. Health tracking diary is the most commonly used function, where patients actively record physiological indicators such as blood pressure, and daily life such as sleep quality and diet, the program automatically analyzes and generates reports, providing evaluation basis for doctors and patients. Online health education provides a platform where doctors provide personalized content based on the health status of each older adults, encouraging them to change unhealthy behaviors and lifestyles. Patient medication management is to remind and supervise patients on medication dosage to improve medication compliance. Remote disease monitoring system constructs a regional collaborative medical service platform or relies on devices similar to telepresence robot technology to monitor the management of chronic diseases in the elderly in real time.
Categories of digital health technologies (DHTs).
In self-management, DHTs is mainly used to improve the quality of life and physical health of older people with chronic diseases, rather than being limited to disease management. Physiological data monitoring tools are the most widely used digital technology. Internet health consultation is a low-cost and convenient service provided by a third-party platform, which covers health assessment, health guidance, medical advice, health education and other nondiagnosis and treatment activities. Disease information query provides patients with information related to chronic diseases, to achieve the correct understanding and scientific management. Disease self-diagnosis assessment utilizes internationally recognized chronic disease assessment scales, allowing patients to conduct health assessments at home. Family mutual aid platform promotes patients to share information with their family or friends. Home alarm devices mainly rely on behavior sensing systems and Internet of Things technology. Home intelligent robots provide elderly people with care services such as household cleaning, health management, and emotional companionship, greatly improving the convenience and quality of life.
Distribution of DHTs
Comparing by time, we can see from Figure 4 that self-management was almost equal than Medical services and support from 2014 to 2016, while Medical services and support had more number of apps after 2017, and from 2017 to 2019 it was mainly focused on Health tracking diary (n = 5).27–31 In 2020 to 2022, the number of Medical services and support and Self-management significantly increased, mainly concentrated in Health tracking diary (n = 8),32–39 and Intelligent wearable device (n = 5).34,35,37,38,40 It is worth noting that Disease self-diagnosis assessment, Family mutual assistance platform, Home robot only appeared after 2020. In 2023 to 2024, the number of Medical services and support is still increasing, mainly focused on Health tracking diary (n = 8),41–48 the number of Self-management has decreased, mainly focused on physiological data monitoring tools (n = 6).41–44,48,49

Application of digital health technologies (DHTs) in different periods.
Comparing by region, we can see from Figure 5, the largest number of DHTs were covered in Europe, with Medical services and support focusing on Health tracking diary (n = 7),27,29,31,34,35,37,38 Self-management focusing on Intelligent wearable device (n = 6).34,35,37,38,40,50 The number of Medical services and support in North America and Asia is higher than that in Self-management. Especially in Asia, the number of Self-management is very small, and Home robot, Home alarm devices, Virtual health coach, Disease self-diagnosis assessment is not involved.

Application of digital health technologies (DHTs) in different regions.
Comparing by disease, we can see from Figure 6, Health tracking diary was most commonly used in these four types of chronic diseases, and it is worth noting that the Family mutual assistance platform, Disease self-diagnosis assessment were all found in the COPD population, and Virtual health coach was found in the Diabetes population. The most commonly used technologies among COPD are physiological data monitoring tools and physician patient interaction platforms.

Application of digital health technologies (DHTs) in different chronic diseases.
