
Abstract
Objective
Advance care planning (ACP) is a dynamic communication process about future care preferences. We aimed to develop and test an ACP support website for people with dementia and their family caregivers.
Methods
We adopted a user-centred design process to develop and test the ACP support website. A content specification phase included needs assessment, evidence synthesis and translation into preliminary content. A creative design phase included storyboarding, iterative prototyping, and usability testing. People with dementia and family caregivers engaged in usability testing across four iterations, using System Usability Scale questionnaires, and think-aloud and semi-structured interviews. An advisory group with people with dementia, family caregivers, and diverse regional stakeholders was involved. Descriptive statistics and qualitative framework analysis were applied.
Results
Website goals were: providing ACP information and facilitating ACP conversations. A ‘what matters most’ approach (i.e. enabling users to reflect on ‘what matters most’ in the present and the future) and non-linear navigation were favoured. We tested the website with 17 people with dementia and 26 family caregivers. Feedback addressed design, navigation and content. Usability scores of 76.4 for family caregivers and 81.3 for people with dementia were achieved. Family caregivers and people with dementia highlighted the value of information and interactive ACP tools, the need for language simplification and harmonised layout. People with dementia experienced challenges in using interactive tools.
Conclusion
The user-centred development process, involving diverse stakeholders, led to the development of an ACP support website deemed usable and useful. Future evaluation should focus on acceptability, feasibility and effectiveness of the ACP support website.
Keywords
Introduction
Background
Advance care planning (ACP) has recently been defined as a process that enables individuals to identify values, reflect upon the meanings and consequences of serious illness scenarios, and define goals and preferences for future care and medical treatment.1,2 Over the past decades, ACP shifted from being a doctor-led, medical process focused on the end of life to a more comprehensive approach involving continuous communication among patients, families and health professionals about preferences for future care and treatment including at the end of life. 3 Table 1 provides an overview of the characteristics of ACP, as defined by the European Association for Palliative Care. 1
Advance care planning (ACP) characteristics.

Given the progressive nature of dementia and the decline in cognitive and functional abilities of those affected by dementia, ACP has been advocated to be particularly important for people with dementia and their family caregivers. 4 Within the context of dementia, several studies have found that people commonly discuss ACP within the family context, and in some cases even engage in more ACP conversations with family than with healthcare professionals. 5 Furthermore, it was found that some people with dementia and family caregivers prefer to discuss values and preferences in a flexible manner with family. 6 This is in line with a public health approach in palliative care highlighting the strength of having conversations about future care and preferences within the family context, to supplement conversations in a professional or medical context. 7 Indeed, the public health approach argues that initiating ACP by exploring values and broader life aspects within the family context can establish a foundation for important considerations like treatment preferences and preferred places of death within the medical context. However, until now, there has been little development of tools that could support people with dementia and their family caregivers in this process.
Web-based tools can provide accessible platforms in this regard. 8 Technology, and especially web-based tools, has been advocated as a good way to support ACP and has shown significant potential in meeting the unique needs of people with dementia.9,10 Web-based tools offer flexibility, allowing users to access them at their convenience, at any location, and their own pace. They can be used independently, with or without the involvement of health professionals or family caregivers, making them accessible to a broader audience. 11
Importantly, previous research has shown that adopting a user-centred approach is paramount when developing web-based tools for people with dementia.12–14 This approach prioritises the needs, preferences and abilities of the end-users throughout the development process, ensuring that objectives and content align closely with their specific requirements.12,13,15 Furthermore, the user-centred approach promotes usability, accessibility and acceptance of technology, resulting in enhanced user experiences and outcomes.16–18 In line with the user-centred approach, the growing recognition of the importance of patient and public involvement (PPI) in dementia research highlights that the expertise and lived experiences of people with dementia and their family caregivers need to be considered.14,19,20 PPI in dementia research encourages the co-design and evaluation of interventions, including web-based tools, to ensure they are user-friendly, acceptable and effective.20–22
Despite the potential benefits, there are currently no rigorous and comprehensive web-based tools that specifically consider the unique needs of people with dementia in the context of ACP. Existing web-based ACP tools are not developed for or tested with people with dementia, and are rarely based on theory. 23 Therefore, they may not address the specific needs of people with dementia and their family caregivers and may lack accessibility. People with dementia can have quite specific needs in terms of ACP compared to other illnesses. For instance, the role of family becomes increasingly important in the ACP process as the disease progresses and cognitive abilities gradually decline.24,25 People with dementia and their family caregivers may also face barriers such as a lack of awareness or knowledge about ACP or difficulties initiating and engaging in such sensitive conversations.4,6,26,27 To bridge this gap, there is a need for research that focuses on the rigorous and user-centred development and evaluation of a web-based ACP tool targeted at people with dementia and their family caregivers. Such a web-based tool is not intended to replace all aspects of the ACP process, as for some parts (i.e. when medical end-of-life scenarios or decisions are discussed) healthcare professionals will need to be involved. It is intended to provide the support needed to reflect and initiate conversations, including those with professionals.
Objectives
In this study, we aimed to develop and test an evidence- and theory-based website to support people with dementia and their family caregivers when engaging in ACP within the family context. To maintain clarity and consistency throughout our study, we use the term ‘ACP support website’.
Methods
Overall design of the study
This development and usability study followed the process map proposed by Elwyn and colleagues for developing web-based decision support interventions 28 and adhered to the development phase of the Medical Research Council (MRC) framework for complex interventions. 29 The study took place in Flanders, the Dutch-speaking part of Belgium and with Dutch-speaking participants in Brussels, where both Dutch and French are official languages, and was conducted from September 2020 to June 2022. An overview of our development approach and timeline is provided in Figure 1. It involved two main phases, i.e. content specification and creative design, in which we adopted user-centred design principles and continuous stakeholder engagement. A comprehensive outline of the research methodology can be found in the published study protocol. 30

Overview of the development process and usability testing of the ACP support website.
