
Abstract
Background
Web-based tools (e.g., websites, apps) for people with dementia and their family caregivers may be useful in supporting advance care planning (ACP). Using a user-centred design approach, we developed an ACP website for people with dementia and their families. This protocol describes how we will test and evaluate the ACP website. Publishing a study protocol can guide others who want to evaluate web-based tools. Moreover, the data collection methods used in this study are very innovative since they aim to involve people living with dementia without overburdening them.
Methods
We will conduct an evaluation study of the ACP website in Flanders, Belgium, using a convergent parallel mixed methods pre-post-test design with continuous follow-up. Thirty eligible dyads of people with mild to moderate dementia (both early and late onset) and their family caregivers will use the website in their everyday life for 8 weeks. We will evaluate the usage, usability, acceptability, and feasibility of the website, as well as the experiences of users. Additionally, we evaluate the effects of using the website on ACP readiness, ACP knowledge, attitudes, perceived barriers to engage in ACP, self-efficacy and skills to engage in ACP
Results
Recruitment and data collection is foreseen between end of 2022 and 2023.
Conclusion
This evaluation study of an ACP website for people with dementia and their family caregivers will be the first to evaluate how a web-based tool can support people living with dementia and their families in ACP. The strength of this study lies in the combination of interviews, surveys, and ongoing data logging, which provide insights into the use of support tools in people's daily context. We expect that recruiting people with dementia and their families will be difficult so we have set up a thorough strategy to reach the anticipated sample size.
Background
Because of the progressive cognitive and functional decline in dementia, considering and engaging in discussions about potential health changes that may occur is very important.1–3 The process of thinking and talking about wishes and goals when one's health changes is called advance care planning (ACP). ACP enables people to identify their values, define goals and preferences for future medical treatment and care, and discuss this with healthcare professionals and families. 4 The concept of ACP has transitioned from a physician-driven process focused on documentation and advance directives to a broader concept of ongoing communication about future care and treatment preferences. Recently, ACP has been broadened further by reframing ACP as a health-promoting activity through public education and engagement. This public health approach to ACP underlines the importance of having conversations about future care and end-of-life preferences within the medical context but also within the family context.5–7 Though, most interventions to facilitate ACP are aimed at supporting healthcare professionals.8,9 Research has shown that people with dementia and family caregivers also want to discuss their values and preferences for future care outside of the professional context with their family.10–13 Web-based tools may help support people with dementia and their families to engage in ACP in the family context, but this has not yet been explored.14,15
The number of web-based tools for people with dementia, such as websites and apps, has increased considerably over the years. Such tools offer promising solutions for meeting several of their needs16,17 – for instance, supporting reminiscence or aiding daily activities like managing time. 18 Generally, people with dementia and their families are enthusiastic and optimistic about using technologies to facilitate their independence and support their care needs. 19 Most web-based tools have interactive features that allow tailoring of content to user needs, 20 which is an advantage for people with dementia – as their abilities and needs, and their family caregivers’ needs, change constantly during the disease trajectory.21,22
We have developed an evidence-based, theory-informed, and user-centred ACP website for people with dementia and their families. First, we identified existing evidence on web-based ACP tools and defined the content of the ACP website with family caregivers and dementia experts. 23 Next, we developed the ACP website using the SCRUM method, which emphasises the role of feedback loops. 24 To improve the ultimate uptake of new interventions – such as our ACP website – by end-users, it is essential to systematically evaluate them before they are implemented. In the evaluation study of the ACP website, we aim to evaluate the usage, usability, acceptability, feasibility (i.e., uptake), and effects of the website, explore the experiences of people with dementia and their family caregivers in using the website and explore the similarities and differences among people with dementia and family caregivers regarding usage, usability, feasibility, acceptability, experiences, and effects.