Categories of digital health
Overview
In the 31 studies included, we explored four categories of DHTs for older people with chronic diseases: (1) Facilitators, (2) Barriers, (3) Needs, and (4) Scenarios. Regarding the Facilitators, we have confirmed the Experience of Use28,29,31–36,39,42,44,47–49,51–64 and Interpersonal Support.27,29,31,32,34,35,38,44,45,48,49,51,53,55,57–60,63–68 Regarding the Barriers, we have confirmed the Awareness of Competence,27,30,31,36,39–41,43–46,48,50–52,57–64,66,67,69–72 Technological Factors,27,28,30,31,34–36,39,40,42–45,48–54,56–64,69,71,73 Sense of Security,28,29,31,33,35,36,38–40,43–45,48–54,57–64,66,69–71 and Individual Factors.28,33,36,39–41,43–46,51,52,56,58,64,67–69 Regarding the Needs, we have confirmed the Service Functions28,29,32,33,36,38–49,51–55,57,60,63,65,66,69,70 and Subjective Needs.41–49,51–53,69 Regarding the Scenarios, we have confirmed the Home,27–35,38–44,47–56,58,59,61–63,65,66,68–71,73 Community,36,37,45,57,60,64,67 and Hospital.46,72
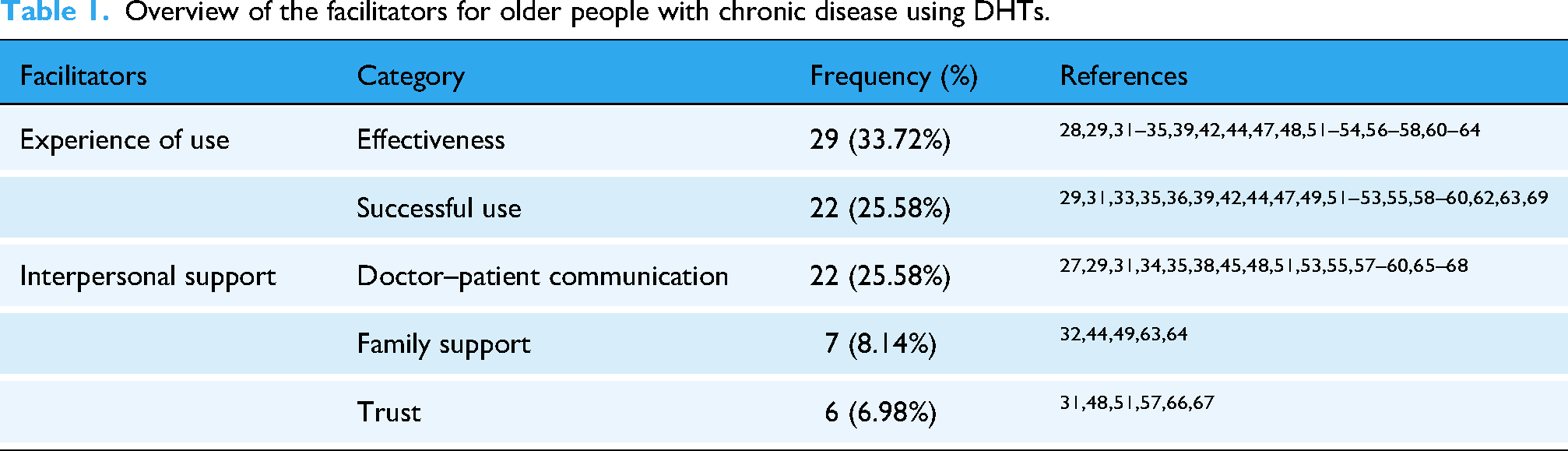
Facilitators
In Table 1, Effectiveness is the main driving force behind the use of DHTs among older adults, who focus on improving their quality of life, promoting health, providing medication advice, helping with dietary and nutritional management, and increasing physical activity. Successful use includes both easy-to-use technology and successfully mastering technological knowledge. In doctor–patient communication, feeling cared for and listened to is important, if they have long-term and effective communication with doctors, regularly share health information, and even receive some incentives (money, praise, etc.), they will be more willing to participate. Moreover, trust in the abilities of healthcare professionals is crucial.
Barriers
In Table 2, in awareness of competence, lack of experience and knowledge, limited learning ability, and spending many time learning greatly weaken the receptivity of older adults. Some people lack interest, manifested as resistance to new technologies or low initiative to learn.
Overview of the barriers for older people with chronic disease using DHTs.
