
Abstract
As future employers, nurse managers are in a key position to assess the correspondence between the competence of graduating nursing students and work life demands. The aim of the present study was to assess the competence of graduating nursing students from the perspective of managers, and analyze the factors linked to it. Among European managers in six countries, a cross-sectional survey design with a convenience sample was applied. Data were collected using the Nurse Competence Scale. The study was reported using the STROBE guidelines. Managers (n = 538, 65.8%) assessed the level of competence of graduating nursing students as good, but there were statistically significant differences between countries. In a multivariable analysis, managers who had a Doctoral/Master's degree and were dissatisfied with the nursing program in their country assessed the level of competence as lower. Overall, graduating nursing students seem to meet the competence demands of current work life rather well. Further research is needed to confirm the connection between the managers’ competence assessment and their individual background factors.
Introduction
The aim of nursing education is to educate a workforce that is able to meet the needs of population health and healthcare systems. 1 However, global health challenges, constant changes in healthcare, and population needs affect the future workforce requirements in different settings, 2 along with nursing curricula, to anticipate and respond to these changes. Therefore, for nursing education, nurse managers’ perceptions are essential, as they have insight into the healthcare system and the challenges facing the nursing profession, working on a daily basis in human resource management at all healthcare levels, 3 summing up the required competencies as they conduct recruitment of new nurses, staff development, and retention strategies. 4 Managers are also in a position to shape the design and delivery of new models of care and drive the changes required for their implementation. 5 All in all, as future employers, the managers’ assessments can be used to facilitate the development of the competences of graduating nursing students (GNSs) and to help them succeed with their nursing career. 6 The term GNSs in this study refers to a student studying at the final stage in a nursing degree program leading to the initial qualification as a registered nurse. The term new nurse is defined as a newly graduated nurse working in a first clinical position after graduation 7 and is registered.
In Europe, nursing education is guided by EU directives such as The Professional Qualifications Directive 2005/36/EC and 2013/55EU8,9 and European Qualifications Framework,10,11 which all countries must follow due to the common labor market. Requirements for the training of general nurses is described in the EU directives. Lately, there has been discussion about how these requirements ensure quality in terms of clinical practice. 12 Clinical practice (90 European Credit Transfer and Accumulation System [ECTS]) is a vital part of European nursing education as it comprises half of the general nursing education (180 ECTS). 8 At the time, clinical practice is mostly hospital-based, including highly specialized clinical wards, 12 which can cause challenges for nursing curricula to respond to the needs of several stakeholders, 13 such as different healthcare organizations, communities, patients, and to the changing organizational aspects of nursing care, 14 such as increasing requirements in community and home care. The students’ competence is also influenced by the pedagogical qualifications of their instructors. 12
The debate about GNSs’ competence and its correspondence with work life demands is ongoing.14,15 Debate can be argued for because competence is an important factor connected with desired outcomes, such as safe and quality care. 16 There are global concerns about staff retention,17–19 and the level of competence is related to nurse turnover, including experiences of exhaustion due to a low level of competence.19–21 Moreover, of particular concern is the transition of new nurses into practice, 6 as GNSs are not seen as practice ready,22,23 which might impact on their ability to adapt and manage their duties as registered nurses,15,23 and, ultimately, their willingness to leave the profession. 23 Simultaneously, GNSs are required to work in changing healthcare environments with increasing acuity, patients with various specialized care needs, and cultural variety, along with advances in research and technology affecting patient care. 1
Nurse managers have reported being unsatisfied with the competence of new nurses 6 and they assess GNSs’ competences lower than their educators.24,25 The suggested reason for the lower competence assessments from the managers is that their view is based on what level of competence GNSs should achieve in order to succeed in a particular clinical setting. 24 New nurses are also reported to lack skills in various clinical areas, in both primary and specialized healthcare. 14 In addition, it has been suggested that the development of competence in new nurses benefits from more advanced knowledge and skills14,15,17 and that a structured program for continuing professional development after graduation is needed.6,23 As there appears to be a competence gap between nursing education and clinical practice across different healthcare settings,6,15 more collaboration is needed between healthcare organizations and nursing education to remove the competence gap.13,25 Overall, however, the perspective of nurse managers, as representatives of work life, on the competence of GNSs is rare and has mainly been studied on a national level. 26 In this study, the term nurse manager refers to all levels of nursing management, from nurse managers and nurse leaders (unit level) to nurse directors and executive nurses (middle and strategic levels). 3
The focus of this multi-country study is on the competence of GNSs as seen by nurse managers, representing work life in healthcare. The aims of the study are 1) to assess the competence of GNSs and 2) to analyze the potential factors connected with managers’ assessments. Competence is defined as ‘functional adequacy and capacity to integrate knowledge and skills to attitudes and values into specific contextual situations of practice’. 27 (pp.330–331) The professional competence of GNSs is seen as an outcome of nursing education and nurse managers’ assessments of its comparability with work life demands.
