
Abstract
Nursing education will play an important role in further advancing healthcare transformation in the future. The aim of this study was to assess and compare nursing education and self-reported professional competence among nursing students graduating with a bachelor's degree from higher education institutions in Europe. Data were collected using the Nurse Professional Competence Scale including 88 items and eight competence areas. In total, 752 nursing students at 11 higher education institutions in Europe participated in the study, with a response rate of 88.7%. The highest measured mean scores were found in the competence areas ‘Value-based nursing care’ and ‘Medical technical care’ and the lowest were found in ‘Legislation in nursing and safety planning’ and ‘Education and supervision of staff and students’. Nursing students in central Europe scored significantly higher on seven out of the eight competence areas than nursing students in northern and southern Europe. In order to standardize and further develop nursing education in Europe, the assessment of nursing-related competences is of crucial importance.
Keywords
Background
Introduction
According to the World Health Organization, nurses and midwifes account for nearly 50% of the global health work force. 1 An important aspect in meeting the demands and requirements of societies and their different healthcare systems worldwide is the educational level and competency of nurses. 2 With this in mind, the Registered Nurse Forecasting Study (RN4CAST) (2009–2011), which was conducted in Europe, is of interest.3,4 The study identified both registered nurses having bachelor's degrees, and workload in terms of number of patients cared for to be factors that can reduce preventable hospital deaths. Nursing education therefore plays an important role in preparing the profession as a whole to further contribute towards global health in the future.
Nursing education in Europe
From a historical perspective, Germany, France and Britain have played an important role in developing nursing in the modern age in Europe. In terms of nursing education, Florence Nightingale was influential in developing it into what it is today. 5 In 1999, ministers of education of 29 European countries adopted a vision for a European Higher Education Area (EHEA). One result was the Bologna Declaration 6 that aimed to create a structure of easily comparable degrees within higher education and to facilitate cooperation between universities in Europe. As a result of the Bologna Process, the academic systems of these countries are now based on three cycles of higher education qualifications: bachelor's, master's, and doctoral degrees. 7 Further work has been performed by the EHEA and the European Union (EU) to facilitate the transition from vocational nursing training to university-based training in some European countries. Another goal of the Bologna Process was to support the mobility of students and professionals within countries belonging to the EHEA. 8
In addition, the Bologna process has inspired various initiatives, such as the Tuning Project, which are supported by the European Commission. The Tuning Project, which is a university-driven project, started in 2000 and aims to ‘offer a universal approach to implement the Bologna Process at the level of higher education institutions and subject area’.
9
Of the nine subject areas (Business, Chemistry, Earth Sciences, Education Sciences, European Studies, History, Mathematics, Nursing, and Physics), nursing was the first health profession to take part in the project.
9
The focus within the subject area of nursing was the academic and professional domain of the general nurse. The Tuning Project distinguishes generic and subject-specific competences for all three cycles. The generic competences are: intellectual, professional and academic, and practical competences. The subject-specific competences for nursing comprise five domains, namely: (1) professional values and the role of the nurse, (2) nursing practice and clinical decision-making, (3) knowledge and cognition, (4) communication and interpersonal skills (including technology for communication), and (5) leadership, management, and teamwork.
10
One educational aim for the EHEA was to include academic training within the European concept of Lifelong Learning. In this context, a European Qualifications Framework (EQF) for Lifelong Learning was developed. See Figure 1 where the links between these two frameworks are illustrated.
The relationship between the European Qualifications Framework for Lifelong Learning and the Framework for Qualifications of the European Higher Education Area.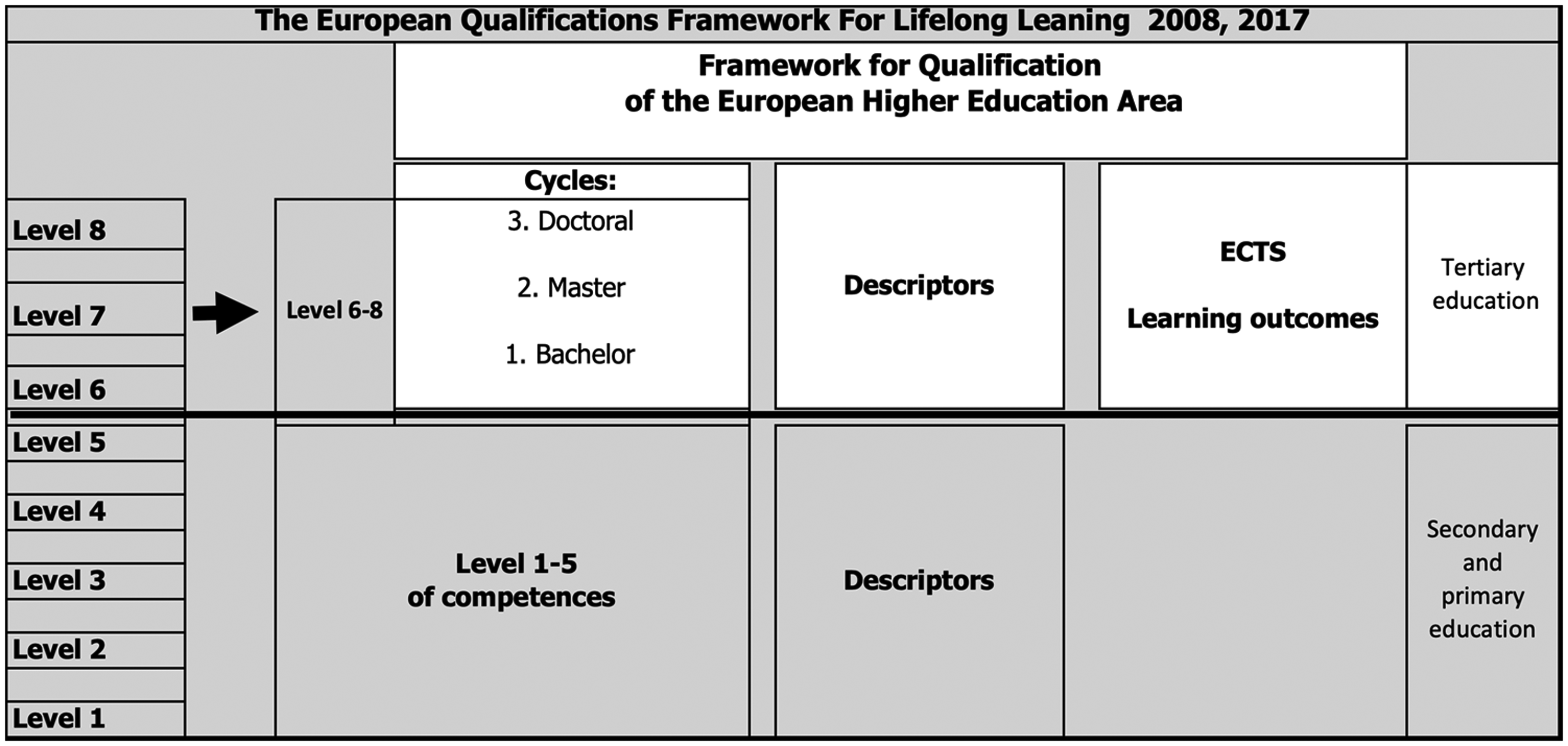
The EQF can be regarded as a meta framework and corresponds to the generic competences mentioned above. Descriptors define the learning outcomes in three domains: knowledge, skills, and competence. 11