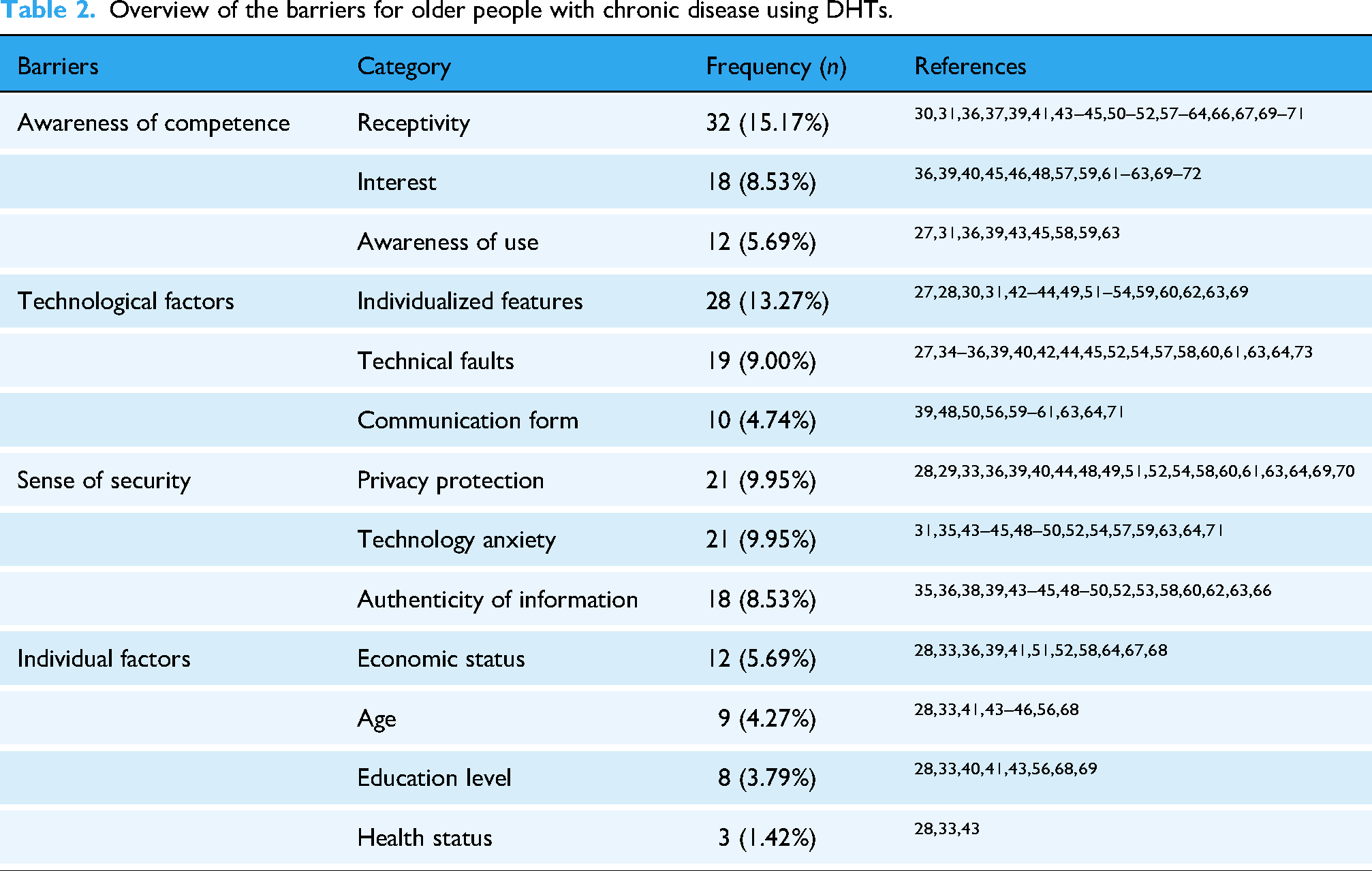
About technological factors, some DHTs lack personalized design, manifested as inadequate navigation functions, lack of targeted health education, insufficient language affinity, difficult-to-read icons and fonts, complex, and unnecessary service functions. New technologies will change the communication form; they are worried that they will reduce opportunities for face-to-face communication, social networking, and physical activity, which will make them feel lonely.
The lack of security is very tricky; most people are concerned about privacy breaches and online fraud and are unwilling to share health information. Technical anxiety is very common, elderly people worry about difficulty in dealing with urgent health conditions, mastering technical knowledge and adapting to updated and upgraded technologies, they feel oppressed when completing daily health tasks, often under the pressure of being monitored, and some negative technological news also makes them psychologically resistant. The authenticity of physiological monitoring data and Internet information, and the credibility of DHTs confuse the elderly.