Methods
In this multi-country study, a cross-sectional survey design was applied using the internationally validated Nurse Competence Scale (NCS 28 ). The data were analyzed with univariate and multivariable analyses. The study was reported using the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 29
Setting
This study is an independent part of the large European research project ‘Professional Competence in Nursing’ (ProCompNurse 2017‒2021) funded by the Academy of Finland. 30 The aim was to analyze the quality of the nursing workforce by assessing the professional competence of GNSs in six European countries: Finland, Germany, Iceland, Ireland, Lithuania, and Spain. The participating countries were chosen from different parts of Europe to represent Northern, Southern, and Central Europe. Thus, nursing education in these countries is comparable, even though there are some differences, such as the duration of nursing education from 210 ECTS to 240 ECTS over 3–4 years at either the bachelor or diploma level (Table 1). The main variation is Germany having vocational training for nurses over three years (4600 h). In each country, the managers’ data were collected from geographically different parts of the countries, mainly from university hospitals (total number of hospitals n = 32) providing clinical placements for GNSs.
Nursing education in the participating countries.
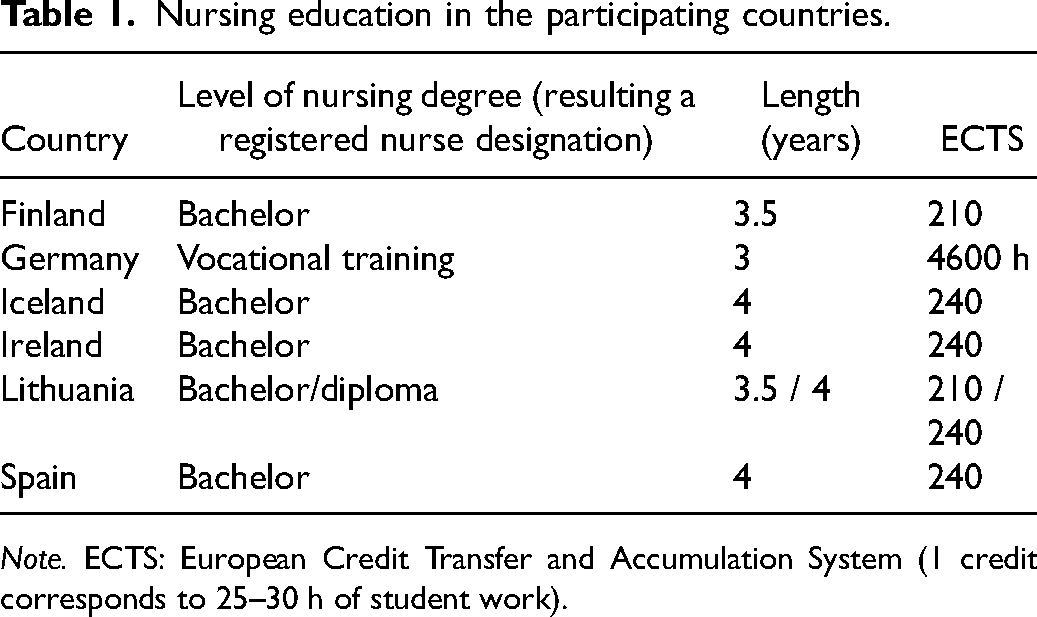
Note. ECTS: European Credit Transfer and Accumulation System (1 credit corresponds to 25–30 h of student work).