In this article, we describe the protocol of the evaluation study. Publishing a study protocol improves transparency in conducting and reporting research studies. 25 Moreover, it helps readers understand the conducted study better, allows the possibility of replicating the study, and facilitates applying the results in practice. 25 More specifically, the combination of data collection methods used for this study is innovative. We will use log data, online pop-up in-the-moment questions, surveys, and interviews. Our approach enables the involvement of people living with dementia without asking them to recall or document their usage throughout the study. This is particularly important considering the challenges associated with memory recall for people with dementia and the potential burden of maintaining a detailed usage diary. 26 This protocol is written using the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) checklist for reporting protocols. 27
Methods
Study design
We will perform an evaluation study, using a convergent parallel mixed methods pretest-post-test design, with additional data collection that is done continuously. Our design will simultaneously collect quantitative and qualitative data. We will conduct quantitative and qualitative research concurrently (i.e., convergent mixed methods design) to address all research questions. In this design, quantitative and qualitative data are analysed independently, and integrated at the point of interpretation. Previous research among family caregivers and health professionals, 23 and studies on web-based ACP interventions,28–30 have shown that people with dementia and their families wish to engage in ACP at their own pace. 23 Hence, we estimated that an 8-week period would be a long enough time frame to allow participants to use the website.
At the start of the study, participants were given the link to the website so that they can use it at home. We will conduct an interview and survey prior to the 8-week intervention period for the baseline pre-test data collection (T0), and another survey and interview after the 8-weeks for the follow-up post-test data collection (T1).
Setting and participants
The study will take place in Flanders, the Dutch-speaking part of Belgium. Several types of advance directives are established in Belgium, and policy efforts have been made to promote ACP. Although ACP has been advocated in Belgium for over 20 years, there are no up-to-date numbers on the prevalence of ACP in dementia. Moreover, there have been evidence-informed initiatives to promote ACP for nursing home residents, including people with dementia,31–35 but not for people with dementia living at home. We will recruit people with mild to moderate dementia (both early and late onset) and their family caregivers as dyads, or the family caregiver alone. This study will be carried out in the participants’ homes or another place of their preference, and participants can use their own devices (e.g., computers, tablets, phones, etc.) to access the website. We used the following eligibility criteria:
For people with dementia and family caregivers:
Having an interest in and being willing to test the ACP website Being able to consent to study participation Speaking and understanding Dutch Having a device (laptop, iPad, mobile phone, etc.) Did not participate in the cognitive testing of study materials Person living with dementia: being diagnosed with young- or late-onset dementia Family caregiver: takes active care (physical, emotional, social, etc.) for the person with dementia Dyads: Although the website has a text-to-speech option, to be able to use the website and text-to-speech, one of the participants needs to be able to navigate the website (e.g., the person with dementia and the family caregiver cannot both have visual impairments or other disabilities that prevent them from interacting with the ACP website).
General procedures for the evaluation study
A timeline for the participants is shown in Figure 1. Prior to the 8 weeks, participants will receive an information letter. All data collection happened individually e.g., per dyad or family caregiver in the participants’ homes (or whatever location the participant preferred) so participants did not have to travel. When a participant indicates that they wish to participate in the study, the researcher will schedule an appointment to conduct the informed consent, T0 interview, survey, and onboarding. During the 8 weeks, there is an ongoing activity registration of the ACP website's use (logging), a reminder call at 4 weeks and ongoing (technical) support when needed. After 8 weeks, participation in the study is concluded with a T1 survey and interview.