The content specification phase consisted of a user needs assessment, evidence synthesis and translating evidence into a preliminary content for the website. The creative design phase consisted of storyboarding, iterative prototyping and usability testing. We adopted an agile development approach, specifically the Scrum method, to create the ACP support website prototypes.31,32 This approach involved iterative and dynamic development, collaborating with various stakeholders, and continuously improving the design through rapid feedback and testing. The Scrum method, known for its emphasis on feedback loops, involves short development timeframes called sprints, typically lasting around four weeks. This led to the development of four prototypes over five stages, encompassing 1 pre-sprint and 4 sprints where the website was developed and tested iteratively. User views and input were sought throughout the development process. Furthermore, meaningful PPI consultation sessions were conducted with an advisory group set up for the purpose of this study.
Stakeholder engagement throughout website development and testing
Following the process map for developing web-based decision-support interventions, 28 four distinct stakeholder groups were involved throughout the development process. These groups encompass a project management team, consisting of FM, CD, LVdB, LP and TS; a project group comprising all the authors of this paper; a technical production group consisting of a contracted IT partner; and an advisory group created for the purpose of this study, which was composed of people with dementia, family caregivers, representatives from regional dementia associations and palliative care experts. This advisory group was consulted in the context of PPI throughout the development process through online meetings and email correspondence.
Content specification phase
User needs assessment
We used four data sources to explore and specify the content of the ACP support website: (1) systematic review of publicly available, interactive web-based tools to support ACP (sub-study 1), 33 (2) content analysis of information on ACP on websites of dementia associations (sub-study 2), 34 (3) focus groups and interviews with the European Working Group of People with Dementia (EWGPWD) on their perspectives of ACP (sub-study 3) 35 and (4) focus group with family caregivers and health professionals to define the content of an ACP support website for people with dementia and their family caregivers (sub-study 4). 36 Supplemental Material 2 provides an overview of the objectives and methods utilised in each sub-study conducted as part of the user needs assessment. The results of these sub-studies are reported in previous publications.33–36
Evidence synthesis
The findings of the user needs assessment were integrated to draw out core elements for the website. A comprehensive summary table was generated, presenting the main findings from each individual data source. Subsequently, a content analysis was conducted by comparing the findings of all sub-studies to identify points of convergence, instances of complementary information, or areas of divergence among the findings from each sub-study.
Translation into preliminary content
Based on the results of the evidence synthesis, we used intervention mapping principles to create the first content of the ACP support website.37,38 More specifically, we identified theoretical methods and practical applications to translate the synthesised evidence into preliminary website content. This means that using broad methodologies designed to change factors determining behaviour (i.e. theoretical methods) 37 and tailoring it to suit the characteristics of our target population and our specific context (i.e. practical applications), 38 we identified core elements that the website should contain. To transform theoretical methods into practical applications, we required a thorough understanding of the underlying theories associated with the methods.37,39 Thus, based on diverse theories, we selected theoretical methods of behaviour change to achieve the website's aims and subsequently translated this to the content needed for the website itself. We identified theoretical methods via the intervention mapping handbook to find theoretical methods that influence specific determinants. 37 The results of our focus groups with family caregivers and health professionals (sub-study 4), where we inquired about what the target group believed were effective strategies were also used in this stage. 36
Creative design phase
The results obtained during the content specification phase informed the creative design phase of the ACP support website. We created an initial structure of the website and related materials in the form of a storyboard (i.e. visual outlines of the website's layout and user flow). We then developed a first working prototype of the website and proceeded to conduct usability testing with participants using an iterative process.
Storyboard
The project group, in consultation with the advisory group, created a storyboard that considered various crucial factors, encompassing the website's structure, navigation pathways and the design of materials. This involved decisions on how information would be presented, the incorporation of interactive elements, and the integration of features such as accessibility features or media. The storyboard phase was approached as a dynamic process, remaining open to significant alterations based on insights gained from usability testing.
Iterative usability testing
Setting and participants
Participants for usability testing of the website were recruited in Brussels and Flanders through organisations such as the Flemish Alzheimer League and memory clinics. To test both independent and joint use of the website, participants included people with dementia, family caregivers, or dyads of both.
Inclusion criteria for people with dementia were: (1) being aware and informed of their diagnosis, (2) having an interest in and being willing to test an ACP support website, (3) speaking and understanding Dutch, (4) being able to understand the information about the study, (5) being able to sign a written informed consent form.
The inclusion criteria for family caregivers were: (1) being the main or primary caregiver of person formally diagnosed with dementia, (2) having an interest in and being willing to test an ACP support website, (3) being 18 years of age or older, (4) speaking and understanding Dutch. We aimed to include a diverse group of people with dementia and family caregivers in terms of age, gender and type of dementia. As sample size, we sought to include 12 participants per sprint, of which 3 people with dementia, 3 family caregivers and 3 dyads. For every testing iteration (i.e. sprint), new participants were recruited through a convenience sampling method.
Patient and public involvement
We conducted continuous PPI with the advisory group. The pre-sprint solely consisted of a PPI consultation with the advisory group. A brief presentation was given about the ACP support website and the aims of the research projects, followed by a short discussion. Topics included different possibilities for layout and structure of the website, as well as the evaluation of potential mood boards (e.g. colour schemes, fonts). The content of the following sprints and prototypes was determined. The storyboard and notes from the meeting were the base for developing the first prototype of the ACP support website.
We also conducted a PPI consultation at the end of each sprint. Meetings started with a brief presentation of the findings from usability testing with participants, followed by a discussion. Topics included the structure, layout and content of the prototypes.