Sample
A convenience sample was used in this study. 31 A nurse manager was eligible for the study if she/he 1) had a background qualification as a nurse, excluding managers who had a background either as a doctor/physician or some other health/social care professional, 2) had an official administrative position in healthcare, 3) had daily or almost daily contact with nursing staff, 4) was responsible for/contributed to the recruitment of nursing workforce, and 5) had a position in an organization providing clinical placements for graduating students. In practice, the work title and/or position of the respondents was either Director of Nursing, Nurse Unit Manager, or Assistant Nurse Unit Manager referring to the strategic, operational, and bedside levels of management, respectively. The potential participants meeting the inclusion criteria were identified by national research teams together with named contact individuals assigned by each participating healthcare organization.
Data collection
The data were collected between May 2018 and March 2019 with a survey. The structured survey contained two parts. The first part comprised individual background factors, such as age, gender, education, work experience, and organizational factors such as work title/position, number of subordinates, and the frequency of newly graduated nurses seeking to work in the unit. In addition, as an educational factor, a question was asked about satisfaction with the nursing degree program in the country.
The second part of the survey was the NCS, which is the most widely used validated instrument to measure the generic competence of nurses, and also developed for the use of managers. 28 The NCS includes 73 items divided into seven theoretical categories: helping role, teaching-coaching, diagnostic functions, managing situations, therapeutic interventions, ensuring quality, and work role. Managers assessed students’ competence on a visual analogue scale (VAS; 0–100) where scores <25 indicate ‘low competence’, ≥25–50 ‘quite good competence’, >50–75 ‘good competence’, and >75–100 ‘very good competence’. 28 The option ‘not applicable’ was also available.
Before data collection, the NCS had already been translated and validated in Finnish, English, Icelandic, and Lithuanian. Thus, translations into German and Spanish were conducted using standard double-translations. 32 The questionnaire was piloted in each participating country to analyze the understandability and clarity of the items before data collection. A paper-and-pencil questionnaire was used. In Ireland, an electronic format was also used by applying Research Electronic Data Capture (REDCap) tools hosted at the University of Turku, Finland. Paper-and-pencil questionnaires were delivered to managers in a sealed envelope either by hand or via post by a member of the research team or a contact person named by the organization. Managers returned the questionnaires in a sealed envelope. For the electronic format, an email containing the link to the survey was sent to the managers’ work email address by the local contact individuals.
The survey was distributed to a total of 853 managers. The number of returned questionnaires was 561, with an overall response rate of 65.8% (range, 37.9% in Finland to 96.8% in Germany). However, some questionnaires were returned empty, leaving 538 questionnaires for analysis.
Data analysis
The background variables age, work experience as a manager, work experience in the current unit, and number of subordinates were compared between countries using the Kruskal–Wallis test, followed by the Dwass, Steel, Critchlow–Fligner multiple comparison procedure in pairwise comparisons. The variables gender, level of undergraduate education, level of postgraduate education, work title/position, the frequency of newly graduated nurses seeking to work in a unit, and satisfaction with the nursing degree program were compared between the countries using the chi-square test.
Univariate p-values for total scale were analyzed using two-way analysis of variance (ANOVA) or covariance (when explanatory variable was handled as a continuous variable). All analyses included at least country and one of the following explanatory variables, one at a time: age, gender, level of undergraduate education, level of postgraduate education, work experience as a manager, work experience in the current unit, work title/position, number of subordinates, newly graduated nurses seeking to work in a unit, and satisfaction with the nursing degree program. After the univariate analyses, multivariable analyses were started, including the following explanatory variables: country, gender, level of postgraduate education, work title/position, number of subordinates, and satisfaction with the nursing degree program. The multivariable analyses were continued by removing all insignificant variables from the model.
The subcategories of the scale were compared between the countries using one-way ANOVA followed by pairwise comparisons where p-values were corrected using Tukey's method. Model-based mean and slope estimates from the models are presented.
95% confidence intervals (CIs) were calculated. All statistical tests were performed as two-sided, with the significance level set at 0.05. The analyses were performed using SAS software, version 9.4 for Windows (SAS Institute Inc., Cary, NC, USA).