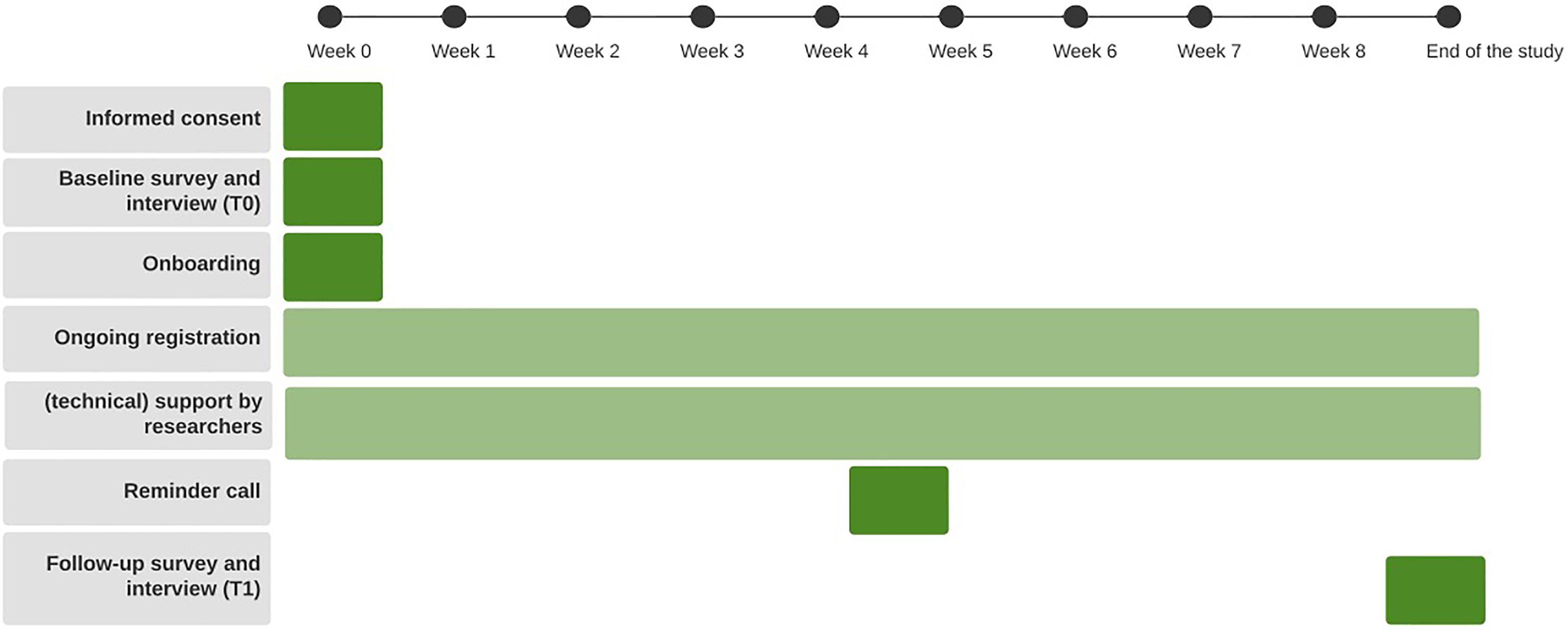
Participant timeline.
The ACP website
The ACP website is designed to inform people with dementia and their family caregivers about ACP and to support them in the ACP process. The website was iteratively developed using a user-centred design. First, the content of the website was defined by a user-needs assessment. Afterwards, four prototypes were presented to people with dementia, their families, and a patient and Patient and Public Involvement group. The website was continually adjusted according to the feedback received. The website aims to improve people's knowledge of ACP, attitudes toward ACP, self-efficacy to start ACP, and skills for engaging in ACP. The ACP website contains several sections: a section about what ACP is and its legal frameworks, a section focused on providing support for people on how to talk about ACP and a section about the existing possibilities to document ACP decisions. The website contains two interactive tools to support people in thinking and talking about their wishes and preferences (including a digital version of the GoWish cards adapted for use in Flanders, 36 a glossary, a frequently asked questions (FAQ) page, a search functionality, a resource and contact page, and a page with information on the website developers and the aim of the website. The website includes special functionalities, such as an option to adjust the text size, choose a different colour contrast, read the text out loud (i.e., speech-to-text function), and the possibility to print (sections of) the content.
Informed consent procedure
Informed consent will be obtained before including potential participants in the study. We will follow the recommendation of the Alzheimer's Association National Board of Directors (2004) by using a double-consent method: consent for the patients’ participation is signed by both themselves and their caregiver (who functions as ‘witness’). 37 Therefore, we will ask the family caregiver to sign the consent form with the participant with dementia. Moreover, the researcher, a nurse with experience working with people with dementia, will explain the research and procedures and will ensure that participants with dementia understand the study and their rights by discussing the statements formulated in the informed consent form with them and the family caregiver. Individuals interested in participating in this study will receive an information letter and an informed consent form. Potential participants are asked to indicate interest if they want to participate in the study. When people indicate they want to participate, an onboarding session will be planned in which informed consent will be obtained, and the website and the study are introduced.
Onboarding session
After receiving informed consent, the researcher will start the onboarding. This consists of introducing the website and giving the participants access. Since the website is not yet publicly available, participants will be able to access the website through a personal link and a participant number. During the onboarding, participants are shown how they can find and access the website and what is on it, and the researcher will ask them to use the website as they see fit. Moreover, the participants will be informed that they can use the website alone or with their family caregiver. Every time the participants visit the website, they are asked to enter their unique participant number and indicate who is using it (person with dementia, caregiver, dyad). In week 4, the research team will call the participants and ask whether they have been using the website and/or need help, schedule the follow-up session and underline that they have the flexibility to cancel or reschedule if the person with dementia is not feeling well or has a challenging day. The ACP website is in a beta phase of development (i.e., testing with the target audience before dissemination/release), and there will be technical support available from the research team. This support is active throughout the study and can be reached via e-mail or phone. The study number, website name, and technical support contact details are summarised on a small support note.