Needs
In Table 3, Service Functions is the largest category for promoting DHTs, the elderly hope that digital technology can provide medication lists, develop scientific medication strategies, and promptly remind medication users. Also, older people hope that doctors have rich digital technology skills, empathy, and communicate with them through video, deeply participate in the process of formulating health plans, and increase the frequency of communication. About personalization, older people hope to obtain targeted disease information, help in reducing stress, and digital technology can automatically transmit their health information to doctors. Moreover, DHTs should have operability, manifested as being easy to carry, safety and reliability, having clear and simple page design, and providing instructional guidance for upgrading functions.
Overview of the need for older people with chronic disease using DHTs.
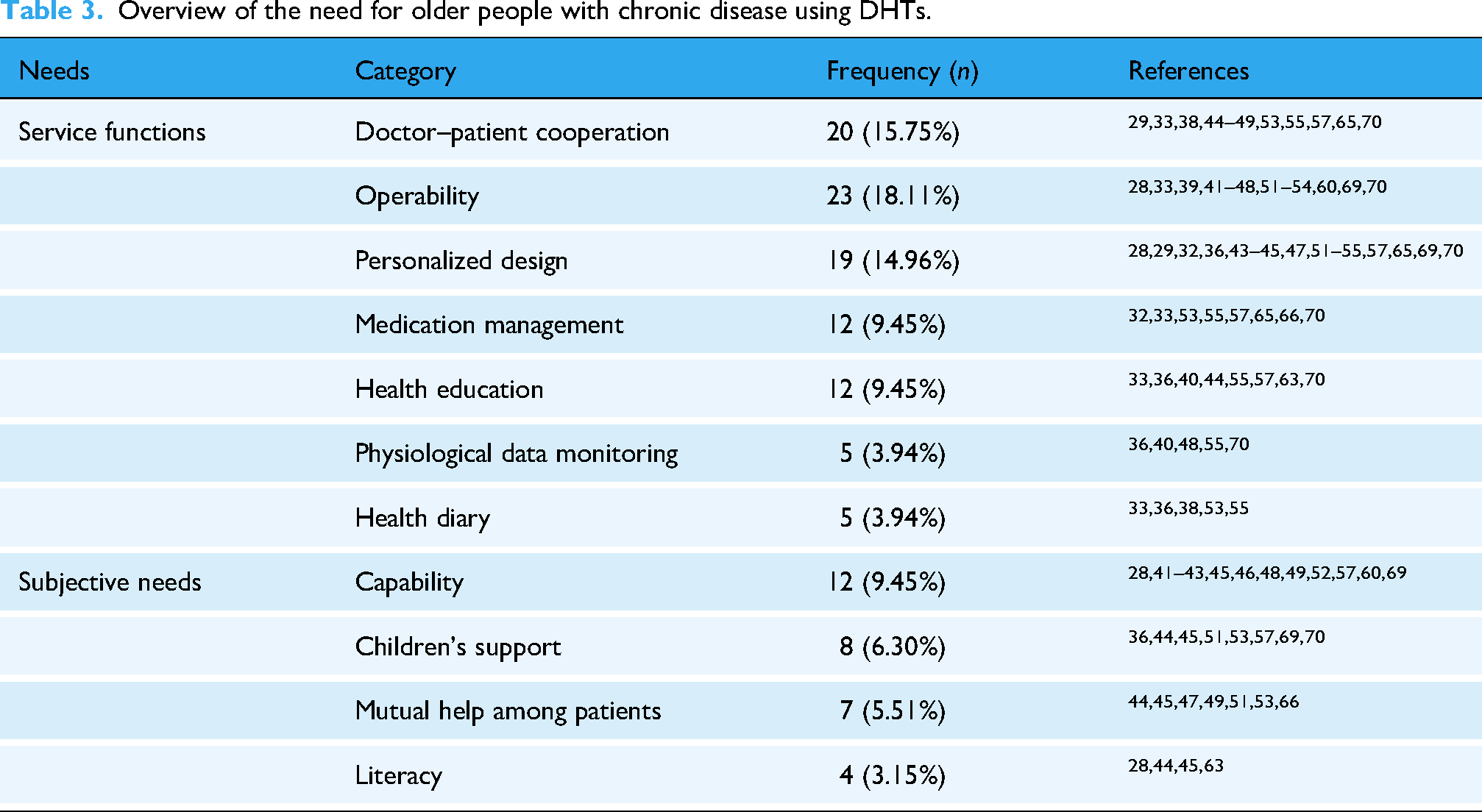
In subjective needs, Regular guidance and education are needed to enhance the elderly's ability to use DHTs and improve their digital literacy to be open to new technologies. In addition, older people have a strong desire to share information with their family and friends.