Ethical considerations
Ethical approval for the entire project was received from the Ethics Committee of the University of Turku (Statement 62/2017, 11 December 2017) and, in addition, according to the national standards in each country. Moreover, research permissions for data collection were granted by all participating healthcare organizations according to their standard procedures. The ethical principles of the Declaration of Helsinki were followed. 33 In an information letter of the survey, managers were informed about the study, voluntary participation, confidentiality, and the right to withdraw at any time without disclosing the reason. Informed consent was also sought in accordance with national standards. Permission to use the NCS was received from the copyright holder. In this study, the EU general data protection regulation (GDPR) was followed. 34 The data were accessed and stored in compliance of the University of Turku Data Security Policy 35 and the Finnish Personal Data Act. 36
Results
Background of the managers
The overall sample consisted of 538 managers (89.9% women; median age 47 years) from six European countries (Table 2). For nearly half (45.0%) of the respondents, the current work title was Assistant Nurse Unit Manager representing the bedside management level. As the basic undergraduate degree in nursing, most of the managers had either a degree from university (46.8%) or a degree from a nursing college or a diploma (43.3%). As a postgraduate degree, a minority of the managers had either a doctoral or master's degree (30.2%), and a majority had other postgraduate education (69.8%), meaning either a bachelor degree, postgraduate diploma, or no postgraduate degree at all. The mean total length of work experience in management was 10 years, of which seven years were in the current unit. The mean number of subordinates was 28. Most of the managers (69.4%) stated that newly graduated nurses seek to work in their unit often or very often. Overall, managers (78.3%) were satisfied with the current nursing education in their country (Table 2).
Background of nurse managers.
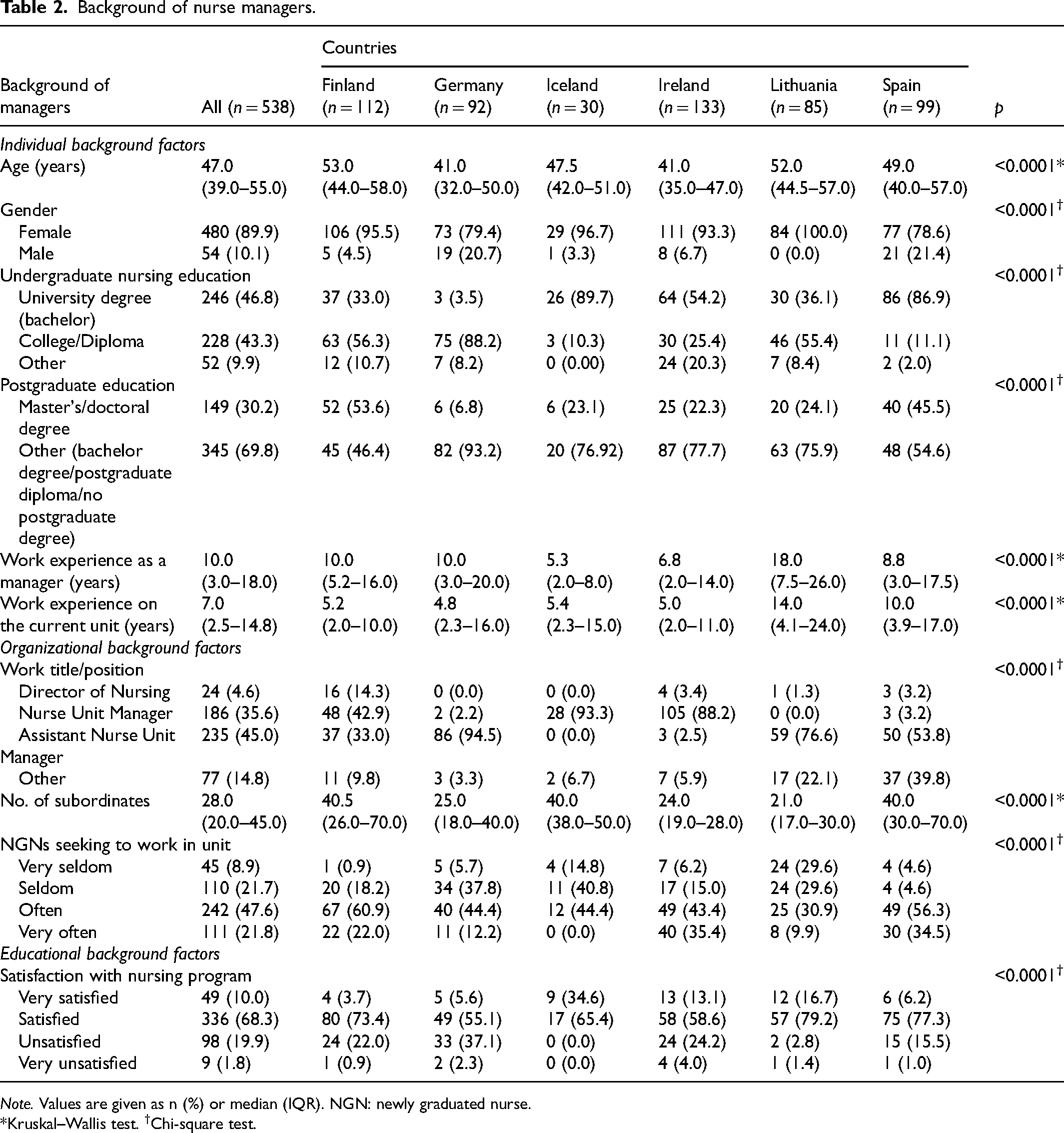