Sample size
The number of participants in the study was chosen based on the sample sizes in previous similar evaluation studies of interactive, web-based tools with heterogenous (non-stratified) populations aimed at evaluating usability and feasibility (22, 27–30). For a full understanding of the usability and feasibility of our website, we aimed mainly to include a sample with sufficient variabilities, i.e., to have people from different age groups, gender, type of dementia, and dyad composition. To achieve this variability, we have estimated needing 30 participants, of which 80% are dyads.
Recruitment
Participants will be recruited via organisations involved in dementia (care), neurologists working in memory clinics, and individual GPs. We will ask the health professionals to select potential participants who might be interested and eligible for this study. Additionally, we will launch a recruitment call, allowing potential participants to contact the researchers directly if they want to participate in the study.
To announce the study, we will ask different organisations, such as the Flemish Alzheimer Liga, day centres, dementia cafes, Belgian health insurers, and individual healthcare professionals and GPs to help recruit via their networks by, for example, contacting patients/clients (e.g., people who have said they want to be involved in studies such as these), e-mail, their member magazines, newsletters, brochures, and/or their websites. The researchers will provide the organisations involved and individual healthcare professionals with a template for a call for participation. Additionally, we will also recruit, via memory clinics, neurologists who will introduce the study to dyads they think are eligible to be included in this evaluation. When dyads are interested in the study, the neurologist will ask the potential participants to contact the researcher or see the researcher directly when s/he is in the hospital. Interested potential participants will receive an information letter and consent form. If one still wants to participate after reading, the researcher will make an appointment with the participant(s) for inclusion. Recruitment is foreseen between the end of 2022 and 2023.
Outcome measures
Socio-demographic and clinical variables
Socio-demographic data (age, gender, education level, marital status, occupational status), computer literacy, and clinical factors (type of diagnosis, time since diagnosis, comorbidities) will be collected using a study-specific questionnaire (Appendix 5). We will also assess the quality of the dyad relationships utilising the quality of caregiver-patient relationships scale. 38 Moreover, post-intervention we will ask the participants if, and how often, they have contacted their healthcare professionals about ACP.
Usage
Usage is defined as the way people with dementia and family caregivers use the ACP website, which will be measured using log data. The results of the participants’ usage within and across each usage session over the 8 weeks of home use will be described in detail to examine usage patterns – and more precisely:
What pages do the people with dementia and the family caregivers visit, what content or functions do they watch or use, and what do they look for when using the search bar? Do they use the interactive elements of the website? and how often do they use them? Do they use the three accessibility features (i.e., text-to-speech feature, option to enlarge the text, and contrast option), and how often do they use them?
Usability, acceptability, and feasibility of the website
Usability in this study is the participants’ evaluation of the user interface. Usability is evaluated by the System Usability Scale questionnaire, a semi-structured interview on their evaluation of the website interface, and 3 pop-up, in-the-moment questions.39,40
Acceptability is defined as the perceptions of people with dementia and their family caregivers of the appropriateness of the content, its delivery, and the format of the ACP website. 41 Acceptability will also be assessed through a post-intervention interview. The website is deemed acceptable if the majority (>70%) of participants evaluate the use of the website as an overall acceptable and positive experience. 41 The interview will address the following seven constructs of the Theoretical Framework of Acceptability 41 : affective attitude (i.e., how the participants feel about the website), burden (the perceived amount of effort that is required to use the website), ethicality (the extent to which the intervention has a good fit with the participants’ value system), intervention coherence (the extent to which the participants understand the ACP website and how it works), opportunity costs (the extent to which benefits or values must be given up to use the website), perceived effectiveness (the extent to which the ACP website is perceived to achieve its purpose), and self-efficacy (the participants’ confidence that they can use the ACP website). 41 The participants will also be shown two pop-up, in-the-moment questions to assess acceptability – (1) ‘I find the website easy to use’, and (2) ‘I find the information on this website clear’ – with answer options on a 5-point rating scale, with 1 = totally agree and 5 = totally disagree. These questions will also include an open-ended item – “can you explain why you have given this score?” – asking for suggested improvements. These questions pop up after 30 s when using the website, and are displayed every time the website is re-opened.