Scenarios
Home is the largest scene that adopts DHTs among older people with chronic diseases, mainly manifested in the following four areas: (1) using mobile health technology to monitor and collect disease data, online health consultation with specialists, online outpatient appointments, etc.; (2) developing telemedicine technology, using digital health platforms for telemedicine videos, health tracking diaries, self-diagnostic assessment of diseases, etc. using the Internet to access medical documents online; (3) using the Internet to access medical documents, query chronic disease information, etc.; (4) using smart wearable devices to measure vital signs in real time, and fall alerts for the elderly at home, etc.
Seven studies focused on communities, one Swedish study focused on the beliefs, attitudes, experiences, and expectations of people about DHTs in primary health care. 57 One Canadian study focused on the use of smart phones by diabetes patients in community health care. 67 Another Canadian study explored the potential characteristics for successful adoption of health management apps by doctors and patients. 39 A Norwegian study explored the use of DHTs by doctors to prevent fewer hospitalizations among home-bound older people receiving community-based care. 37 One UK study focused on the feasibility and potential effectiveness of a social network map assessment tool in Community Care for COPD Patients. 64 One Dutch study focuses on the needs, barriers, and facilitators of older people in the community using DHTs to access general practice services. 60 Korean study focuses on the preparation, challenges, and opportunities for implementing DHTs. 45
Only two study focused on DHTs in hospital scenarios, one exploring the perceptions of medical staff on interprofessional collaboration in the use of DHTs for medication management, 72 and the other exploring patients’ perceptions of doctors’ use of DHTs in clinical care. 46
Discussion
Main findings
In this study, we found relevant scientific papers on the use of DHTs in older people with chronic disease. Currently, DHTs have been widely used and promoted in the older people with chronic disease. Digital health technologies can be summarized as Medical services and support and Self-management, we have drawn meaningful conclusions by exploring the distribution characteristics of these technologies over time, region, and disease. More importantly, we identified four schemes: facilitators, barriers, needs, and scenarios. The Facilitators category contained Experience of Use, Interpersonal Support, and the Barriers category contained Awareness of Competence, Technological Factors, Sense of Security, Individual Factors, the Needs category contains Service Functions, Subjective Needs, The Scenarios category contains Home, The Scenarios category contains Home, Community, and Hospital.
Current Status of DHTs
In terms of time span, the number of studies is generally showing an upward trend, with a blowout growth in the number of studies in 2020 and 2024, which is closely related to the outbreak of the new coronavirus pneumonia and the mature application of technology. 74 Digital health technologies breaks the traditional healthcare service model and improves the accessibility and convenience of healthcare services to a great extent, there have been many studies on DHTs use for chronic disease management during the pandemic, but not necessarily focused on the elderly, our review fills the research gap in this field.75,76 The focus of research has evolved over time, early research, which focused more on physiological data monitoring tools and Internet health counseling services, subsequently, a variety of communication tools became popular, this is because the elderly hope to establish more social connections and share their lives with others on the basis of meeting health management needs. 77 James believed that social network interventions are a low-cost, high-yield social resource. 78 Although only seven studies in our review addressed the social connection of older people with chronic diseases, this may change in the near future as new information tools are rolled out.79,80
Geographically, developed countries in Europe and the United States have conducted the most in-depth research on the use of DHTs in older people with chronic diseases, particularly in the use of mobile devices to facilitate information exchange and feedback between doctors and patients and family mutual aid platform, because it can effectively improve the digital literacy of the elderly, enhance their initiative and enthusiasm to adopt and use self-management technologies.53,81 It can be seen that more technologies with higher levels of intelligence will be applied to the management of chronic diseases among the elderly. Niakan Kalhori et al. also proposed similar conclusions in their review. 82 However, some studies worried that it may increase the possibility of providing health interventions to older people who have difficulty accessing health resources.83,84 Heoretical study and achievement transformation of DHTs is more limited in developing countries. Both the number of studies and the scope of DHTs adoption lag far behind developed countries, with doctor–patient communication still using SMS for health management, and low cost and low network requirements facilitating the spread of apps, especially more prevalent in low-income countries, this is because many regions have immature digital technology, do not attach importance to self-management, and still rely on medical institutions to provide care services for the elderly.85,86 In addition, we found that over half of the research in Asia was conducted in 2024, indicating that DHTs are increasingly being valued in chronic disease management.