Data collection procedures
We conducted usability testing from sprint 1 through 4. In sprint 1 to 3, we tested the usability of the ACP support website with people with dementia, family caregivers and dyads. Each testing session occurred in participants’ homes and started with a questionnaire covering sociodemographic characteristics, followed by a think-aloud exercise on predefined tasks to be conducted on the website. 40 Participants were given tasks and verbal instructions to navigate through the ACP support website prototype, using the think-aloud method to express their thoughts, impressions and feelings. A researcher (CD), who is also a nurse and has experience working with people with dementia, observed and took note of the participants’ physical cues, successes in tasks, mistakes, difficulties, or comments. 40 The researcher minimised interference so the prototypes’ intuitiveness could be captured, intervening only when participants remained silent for too long. Participants’ perspectives on usability were further evaluated using a usability survey, the System Usability Scale (SUS). 41 In sprint 4, all participants were requested to complete a sociodemographic questionnaire. Subsequently, people with dementia, family caregivers and dyads were asked to explore the ACP support website and provide feedback through a semi-structured interview. All think-aloud and semi-structured interviews lasted between 20 and 60 min.
Data collection measures
In each sprint, participants rated system usability of the ACP support website prototype on the 10-item SUS (see Supplemental Material 1). 41 The SUS can measure subjective usability of a website in terms of effectiveness, efficiency and satisfaction. Responses were recorded on a 5-point Likert-type scale. 42 Total SUS scores were converted to a 0 to 100 scale, with higher scores indicating better usability. 42 A SUS score above 68 is considered above average, 43 indicating acceptable experienced usability.
Data analysis
The think-aloud and semi-structured interviews were audio-recorded and transcribed verbatim. All transcripts were pseudonymised. The field notes from the observations were utilised to supplement the data obtained during the think-aloud exercises. During sprints 1 to 3, framework analysis was conducted on the notes taken by researchers during the think-aloud sessions.44,45 When necessary, the audiotapes were reviewed to enhance the completeness of the notes. Framework analysis is a form of thematic analysis that involves several stages, including data familiarisation, thematic framework development, indexing all data against the framework, charting to summarise this data, and lastly mapping and interpretation.44,45 Following sprint 4, framework analysis was also used to analyse the transcripts of the semi-structured interviews. FM and CD familiarised themselves with the data by listening and immersing themselves in the interview transcripts and audio-recordings. Based on the interview guide, we developed subcodes which constituted our preliminary framework. FM and CD applied the framework to all the transcripts. Next, all indexed data were charted onto a framework matrix by summarising participants’ interviews and arranging them by categories (i.e. subcodes). This facilitated analysis within and between each interview, and the preparation of data for interpretation.
The data obtained from the SUS questionnaire complemented the Insights from the think-aloud sessions and interviews. The data were analysed using SPSS (SPSS Inc), v25. Mean scores and standard deviations (SD) were calculated for people with dementia and for family caregivers. We used descriptive statistics to describe sociodemographic characteristics of the participants.
Results
Content specification phase
Based on the needs assessment and subsequent evidence synthesis, we could draw several key lessons regarding the aims and content of the ACP support website. A full account of these findings is described in Supplemental Material 2; here we provide a summary.
First, we identified two distinct aims for the ACP support website i.e. to provide information about ACP and to support communication about ACP. Participants in our focus groups on the content of the ACP support website (sub-study 4) highlighted that information about ACP (e.g. what it is and why it is done) and guidance on how to start and conduct ACP conversations throughout the dementia trajectory, should be the main aims of the website. 36 Core components of the ACP support website should be: information, reflection and communication, and decision-making and documentation.33,34,36 Regarding specific elements of the website, our participants expressed a desire for testimonials from peers and from health professionals who have already been involved in ACP. They wished for an ACP support website that would enable them to discuss ACP within the family context, before engaging in discussions with health professionals. 36
Second, a ‘what matters most’ approach to ACP seemed most appropriate for a website to support ACP within the family context. Insights gathered from the EWGPWD (sub-study 3) stressed the importance of adopting a holistic approach of ACP that prioritises what matters most to people with dementia and their family caregivers. 35 The EWGPWD found that while medical aspects of care are an important part of ACP, social aspects of care, conversations about what matters to people in the present and in the future, and future meaningful daily activities should be included in the process of ACP. Our literature review of web-based ACP tools (sub-study 1) and our content analysis of dementia associations’ websites (sub-study 2) showed that this ‘what matters most’ approach is not commonly adopted. Indeed, a significant portion of web-based ACP tools included in our literature review (sub-study 1) did not comprehensively cover every aspect of the ACP process (e.g. ACP definition, legal frameworks, care preferences, documentation, personal values, communication with family and health professionals, and handling future serious illness scenarios). 33 This finding was corroborated by our content analysis of the ACP information on dementia associations’ websites (sub-study 2), which revealed that only a limited number of websites addressed all aspects of ACP. 34 Notably, the emphasis was on medical and legal aspects of ACP.
Third, navigation should not be linear and forced upon the users. We found that most ACP tools generally adopted a linear approach to ACP, where users are guided through a predetermined sequence of steps (sub-study 1). 33 However, it is important to note that ACP should ideally be a flexible process involving exploration, discussions and the documentation of preferences and decisions. The appropriateness of predefined steps can vary depending on people's readiness, personal barriers and preferences towards ACP. Some people may seek to explore options without immediately engaging in ACP discussions, while others may prefer to prioritise decision-making. Our focus groups (sub-study 4) also identified the need to account for users’ varying levels to engage in ACP in the structure of the website. 36
Next, the lessons learned from the evidence synthesis were discussed within the project group to translate the evidence synthesis into aims, methods and specific content of the ACP support website. An overview is shown in Table 2. The identified aims of the website were: (1) users are informed about ACP and (2) users engage in ACP conversations, measured via several outcomes, including knowledge, attitudes, self-efficacy, perceived barriers and skills. Then, we identified several theories (e.g. protection motivation theory, social cognitive theory, etc.) and methods of behaviour change (e.g. using arguments, positive framing, modelling, etc.) that could be applied to the outcomes targeted by the ACP support website. We then created specific content of the ACP support website based on this process, such as different tips on how to conduct ACP or testimonials from dyads who have already been involved in ACP.