Finally, feasibility in this study is defined as uptake: that is, whether people used the website or not, and why. Feasibility will be evaluated using log data and a semi-structured interview with the people living with dementia and their family caregivers.
Experiences using the website
The ‘experience’ is the way using the website goes/happens, and how it makes the participants feel. To evaluate user experiences, the participants will be asked to rate the following pop-up, in-the-moment question: ‘My experience with this website so far is’ on a 5-point rating scale (from very positive, slightly positive, neutral, slightly negative, to very negative), and they will be asked to explain why they gave this rating. Moreover, the participants will be asked post-intervention how using the website made them feel. If the participants indicate that they did not use the ACP website, the reason for not using the website will be evaluated, including how we can improve the website to make it more useable. Furthermore, we will consider any technical issues interfering with the use of the ACP website, because they can be considered barriers to using the website. The calls the participants make to the helpdesk, and the issues discussed, will be recorded in a logbook. The entries in the helpdesk logbook will be evaluated based on the type of issue encountered and if and how the problem can be solved.
Effects on ACP readiness, ACP knowledge, attitudes, perceived barriers to engage in ACP and self-efficacy, skills to engage in ACP
Effect will be the changes in selected outcomes as a result of using the ACP website. To assess the potential effects of the ACP website, we will investigate any possible changes in readiness for ACP engagement via the Dutch 4-item ACP engagement survey. The survey will be administered to people with dementia and family caregivers at both time points (T0 and T1). 42 Moreover, we will assess knowledge (i.e., the range of one's understanding or information); attitude (i.e., a person's positive or negative evaluation of performing a particular action); perceived barriers (i.e., a person's beliefs regarding the potential negative aspects of a particular action); self-efficacy (i.e., the subjective probability that a person is capable of executing a certain course of action); and skills (i.e., an ability or proficiency acquired through training and practice).
We will ask the participants before and after using the ACP website what they think ACP is and their experiences with ACP. The interview will address the following points: (1) what do they think ACP is, and what do they think ACP can achieve; (2) have they ever considered discussing the different elements of ACP with a member of their family (or other close relationship); (3) have they ever discussed ACP, and how, with their family caregiver or with a healthcare professional; and (4) the researcher will also ask them to elaborate on their experiences with conversations about ACP.
Data collection methods
We will conduct both an interview and surveys at the start of the 8-week intervention period (pre-test data collection T0) and after the 8-week intervention period (post-test data collection T1). During the 8 weeks, there will be continuous data collection via logging of user activity on the website, recording technical issues addressed via phone, and the pop-up, in-the-moment questions hereafter called EMA questions (Table 1). Data collection is foreseen between the end of 2022 and 2023.
Overview of research questions and data collection methods.

EMA: ecological momentary assessment; ACP: advance care planning.
Baseline interview (T0)
We will conduct the baseline interview during the onboarding session. In this interview, we will ask the participants about their previous experience with ACP: for example, what they think ACP is and whether they have engaged in ACP before; and if yes, with whom. Interviews will be conducted using a semi-structured interview guide (Appendix 6) and will last about 30 min. Interviews will be held separately (i.e., the person with dementia and the family caregiver are interviewed by themselves), but the participants could also choose to have the interview together.
Baseline survey (T0)
Directly after the interview, we will ask each participant individually to fill in the baseline survey, consisting of questions on. 1 socio-demographic data, clinical factors, the quality of the dyad relationship (5), and 2 their ACP engagement using the ACP engagement survey. 42 Each participant (i.e., the person with dementia or the family caregiver) will complete their own surveys.
Ongoing log data registration and EMA questions
When the participants use the website, log data (i.e., records of the website usage) are collected. Collecting log data can provide information (via log files) on the interaction between the user and the website.