Note. Values are given as n (%) or median (IQR). NGN: newly graduated nurse.
*Kruskal–Wallis test. †Chi-square test.
Managers’ assessments of GNSs’ competence
Overall, the total competence level of GNSs was assessed by the managers as good (mean 58.8 ± 18.8) (Table 3). All subcategories were also assessed at the good level, with the work role getting the highest score (mean 61.5 ± 20.7) and subcategory of teaching and coaching the lowest score (mean 55.9 ± 19.4).
Differences between the countries in the total score of NCS and its subcategories.

Note. DE: Germany; ES: Spain; FI: Finland; IE: Ireland; IS: Iceland; LT: Lithuania; NCS: Nurse Competence Scale.
Adjusted p-values are as follows: *p < 0.05, **p < 0.01, ***p < 0.001. †For the statistically significant differences between means and confidence intervals, please, see above row(s).
There were differences in the assessments between countries. Lithuanian managers assessed their GNSs’ competence level as the highest (mean 75.9 ± 15.6), indicating very good competence. Finnish managers gave the lowest scores (mean 46.1 ± 15.7), indicating that the GNSs in their country had a fair competence level. The differences between countries in the total competence scores and all its subcategories were statistically significant (overall p-value for country comparisons p < 0.0001).
Background factors connected with managers’ assessments of GNSs’ competence
Based on the univariate analysis, the managers’ competence assessment was connected with country (p < 0.0001), gender (p < 0.039), the level of postgraduate education (p < 0.014), number of subordinates (p < 0.023), and satisfaction with the nursing degree program (p < 0.0001) (Table 4). Managers gave higher assessments if they were female and if their postgraduate education was either a bachelor degree, postgraduate diploma, or no postgraduate degree at all. The more subordinates the managers had, the lower were their assessments. Furthermore, the more satisfied the managers were with the nursing degree program, the higher was their competence assessment.
Association of background factors with nurse managers’ assessments of total competence score.