Website aims, outcomes targeted, methods used and corresponding theoretical basis, and website content.

Creative design phase
Storyboard and pre-sprint
Based on the work in the content specification phase, the project group and the advisory group jointly developed an initial website structure, resulting in the structure of the website presented in Figure 2. A few important accessibility features were also selected such as a text-to-speech option, a contrast option and a font size option. We also determined that it would be important to ensure that content could easily be printed.

Initial website structure diagram.
Additionally, the project group developed the materials for the ACP support website, drawing upon their collective expertise. First, to provide comprehensive information, we presented a complete overview of the ACP process, as identified in our content specification phase. We built the information on the website around the following core ACP processes, as identified in our content specification phase 33 : (1) information, (2) reflection and communication and (3) decision-making and documentation.
To inform users about ACP, a part of the website is dedicated to explaining what ACP is and what its potential benefits might be. To maintain clarity and manage the text volume, we created a glossary and frequently asked questions sections on the website, where essential terms specific to ACP and dementia, in the Belgian context, are explained. For instance, these sections describe terms such as ‘Do Not Resuscitate’ (DNR), quality of life, family caregivers, organ donation, palliative care, patient rights, power of attorney, capacity, euthanasia, or advance directives and the legal frameworks surrounding them. To support ACP reflection and communication, a part of the website provides a set of recommendations on communication about ACP. We developed two interactive communication tools. The first tool, the ‘Life Wishes Cards’ (Levenswensen kaarten in Dutch) is an adaptation of the ‘Go-Wish’ cards developed in the United States. 52 The cards are designed to facilitate discussions about wishes and preferences regarding the end-of-life, using preformulated statements that can be sorted. We previously translated and culturally adapted the original cards for use in Flanders, Belgium 53 and digitised them for our website. The second interactive communication tool, named ‘Thinking Now About Later’, is a fill-in tool that guides users through a reflective process by offering prompts and questions to think and talk about the future. Its primary goal is to help users think and talk about and write down their preferences for the present as well as the future, taking the lens of ‘what matters most’. It also helps users in the process of choosing a proxy decision-maker, in deciding