43
It can reveal the patterns regarding how many sections of the website are being used and how often and in which way the website is being used. During the use of the website, questions will pop up at the moment (pop-up, in-the-moment questions) of usage. These so-called EMA (or experience sampling methods) questions will capture real-time data to capture the participants’ behaviour, mood, and activities.39,40 In EMA, participants are asked to respond to ‘in the moment’ questions, which avoids recall bias, making this a valuable tool for people with dementia. The ACP website holds a logging facility for the following events:
Entry – who is using the website (i.e., study ID and the person with dementia, family caregiver, or dyad); Usage – the way people with dementia and family caregivers use the ACP website – for example, watching a video, visiting a webpage, using interactive tools; Evaluation – ‘in the moment’ information on their website evaluation using EMA. The EMA question for feasibility will be related to the page the user is on, shown 30 s after they enter the page. The EMA question for experiences is shown 3 min after the participants start using the website.
Post-intervention interview and survey (T1)
T1 will proceed in the same way as T0. First, an interview will be conducted, which will also ask about experiences with the website. After that, the questionnaires will again be administered individually.
Testing of data collection instruments
We cognitively tested all data collection instruments (the EMA questions, surveys, and interviews) with people with dementia (n = 2) and family caregivers (n = 4). We presented the instruments to people with dementia and family caregivers to understand how potential participants interpret the questions and the instructions used in the evaluation study. We asked them if the questions were clear, understandable, not too difficult, and if the instruments are easy to use. Only some minor details were adjusted, such as the use of words and making sentences shorter. Based on this feedback, the instruments were slightly modified.
Data analysis and reporting
Qualitative data
All interviews will be recorded and transcribed verbatim. All transcriptions will be pseudonymized and analysed via thematic framework analysis on the qualitative analysis software NVivo. First, two researchers (independent coding) will familiarise themselves with the data. Next, they will generate initial codes, identify recurrent patterns and define and name themes. 44 After independent coding, the two researchers will compare their coding, and differences will be resolved in a small group meeting with a third researcher until a consensus is reached for all themes. Subsequently, the two researchers who did the independent coding will separately group all similar or related themes to form thematic categories. This grouping of thematic categories will again be compared and discussed with a third researcher until a consensus for all thematic categories is reached.
Quantitative data
All of the data from the surveys will be analysed using SPSS. Descriptive statistics will be used for participant characteristics, general evaluation, and ACP engagement. We will use linear mixed models to test for differences between pre- and post-intervention outcomes and to identify differences within and across participants. Descriptive statistics are used to analyse the log data and responses to the EMA questions using RStudio. Logs will comprise a time stamp, a unique ID (based on the user's IP address), and what the interaction with the website was (e.g., watching a video, or visiting a page). The EMA responses consist of a unique ID (IP address), the proposed question, and the user's given response.
Integrating qualitative and quantitative results
Because of this study's convergent parallel mixed method design, we will combine the qualitative and quantitative results. 45 In this study, quantitative and qualitative data will be analysed independently and integrated at the point of interpretation to obtain a complete evaluation of the ACP website. If, for example, the qualitative and quantitative results contradict, we will take further steps to try to explain the differences by re-examining the results. 45
Data reporting
When reporting the study's results, we will follow the Transparent Reporting of Evaluations with Nonrandomized Designs statement. The results from the study are expected at the end of 2023.
Ethical considerations
The research protocol was submitted to the Ethical Committee of the University Hospital (UZ) Brussels before the start of the research, and positive advice to start the study was granted by the Ethical Committee (B.UN 1432022000179). Several measures will be taken to protect the research participants and ensure ethical research practices. Thinking and talking about ACP can raise questions or might be distressing. The researcher will monitor the participants’ reactions during all in-person data collection activities and remind them that they can stop at any time. To ensure that the participants can raise questions after the researcher has left, or reach out in case of distress, they will have the option to contact the researchers. The researchers’ contact details will be made available on the ACP website, in the support note, and in the information letter.
Discussion
In this article, we have described the protocol for a study in which we will test and evaluate an ACP website for and with people with dementia and their family caregivers. This evaluation study will provide a detailed understanding of the usage, usability, acceptability, and feasibility (i.e., uptake) of the website and the experiences of people with dementia and their family caregivers in using the website. Moreover, it will provide knowledge on the potential effects of using the website on ACP readiness, knowledge of ACP, attitudes towards ACP, perceived barriers to engage in ACP, self-efficacy and skills to potentially start an ACP conversation.