In terms of the types of chronic diseases, the chronic disease population with the most use of DHTs is COPD patients, on the one hand, COPD has become a global public health problem with high prevalence and mortality rates, 87 on the other hand, the new coronavirus pneumonia has exacerbated the prevalence of COPD, which in turn has led to a dramatic increase in the demand for medical care for COPD patients. 88 We found that the most involved DHTs were health tracking diaries and online communication platforms for doctors and patients. This is broadly in line with the findings of a number of other studies, most of which used telehealth technologies for COPD management, where mobile devices and virtual technologies are widely used to deliver health interventions outside of healthcare settings. 89 Lundell et al. showed through a meta-analysis that telemedicine improved physical activity in patients with COPD but had no significant effect on patients with dyspnea. 90 However, the Hanlon study found no significant impact of telemedicine on reducing mortality and improving health outcomes in COPD patients. 91 Sul et al. study shows similar results found in meta-analysis of telemedicine. 92 Whether DHTs can improve the quality of health management for COPD patients still requires further research.
Adoption of DHTs
Older people with chronic diseases have positive attitudes towards the acceptance of DHTs, but they are also affected by several factors. Effectiveness and interpersonal support are the main factors, older people hope to obtain advice on medication use and physiological data monitoring, DHTs help improve dietary and nutritional management, increase daily physical activity, and significantly reduce sedentary time through the use of DHTs to achieve the goal of improving quality of life and promoting health has greatly increased the initiative and motivation of older persons to use DHTs.93,94 Older people are better able to acquire knowledge and competence in DHTs through independent learning or with the help of others, so that they can gain more confidence and interest in embracing and exploring the potential of DHTs for use in daily life and chronic disease management.58,59,69 Doctor–patient communication is particularly influential in interpersonal support, where doctors or nurses follow up on the health status of older people with chronic diseases over time by phone or video, so that older people feel cared for and listened to.45,95
Being able to share with healthcare professionals the results or difficulties of using DHTs, and believing that using DHTs is a very important thing to do helps reduce isolation and feelings of being misunderstood.34,48,51 It is also important to have a trusting relationship between older people with chronic diseases and their healthcare providers, and trusting the healthcare provider is a prerequisite for talking about health conditions and experiences with DHTs.51,57 In addition, spouses or children of older people with chronic diseases who help them learn about DHTs and remind them to use them in their daily lives can similarly change older people's attitudes and frequency of DHTs use,54,64 Asia has started to pay attention in recent years.
Awareness of competence is a notable issue among the factors influencing older people with chronic diseases themselves. Most studies have found a general lack of experience and knowledge in the use of DHTs among older people with chronic diseases, with some older people believing that DHTs are too complex and require a lot of time and effort to learn.30,45 Frustration or failure in learning or use will completely demotivate older adults to learn DHTs.59,69 Some studies have found that some older adults lack interest in DHTs and even have an aversion and resistance to new technologies, and that the digital divide, traditional culture, limited technological skills and information-seeking behaviors increase older adults’ technological anxiety and resistance to change.60,69 Many studies have found that digital literacy positively impacts individuals’ physical and mental health.96–98
It is necessary to involve the elderly in the DHTs design process, some designs are not friendly to the elderly, such as complicated logins, unclear navigation, and difficult to read fonts, which also reduces motivation to learn.43,48,52,99 Especially in recent years of research, many older people have expressed a desire to participate in design technology.44,46,47 In addition, technological failures are of greater concern, older people with chronic diseases are prone to frustration, anger and disappointment when they encounter problems with network signals, hardware failures, etc., which leads to a reluctance to use DHTs again in older adults.31,45,54
Digital health technologies have changed the forms of social communication for older people, with less face-to-face contact via cell phones or the internet, makes people more distant from each other, older people with chronic diseases are more inclined to go to the hospital in person to buy medicines or queue up for outpatient appointments because it allows them to get out of the house and increase their opportunities for physical activity.56,63,64 Moreover, establishing connections with others can reduce the sense of emptiness among the elderly, which is very important for them.100,101