whether they want to document any preferences in formal advance directives, and in determining the next steps including conversations with family and friends as well as health professionals. LVdB and CD led the development of this fill-in tool drawing on the expertise of the project group. Finally, to support ACP documentation, we provide access to existing templates for advance directives in Belgium 54 and encourage users to discuss these with healthcare professionals.
The pre-sprint was dedicated to determining the look and feel of the ACP support website. Based on the content specification phase and storyboard, the advisory group selected a mood board (i.e. colours, etc.). For instance, neutral or depressing colours were rejected in favour of more uplifting and positive colours. Furthermore, the advisory group and the project group planned for the development of the website and the content of the following sprints was determined. Sprint 1 evaluated the homepage and structure of the website, sprint 2 focused on the information components of the website and sprint 3 concentrated on the communication tips and interactive communication tools. Sprint 4 evaluated the final prototype composed of the entire website.
Usability testing
Participant characteristics
In total, 17 people with dementia and 26 family caregivers took part in the usability testing of the ACP support website prototypes. Of these, there were 10 dyads, while 7 people with dementia and 16 family caregivers participated on their own. Table 3 shows their demographic and dementia-related characteristics. People with dementia rated their computer skills between 5 (SD = 3.5) and 6.6 (SD = 1.5), while family caregivers rated their computer skills between 7.8 (SD = 1.1) and 8.4 (SD = 1.5) (scale 1 to 10).
Characteristics of study participants.
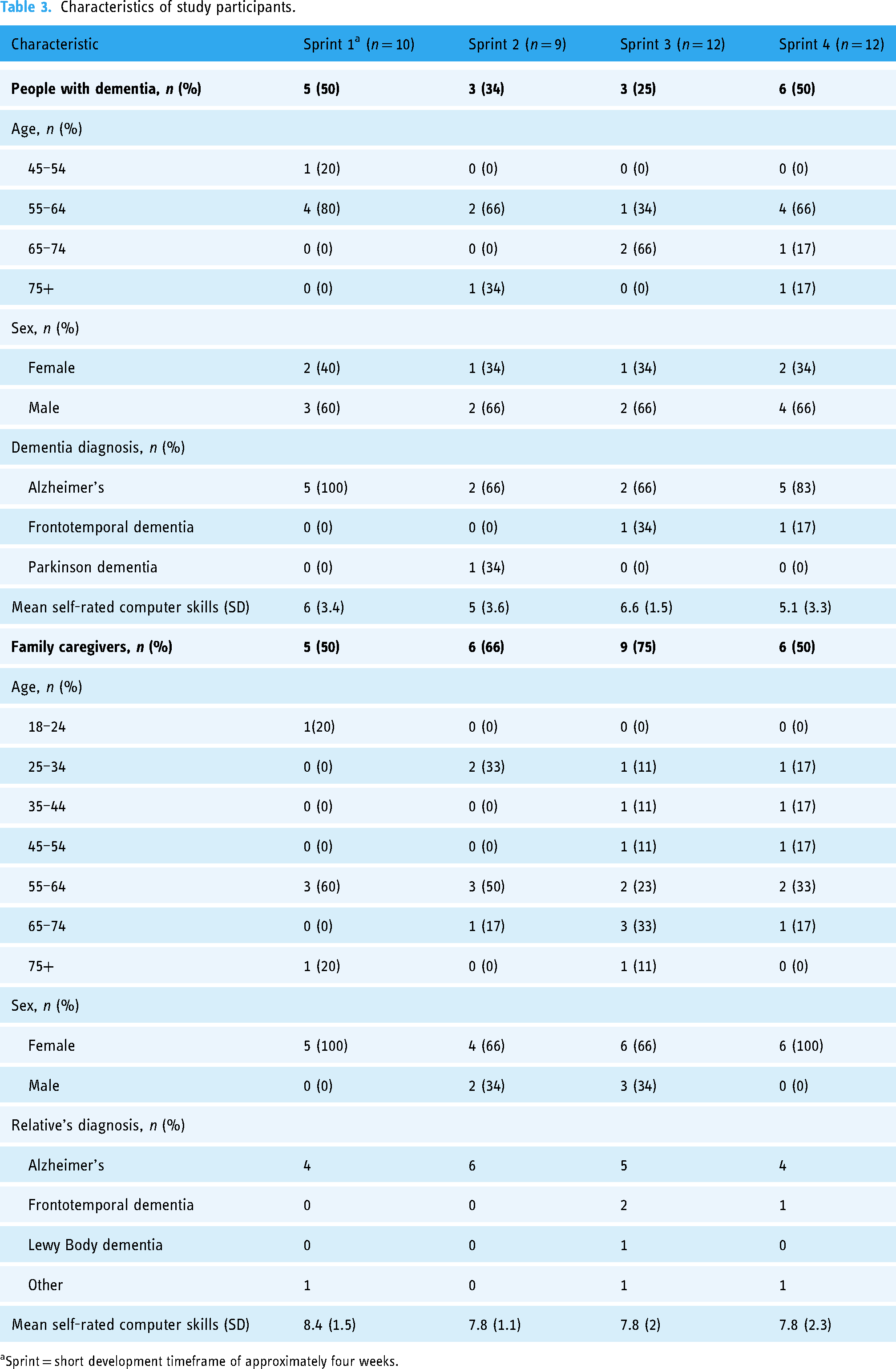
Sprint = short development timeframe of approximately four weeks.
Iterative development and usability testing of the ACP support website (sprint 1 to 3)
The time from the completion of a usability testing sprint to the implementation of website revisions and addition of new content was approximately 1 to 2 months. Figure 3 shows the means of the SUS score for people with dementia and family caregivers in each sprint. Overall, users gave the website prototypes a total mean usability score ranging from 72.5 (SD = 11.5) to 82.5 (SD = 7.5). Participants’ feedback on the prototypes ranged from comments on design, navigation or content, to comments on the device used to test the website. An overview of suggestions made by participants and the advisory group and the resulting modifications are described in Table 4.
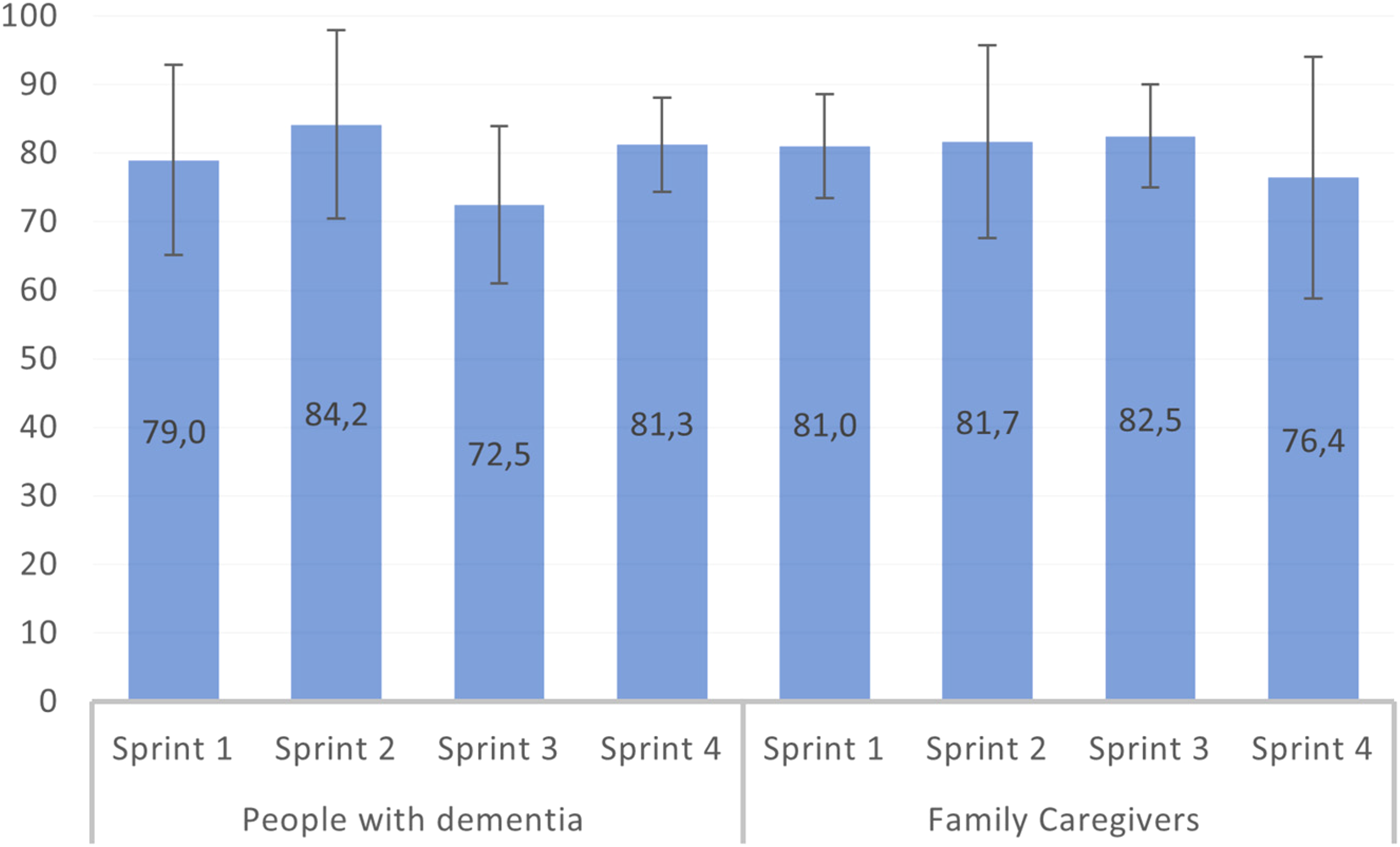
Mean SUS scores and SD per sprint for people with dementia and family caregivers.