Through this study, we aim to better understand how the ACP website can support people with dementia and their families in ACP. We will do this by extensively evaluating the effects of the website on people with dementia and their family caregivers’ knowledge of ACP, their attitudes towards ACP, perceived barriers to engaging in ACP, their self-efficacy, and skills to start an ACP conversation, and their intention to engage in ACP. The concept of ACP has changed significantly over time. While initially focused on completing advance directives, the focus has shifted towards an ongoing communication and decision-making process. 4 This process has been highlighted as very important for people living with dementia and their families.1–3 However, conducting ACP in still dementia is challenging. 21 People with dementia and their families experience difficulties in talking about ACP. 12 Because of dementia, they may have difficulties comprehending the concepts involved in ACP. 21 Moreover, though insufficient knowledge about ACP is a big barrier to engaging in ACP,12,46 a recent study on online ACP information for people living with dementia showed online ACP information is often incomplete or even missing. 47 Hence, it is very useful to understand whether and how technology – such as a website and the online information provided – can help support them in the ACP process.
The described methods of this study will also deepen the knowledge of how new interventions, such as ours, can be evaluated for people with dementia and their families. Evaluating new interventions helps one understand what works and needs to be changed to advance uptake in the long run. 48 While necessary for all new interventions, it is especially important for ACP interventions in dementia, since only a handful of interventions have been developed for this population, and even fewer have been systematically evaluated. As far as we know, this is the first study to evaluate a web-based ACP intervention for people with dementia and their families in the family context.
This study has several strengths. First, our research methods were specifically adapted for people with dementia and their families, which is crucial in order to collect high-quality data. We will use a combination of interviews, surveys, and ongoing data logging. The latter allows us to retrospectively examine usage and evaluate in-the-moment experiences without burdening people with dementia to recollect memories. Moreover, when using web log data, we request less data collection, which enables us to collect data more efficiently and ethically. In addition, combining interviews, surveys, and web log data can give a complete and accurate picture of how people use the ACP website, which can help us optimise it. 43
At the same time, this study also has some challenges. First, we expect to have some difficulties recruiting people with dementia and family caregivers and reaching the anticipated sample size. Previous research shows that recruiting people with dementia and their families can be challenging, especially in studies about end-of-life care communication. 49 In the past, recruiting people living with dementia and their families has been difficult because they do not want to discuss their future and do not have time to participate in research. 49 Moreover, since people living with dementia have relatively low care needs in the early stages of the disease, the population cannot be recruited via a single site, such as a hospital. Therefore, we chose various recruitment strategies to reach as many participants as possible. In this study, we did not calculate a sample size. We thoroughly considered and decided on our sample size and consulted similar studies, we did not calculate a sample size. We aim to evaluate the website, not find differences between groups. Moreover, to facilitate participation, we have tried to eliminate known barriers to participation in research studies, such as the travel distance to the study site.49,50 Furthermore, it is important to note that potential participants may have been unintentionally omitted due to the inclusion criteria requiring owning a device. Introducing a new device can present challenges and impose additional barriers to participation. Additionally, there may be exclusion of people due to the requirement of digital literacy. Because the use of the ACP website requires a certain computer proficiency, we may have unintentionally missed valuable perspectives from people who lack digital skills or access to digital devices. Therefore the findings of our evaluation study may not fully capture the experiences of those with limited digital literacy.
Conclusion
This study protocol describes how we will test and evaluate an ACP website for people with dementia and their family caregivers. This evaluation study will be the first to systematically evaluate how a web-based tool can support people living with dementia and their families in ACP and will add considerably to the evidence on ACP in dementia and the use of web-based tools to support ACP in the family context. The strength of this study lies in the combination of data collection methods. By combining interviews, surveys, and ongoing data logging the usage and experiences can be evaluated without burdening people with dementia to recollect memories. However, the recruitment of people with dementia and their families hence reaching the anticipated sample size of this evaluation study are expected to be difficult.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by a grant from the Research Foundation – Flanders, file number S002219N. The research presented in this article was carried out as part of the DISTINCT project, a Marie Curie Innovative Training Network (ITN), H2020-MSCA-ITN-2018, under grant agreement number 813196.
Ethical approval
The research protocol will be submitted to the Medical Ethics Committee of the Brussels University Hospital (Vrije Universiteit Brussel) before the start of the research (BUN 1432022000179).
Contributorship
All authors have substantially contributed to the research and approved the published version.
Guarantor
CD.