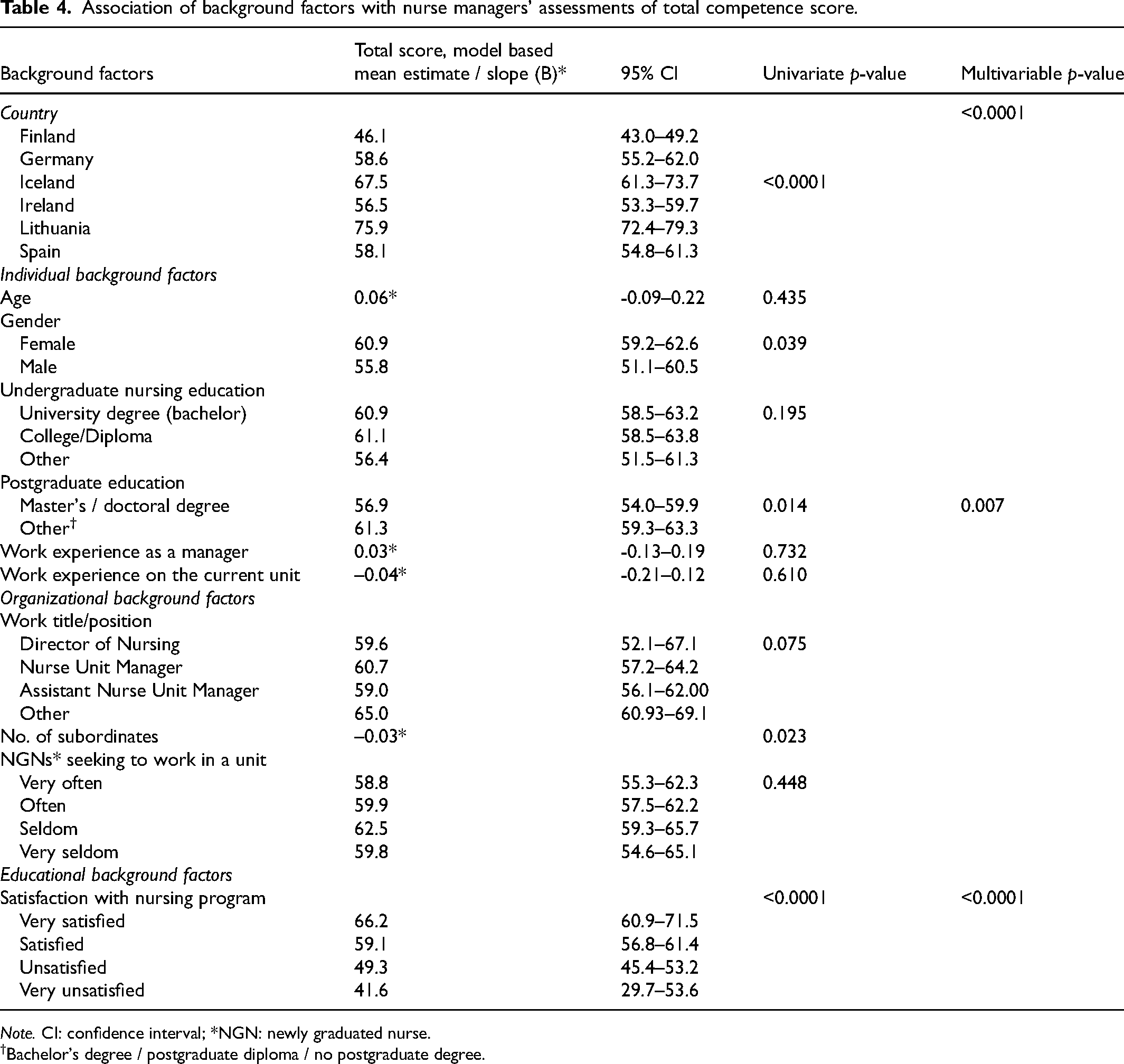
Note. CI: confidence interval; *NGN: newly graduated nurse.
†Bachelor's degree / postgraduate diploma / no postgraduate degree.
The multivariable analysis showed that the background factors connected with the managers’ assessments of students’ competence were country (p < 0.0001), managers’ level of postgraduate education (p = 0.007), and satisfaction with the nursing degree program in the country (p < 0.0001) (Table 4). Managers who had a doctoral/master's degree and who were dissatisfied with the nursing degree program in their country assessed the GNSs’ level of competence as lower.
Discussion
This pioneering European pilot study produced the first exploratory multi-country analysis of the perspective of nurse managers, i.e. work life, on the competence of GNSs. In this study, the GNSs’ competence met the demands of current work life rather well. However, the level of competence only just reached the good level, indicating that the correspondence between education outcomes and work life needs to be further examined. Promoting competence in a collaborative effort between education and work life 18 can be a key to retaining nurses and improving the quality of care 6 at a time when the turnover and shortages of new nurses affect the delivery of care and nursing workforce trends.