Usability testing feedback and revisions made from pre-sprint to sprint 3.

Usability testing of the final prototype of the ACP support website (sprint 4)
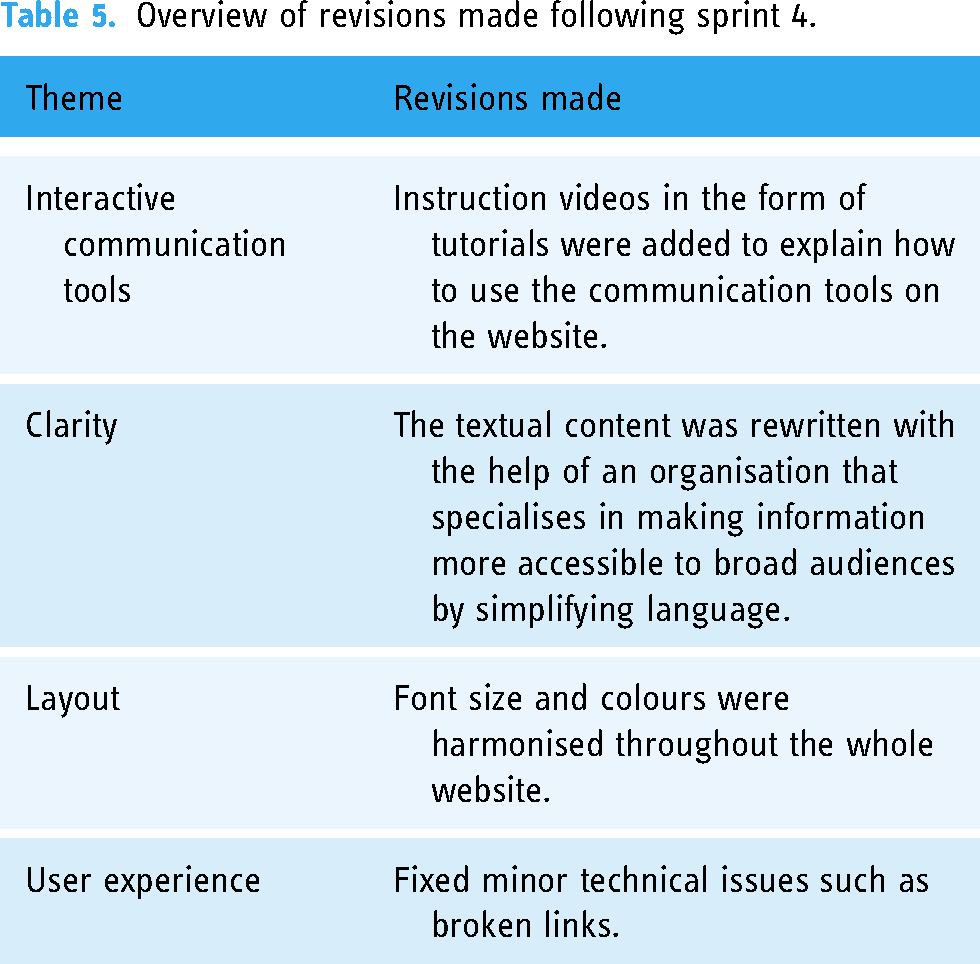
The last usability testing sprint was conducted to test the entire website with users. Overall, family caregivers rated the usability of the whole website with a mean SUS score of 76.4 (SD = 17.6) and people with dementia with a mean SUS score of 81.3 (SD = 6.8; see Figure 2). The feedback revolved around the following themes regarding the website: clarity, usefulness, user experience on the website and layout. Table 5 presents the final revisions that were made to obtain the final prototype.
Overview of revisions made following sprint 4.
In the semi-structured interviews, most participants described a positive user experience on the website. Some reported small issues such as encountering broken links while they tested the website. Overall, they found the website useful and thought that the information provided was complete and the tips and interactive tools were an ideal place to start the discussion on ACP. Many participants mentioned that they would use the website regularly in the future. Both the interactive tools were particularly appreciated by most of our participants. It's not always so easy. It's not that simple to put things down on paper of ‘what do I want?’ But then when you see these tools such as the cards or the reflection and fill-in tool, that can help you in your process. – Person with dementia #1
Although the interactive communication tools were seen as useful, several participants also mentioned that it was difficult to understand how they worked exactly and that they would benefit from clearer instructions. Indeed, some had difficulties with navigating the fill-in tool, and others had issues with understanding how to skip or move the cards within the card tool.
And then the cards… That part, I found it a bit more challenging… with the dragging. I’m not really a computer person. I have to do it, but that's all things that I didn’t grow up with, you know. And I had some problems with it, and then I sat there searching. […] So I don’t find it easy. – Person with dementia #4
Most participants praised the clarity of the website, including the goals of the website, the clarity of the information provided, as well as the tips given. They noted that the language was easy to understand and that the accessibility features incorporated on the website, such as the text-to-speech option or the font size option, were helpful. However, more than half of the participants still found the text too long, and the website too busy. They suggested that the written content could be more to the point, which would also improve the clarity of the website overall.
Also, I share the opinion that the sentences are too long. I think you could write the same text much more concisely and much more understandable. And someone should proof-read it carefully as well. – Person with dementia #3
Due to the difficulty of the textual content, most family caregivers and two people with dementia also noted that people with dementia would not necessarily be able to use the website on their own and that they would most probably need assistance from family caregivers.