Additionally, a sense of security is an important consideration for older people using DHTs.54,102 Some patients consider disease status to be very private information and are reluctant to share it with uninvolved people become more cautious when using the internet, fearing that online access to health information or medical services is prone to cyber fraud, privacy breaches.48,54,57 Older people worry that it will be difficult for DHTs to cope with health problems in emergency situations, concerns about lack of IT knowledge or difficulty in adapting quickly to newer and upgraded features.62,70 Some older people may forgo the use of features and services because they are unable to distinguish the authenticity of Internet material.35,38,45
Our review shows that the majority of studies focused on the use of DHTs for home self-health management by older people with chronic diseases, they have higher acceptance and use of DHTs at home, but more exploration in the community and in healthcare organizations is still needed.103,104
Limitations
First, target population is older people with chronic diseases, but the distribution characteristics of technology mainly focus on COPD, diabetes, heart failure, and hypertension which may not be applicable to other chronic diseases. Second, DHTs may appear in the title or abstract as a specific technology or device, although we searched multiple databases, some research may still be overlooked. Thirdly, our review only considered research in English, which may result in missing some important studies in other languages.
Conclusion
The global aging trend and rise in chronic diseases highlight the importance of DHTs. Digital health technologies provide essential services, including medical support and services, as well as self-management, which exhibit different distribution characteristics in terms of region, time, and chronic diseases. Facilitators such as experience and interpersonal support, alongside barriers including awareness of competence and technological issues, significantly influence the adoption and effectiveness of DHTs. Despite a growing body of research and increasing usage, particularly in developed countries and for COPD, challenges remain in developing countries and with specific patient. Future studies should focus on addressing concerns about DHTs availability, security, and reliability in older people with chronic diseases. Incorporating feedback from the elderly and personalizing services are essential. Digital health technologies in the community and hospitals have great potential in the future with the full mobilization of positive social factors.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251348578 - Supplemental material for Current status of older people with chronic diseases adopting digital health technologies: A scoping review
Supplemental material, sj-docx-1-dhj-10.1177_20552076251348578 for Current status of older people with chronic diseases adopting digital health technologies: A scoping review by Chengjin Li, Hansong Wang, Jiajun Yuan, Lili Shi, Yunhao Chen, Zefang Gao, Liebin Zhao and Abilio Oliveira in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251348578 - Supplemental material for Current status of older people with chronic diseases adopting digital health technologies: A scoping review
Supplemental material, sj-docx-2-dhj-10.1177_20552076251348578 for Current status of older people with chronic diseases adopting digital health technologies: A scoping review by Chengjin Li, Hansong Wang, Jiajun Yuan, Lili Shi, Yunhao Chen, Zefang Gao, Liebin Zhao and Abilio Oliveira in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076251348578 - Supplemental material for Current status of older people with chronic diseases adopting digital health technologies: A scoping review
Supplemental material, sj-docx-3-dhj-10.1177_20552076251348578 for Current status of older people with chronic diseases adopting digital health technologies: A scoping review by Chengjin Li, Hansong Wang, Jiajun Yuan, Lili Shi, Yunhao Chen, Zefang Gao, Liebin Zhao and Abilio Oliveira in DIGITAL HEALTH
Footnotes
Acknowledgments
The authors thank the Shanghai Jiao Tong University School of Medicine Library for guiding us in developing an accurate search strategy.
ORCID iDs
Author contributions
LZ and AO conceived of the scoping review and participated in the design. CL and HW participated in screening literature, coding, and drafting the manuscript. HW, JY, LS, YC and ZG participated in the revision of titles, abstracts, and reviews. All authors have contributed to manuscript refinement.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Fund of China under Grant number 72293585; Fundamental Research Funds for the Central Universities under Grant number YG2022QN095; Shanghai Public Health Excellent Talent Project under Grant number GWVI-11.2-YQ58. Shanghai Public Health Excellent Talent Project, National Natural Science Foundation of China, Fundamental Research Funds for the Central Universities (grant number GWVI-11.2-YQ58, 72293585, YG2022QN095).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
LZ and AO.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.