In this study, there were differences between countries in the managers’ competence assessments. The assessments varied on overall competence and across competence areas. Previous multi-country studies about nurse managers’ assessments of the competence of GNSs are scarce, but these findings are in line with earlier studies in single countries using the same scale.24,28 As there are differences between the healthcare systems and settings in different countries, such as the level of independence in the work role of nurses 37 and doctor-to-nurse ratios, with countries such as Finland, Germany, and Ireland having the highest number of nurses in the EU, 38 different needs for competences and performance exist. Therefore, nurses’ different responsibilities and tasks in patient care could explain some of the variation in managers’ assessments of GNSs’ perceived level of competence in different countries. 37 Further research is needed to shed light on the possible reasons behind this variation.
The level of GNSs’ competence across different competence areas varied in managers’ competence assessments in participating countries. For example, the lowest level of student competence was assessed by managers in therapeutic interventions in Finland as well as in Spain. In this subcategory, questions were mainly related to nursing interventions, decision-making, and multidisciplinary teamwork. Therapeutic interventions have also been given lower ratings in previous studies using the NCS.39,40 In order for GNSs to be able to make appropriate decisions regarding patient care and respond to patient situations with appropriate actions, they need time and relevant experience to learn these things and develop critical thinking skills. 41 In addition, recent studies suggest that the requirements of clinical skills (also known as technical or psychomotor skills) are increasing in nursing care across different healthcare settings.14,15
Managers in Lithuania, Iceland, and Ireland assessed teaching and coaching as the lowest competence subcategory. The questions in this subcategory were related to patient education along with teaching other professionals and nursing students. Teaching competence including patient education has also been reported as the area of lowest competence in previous studies or a generally less used practice. 42 However, teaching has been recognized as a key component of the nurses’ role and practice,42,43 and new nurses are required to teach patients and their families, as well as students and other professionals, soon after graduation. 43 In Germany, managers assessed ensuring quality as the lowest competence subcategory, in which questions mainly related to the use of research for work or further development. In Germany, research education has not necessarily been a part of the undergraduate programs and managers may therefore have noticed some shortcomings in this area of competence. The integrated support of managers and educators can facilitate students’ learning of research and its utilization. In addition, managers can encourage both students and nursing staff to improve their understanding of the association between research application and care quality. 44 By promoting evidence-based practices as a part of daily practice, it has the potential to improve patient outcomes and the practice environment. All in all, collaboration between nursing education and healthcare organizations is needed to ensure the connection between education and practice, and the adequate transition of new nurses to practice preparation. As nursing education in Europe aims for the training of general nurses, a structured program for continuing education after graduation is needed to ensure the development of more advanced nursing competence in highly specialized clinical areas.
The managers’ competence assessments were connected to satisfaction with the nursing degree program. This supports the idea that employer satisfaction and the employability of graduates indicate the quality of higher education. 45 Still, as employment is almost certain due to the nursing shortage, the nurse managers’ satisfaction as employers is less noted. As for the logical directions, managers in Lithuania, Iceland, and Spain assessed the level of GNSs’ competence highest and were also most satisfied with the current education in their country, while managers in Ireland and Finland assessed the level of GNSs’ competence lower and were less satisfied with their current nursing education. A contradiction between managers’ competence assessments and satisfaction was seen in Germany, where managers assessed the GNSs’ level of competence among the highest but were most unsatisfied with the current nursing education in their country. To conclude, the division of labor in different countries and variations in nursing education, such as Germany having vocational training for nurses, may affect managers’ satisfaction. However, these aspects warrant further research. All in all, as future employers, the managers’ satisfaction with nursing education along with their competence assessments might give important insight into how nursing education succeeds overall in producing the competencies required by work life and could indicate areas that need improvement. However, further study on the topic is needed.