Finally, all participants seemed to be satisfied with the navigation of the website. One feature that was noted by several participants was the advantage of being able to go through the website in their preferred order, and not having to go through a linear process.
Sometimes you have to go through a whole bunch of pages before you actually get to the page that you want. Here you can actually go directly to your page and I think that’s an advantage. Each item is separate from the other and I actually like that. – Family caregiver #4
Participants also noted some inconsistencies in font sizes or in use of colour on different webpages, which they found lead to a lack of harmony on the website.
Figure 4 provides a screenshot of the final website home page, see Supplemental Material 3 for additional selected screenshots of the website.

Screenshot of the ACP support website homepage (in Dutch).
Discussion
This study outlines the outcomes of an iterative and user-centred development process of a website to support people with dementia and their family caregivers to engage in ACP in the family context. It provides access to a range of information ranging from what ACP is and what its benefits can be, to explanations of advance directives and difficult terms and jargon used in ACP (e.g. decision making capacity or DNR). The website also provides tips on how to communicate about ACP within the family as well as with health professionals. Moreover, we developed and tested two interactive communication tools that users can use to reflect about ACP or to facilitate their ACP conversations: (1) the ‘Life Wishes Cards’, which allow users to sort statements about their wishes for future care and (2) a fill-in tool that allows users to reflect about preferences for what matters most to them now and in the future. Features integrated on the website included a font size option, a text-to-speech option, a contrast option, several videos from health professionals and testimonials from people with dementia and family caregivers about ACP.
The ACP support website presents several innovative features that distinguish it from other ACP web-based tools. Notably, our website takes a ‘what matters most’ approach to ACP. By focusing on ‘what matters most’ to people in the present and for the future, the website encourages the identification, not only of preferences for medical aspects of care but also preferences and wishes on social aspects of care and future meaningful daily activities. This approach enables users to have ACP conversations that include broader range of content or topics. As advocated by the public health approach in palliative care, these broader conversations about what matters most can allow people with dementia and family caregivers to thoroughly reflect and talk about their values and wishes. These conversations can serve as a valuable starting point for more detailed and specific conversations and decision-making about medical aspects of care such as treatment preferences.7,55
Additionally, unlike other ACP web-based tools or interventions that primarily focused on completing advance directives or centred on professional settings,27,56 our website promotes ACP conversations within the family context by providing people with dementia and family caregivers with information and giving them the opportunity to engage in ACP either by themselves or together. Nevertheless, the ACP support website also acknowledges the importance of discussing ACP with health professionals, as it also encourages users to reach out to their health professionals and address ACP with them. This link to health professionals may enable the ACP support website, which is designed to primarily be used in the family context, to serve as a complement to ACP conducted with health professionals in a medical context.
Furthermore, the ACP support website deviates from the standard linear navigation pathways found in other web-based tools to support ACP. Previous web-based ACP tools developed for the general public typically follow predefined steps, starting with the provision of information, prompting reflections, moving on to communication, and ultimately concluding with the completion of advance directives or other forms of documentation. 33 However, research has shown that ACP readiness plays a pivotal role in the ACP process.57–60 The optimal timing of conversation about future care can be a subject of distinct divergence between people with dementia and family caregivers.4,61 While some people with dementia can wish to have such discussions immediately after diagnosis, others often perceive ACP as an emotional and complex process and prefer to ‘live in the present’ and focus on their current capabilities. 6 The diverse views on the ideal time to initiate ACP conversations depending on readiness levels have been shown to be significant barriers to ACP initiation by health professionals.4,62,63 The non-linear, flexible navigation of the ACP support website allows people with dementia and family caregivers to engage in the process accordingly to their needs and readiness level. Users can select which section of the website they would like to use, without having to go through the rest of the website. Moreover, people with dementia and family caregivers can pause and return to the website as they wish.
Participants in our study had positive ratings for the usability of the ACP support website. We found that usability was influenced by factors such as text length, formulation of content and the incorporation of media such as videos. People with dementia and family caregivers encountered some difficulties with the use of the interactive communication tools particularly. Our participants also noted that people with dementia could face challenges using the website independently. It should be noted that our participants were predominantly under the age of 65, and living with mild to moderate dementia. None of the people with dementia were in the more advanced stages of dementia, however, family caregivers of people in the advanced stages of dementia took part in the study. Thus, challenges in the use of the website may be either due to varying levels of digital skills or due to the cognitive decline associated with dementia. Therefore, the ACP support website may not be usable by all people with dementia, or they may require further assistance to use it as the condition progresses. This raises issues such as digital literacy or access to a family caregiver to assist with the ACP support website. Furthermore, users could (over)rely on family caregivers’ abilities, potentially creating a burden to family caregivers. 64 To attempt to address these difficulties, we included tutorial videos to explain how to use the communication tools visually and support the use of the website. However, the strength of our approach lies in its evidence- and theory-based, user-centred and iterative development process. The iterative user-centred approach included the perspectives of people with dementia, family caregivers and different stakeholders in all stages of the development from content specification to creative design. We actively involved people with dementia and their family caregivers, following recommendations of previous research and organisations groups such as Alzheimer Europe,12,19,65 which emphasise the importance of user input in the development of technology and interventions for people with dementia. Our development process also incorporated insights from regional stakeholders and experts, ensuring that the ACP support website also aligned with their values and interests, thereby helping facilitate the website's reach. We adopted a unique development process based on several approaches such as the MRC framework for the development of complex interventions, 29 a process map for the development of web-based decision support interventions, 28 and the scrum method 32 rooted in agile development and user-centred approaches. This combination of approaches allowed us to provide a thorough description of both the content specification and creative design phases of the ACP support website development process. Furthermore, the development of the content of the website was grounded in theory. We aligned website outcomes and content with established theories and explicitly selected theoretical change methods, thereby taking steps towards ensuring a well-founded intervention. 66 These strengths enhance the relevance and potential for implementation and dissemination of the ACP support website.