The managers’ level of postgraduate education was also connected with their competence assessments. Consequently, it appears that the higher the level of managers’ education, the more critical their view on competence assessment. The number of managers with a doctoral or master's degree was highest in Finland, and, overall, Finnish managers assessed the competence of their GNSs as lowest. Although not explicitly shown statistically, it is worth pointing out that managers’ organizational background factors – for instance, managers describing their role in the healthcare organization in terms of the number of subordinates – can be interwoven into their competence assessment in the national context. From the perspective of work life demands and recruitment, when considering the duties of executive or director level managers – setting out strategic and system thinking, leading the vision and values in the organization, managing evidence-based practice, demonstrating measurable outcomes, effectiveness, 46 and cost control by planning and allocating staff resources – they might assess GNSs’ competences beyond the unit level, including a wider area of responsibilities and transferability of competences into different settings. 47 On the other hand, unit level managers operate in clinical practice and work with service quality, 48 and thus assess the competence of GNSs in direct patient care at the unit level. In addition, whether competence assessment and performance evaluations are part of nurse managers’ tasks, and whether explicit and tangible career paths for nurses exist in healthcare organizations, might affect managers’ competence assessments in different countries.
Variations in the role and responsibilities of managers in different healthcare organizations might have influenced the assessment of competence along with managers’ expectations towards the competence of GNSs in different countries. Overall, there is limited knowledge regarding the European nurse manager population, and statistical information describing their demographics appears to be unavailable. This also explains something about nursing management education in Europe as there are no uniform qualification requirements for nurse managers. In addition, synthesized knowledge about nurse managers’ competences has been missing. 49 Further studies about managers’ assessments of the GNSs’ level of competence in relation to the competence expectations from managers in different countries are needed. In addition, the level of education of nurse managers in relation to competence assessment and nursing outcomes warrants international research in the future.
Strengths and limitations of the study
A strength of this study is that the managers used an internationally validated instrument to measure the competence of GNSs. 28 In addition, as data were mainly collected from university hospitals providing clinical placements for students and operating as teaching hospitals, managers were assumed to know about the students’ competence because of their experience in arranging clinical placements.
The present study also has some limitations. The first limitation is that the healthcare organizations in this multi-country European study were recruited to the study using convenience sampling. The selection bias was reduced by choosing hospitals across the countries to reach national samples when possible. The second limitation is that despite the joint inclusion criteria, the nurse manager populations were overall very heterogeneous. Undoubtedly, differing samples limit the generalizability of the results although there is little knowledge of the European nurse manager population on the whole and thus of the representativeness of our sample. 50 However, in the present study, all levels of managers were targeted and, as future employers, their competence assessment has its place. Finally, the response rate differed in the different countries, ranging from 37.9% in Finland to 96.8% in Germany. This might have caused some bias, even though research protocol was used in this study to outline data collection and similar samples in each country. 51
Conclusions
From the managers’ perspective, GNSs seem to meet the competence demands of work life. Collaboration between the health service system and nursing education about the correspondence between the outcomes of education and the demands of work life is the key to the GNSs’ competence and transition to a professional nurse. Continuous changes call for constant dialogue between these stakeholders. Some implications for cooperation are to develop common continuing education programs to ensure the development of advanced nursing competence in highly specialized clinical areas, along with utilizing faculty's expertise to ensure the pedagogical qualifications of instructors. In addition, joint evidenced-based nursing practices in education and clinical practice could merge the gap between education and practice. A competence gap can also occur when GNSs’ competence and managers’ expectations or competence needs of the health service system are not met. Therefore, managers’ competence assessments can provide insight into competence and learning the needs of the health service system. Given the heterogeneous sample, further research is needed to confirm the connection between the managers’ competence assessments and their individual background factors, such as level of education. Further research is needed about the population of European nurse managers and their role in different healthcare systems as this might be associated with managers’ evaluation of GNSs’ competence.
Footnotes
Acknowledgments
We thank all respondents for their time and effort to take part in this study. We also thank everyone who has assisted us in the data collection in numerous hospitals in each country. Finally, we thank Katie White who assisted the Irish project team during her Undergraduate Summer Internship in 2019.
Author contributions
HL-K, LS, SK, EL, NF, PF, DL, JS, and HS conceived and designed the study; SK, EL, PK, LS, HL-K, NF, PF, DL, JS, and HS acquired the data; PK, SK, EL, LS, HL-K, NF, PF, DL, JS, and HS analyzed and interpreted the data; PK and SK wrote the first draft of the manuscript; SK, EL, LS, HL-K, NF, PF, DL, JS, and HS commented on previous version of the manuscript for important intellectual content.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Turun Yliopistollinen Keskussairaala, and Academy of Finland (grant no. 11087, 310145).