However, there are limitations that need to be considered. The user group of people with dementia was smaller than the group of family caregivers. This was due to considerable challenges in recruitment in sprints 2 and 3 especially, where people with dementia represented only a third and a quarter of the samples. In addition to the usual recruitment challenges typically encountered when including people with dementia or people with cognitive impairment in research, 67 multiple other factors may have contributed to the lower inclusion rate of people with dementia. Firstly, the sensitivity of the topic of ACP may have discouraged some people from participating in our study. Furthermore, participation in this study implied using a computer or a tablet, which are tools that are potentially not well mastered by some people with dementia or their family caregivers. Limited access to an appropriate device to use the ACP support website may have prevented eligible individuals from participating in the study and may have excluded people with dementia and family caregivers who may have benefited from the ACP support website, highlighting an important limitation in terms of the population the website can reach. Finally, the recruitment period coincided with the COVID-19 pandemic which proved very challenging.
For future research, our study can be an example in terms of development methods for web-based tools targeting people with dementia and their family caregivers. We recommend establishing early collaborations among researchers, software developers, regional stakeholders and end users from the start of the project. Such a collaborative approach increases the chance that web-based tools that are well-suited for their intended purpose and enhances the potential for successful implementation and sustainability. Regarding the ACP support website itself, a thorough evaluation study on the website's acceptability, feasibility and potential effectiveness in engagement in ACP is necessary. This evaluation is currently being conducted. 68 Potential handover of the website to a regional association will also be discussed to ensure sustainability.
Conclusion
This study presented the development of a website to support ACP in the family context for and with people with dementia and their family caregivers. The iterative, user-centred approach incorporated insights from people with dementia, family caregivers and regional stakeholders. The ACP support website's distinctive ‘what matters most’ approach; its nonlinear and flexible navigation; and its innovative user-centred, evidence- and theory-based development process based on a unique combination of approaches set it apart from previous web-based ACP tools. While usability was generally positively rated, challenges with the interactive communication tools provided on the website highlight the need to address digital literacy and accessibility. Future research will focus on the evaluation of the ACP support website, including its acceptability, feasibility and effectiveness to facilitate engagement in ACP.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241304018 - Supplemental material for A user-centred website to support advance care planning for people with dementia and their family caregivers: Development and usability study
Supplemental material, sj-docx-1-dhj-10.1177_20552076241304018 for A user-centred website to support advance care planning for people with dementia and their family caregivers: Development and usability study by Fanny Monnet, Charlèss Dupont, Lara Pivodic, Tinne Smets, Aline De Vleminck, Chantal Van Audenhove and Lieve Van den Block in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076241304018 - Supplemental material for A user-centred website to support advance care planning for people with dementia and their family caregivers: Development and usability study
Supplemental material, sj-docx-2-dhj-10.1177_20552076241304018 for A user-centred website to support advance care planning for people with dementia and their family caregivers: Development and usability study by Fanny Monnet, Charlèss Dupont, Lara Pivodic, Tinne Smets, Aline De Vleminck, Chantal Van Audenhove and Lieve Van den Block in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076241304018 - Supplemental material for A user-centred website to support advance care planning for people with dementia and their family caregivers: Development and usability study
Supplemental material, sj-docx-3-dhj-10.1177_20552076241304018 for A user-centred website to support advance care planning for people with dementia and their family caregivers: Development and usability study by Fanny Monnet, Charlèss Dupont, Lara Pivodic, Tinne Smets, Aline De Vleminck, Chantal Van Audenhove and Lieve Van den Block in DIGITAL HEALTH
Supplemental Material
sj-docx-4-dhj-10.1177_20552076241304018 - Supplemental material for A user-centred website to support advance care planning for people with dementia and their family caregivers: Development and usability study
Supplemental material, sj-docx-4-dhj-10.1177_20552076241304018 for A user-centred website to support advance care planning for people with dementia and their family caregivers: Development and usability study by Fanny Monnet, Charlèss Dupont, Lara Pivodic, Tinne Smets, Aline De Vleminck, Chantal Van Audenhove and Lieve Van den Block in DIGITAL HEALTH
Footnotes
Acknowledgements
We would like to thank all study participants who took part in the usability testing of the different prototypes. We also thank the members of our advisory group, as well as the Mindbytes team for their efforts to develop, build, and refine the ACP support website.
Contributorship
Study concept and design: All authors. Acquisition of data: CD. Analysis and interpretation: FM and CD. Drafting of the manuscript: FM. Critical revision of the manuscript: All authors. All authors gave final approval of the version to be published.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study received approval from the medical ethics committee of Brussels University Hospital of the Vrije Universiteit Brussel on 26 June 2021 (BUN: 1432021000437), and all participants provided written informed consent.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is part of DISTINCT: ‘Dementia: Intersectorial Strategy for Training and Innovation Network for Current Technology’, which has received funding from the European Union’s Horizon 2020 research and innovation programme under the Marie Skłodowska-Curie grant agreement No. 813196. It is also part of the project ‘CAPACITY: Flanders Project to Develop Capacity in Palliative Care Across Society’, a collaboration between the Vrije Universiteit Brussel, Ghent University, and the Catholic University Leuven, Belgium, which is supported by a grant from the Research Foundation – Flanders, file number S002219N. This work was supported by the ‘Wetenschappelijk Fonds Willy Gepts of the UZ Brussel’. LP was a Senior Postdoctoral Fellow of the Research Foundation-Flanders (FWO, 2021-2023). ADV is a Senior Postdoctoral Fellow of the Research Foundation-Flanders (FWO). LVdB is Francqui Research Professor (2020-2023).
Guarantor
FM
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.