In Figure 1, levels 1 to 5 refer to primary and secondary education, whereas levels 6 to 8 refer to tertiary education in Higher Education. Regarding nursing education, two major nursing reform phases have been described at the European level.12,13 This observation has repeatedly been reported also in other studies.14–16 The first reform phase contributed to a unified platform for preregistration programmes for levels 1 to 5, while the second reform phase aimed to contribute to the integration of nursing programmes into higher education, that is, levels 6 to 8. It has been emphasized how this second reform (levels 6 to 8) has led to a growing divergence instead of a convergence of nursing programmes across Europe.
Aim
The aim of this study was to assess and compare nursing education and self-reported professional competence among nursing students graduating with bachelor's degrees from higher education institutions in Europe.
Method
Study design
A cross-sectional multi-centre study was conducted at 11 higher education institutions (HEIs) in six European countries using the Nurse Professional Competence (NPC) Scale 17 with nursing students about to graduate with bachelor's degrees. For cultural, geographical, and linguistic reasons, the participating countries were divided into three regions; northern Europe (Norway and Sweden), central Europe (Austria, Germany, and Switzerland) and southern Europe (Portugal). The collaboration is related to the European Network of Nursing Academies (ENNA e.V.) with the intention to contribute towards quality assessment and quality improvement in nursing education in Europe. To date, ENNA has members in Austria, Germany, Italy, the Netherlands, Norway, Portugal, Sweden, and Switzerland. Researchers from Austria, Germany, Norway, Portugal, Sweden, and Switzerland chose to participate in the present study.
The instrument
The instrument used in this study was the NPC Scale, which originates from Sweden and was developed to measure self-reported professional competence among nursing students graduating with bachelor's degrees and registered nurses with or without a specialization.
17
The NPC Scale is based on Swedish national guidelines and the World Health Organization's European Strategy for Nursing and Midwifery.
18
The Swedish-language version of the NPC Scale has been validated and has shown good validity and reliability in several studies.17,19 The NPC Scale consists of 88 items distributed into eight competence areas (CA):
Nursing care (CA1), e.g. ‘acknowledge the healthy aspects of the patient’ Value-based nursing care (CA2), e.g. ‘communicate with patients, next of kin and staff respectfully, sensitively and empathetically’ Medical and technical care (CA3), e.g. ‘manage drugs adequately, applying knowledge in pharmacology’ Teaching/learning and support (CA4), e.g. ‘provide support and guidance to enable optimal participation in care and treatment, in dialogue with the patient and next of kin’ Documentation and information technology (CA5), e.g. ‘make use of relevant patient records’ Legislation in nursing and safety planning (CA6), e.g. ‘comply with existing regulations as well as guidelines and procedures’ Leadership in and development of nursing care (CA7), e.g. ‘take part in ongoing systematic and documented quality assurance and safety work and continuous improvement work’ Education and supervision of staff and students (CA8), e.g. ‘participate in the supervision of co-workers/staff and students in development work’
Responses to the 88 items are made on a four-point scale (where 1 = to a very low degree and 4 = to a very high degree). The response alternative ‘cannot decide’ was also available. The NPC Scale was translated from Swedish to English 20 and in addition to the original Swedish version, the NPC Scale is currently available in Dutch, English, German, Norwegian, and Portuguese.
Data collection
Data were collected using a convenience sample including nursing students at 11 higher education institutions (HEIs) in Europe belonging to the ENNA network. The NPC Scale was given to nursing students during the final part of their bachelor's nursing degree programme, when the majority of clinical and theoretical elements had been completed (October 2015 to June 2017). The total response rate was 88.7% (northern Europe 96.3%, central Europe 86.8%, and southern Europe 86 %). In addition to the NPC Scale, a questionnaire was sent to one contact person representing the research team at each participating HEI. The questionnaire included questions addressing the following areas of the nursing programmes: name of the programme, level, cycle, length (duration), European Credit Transfer System (ECTS), construction of the programme (full-time/part-time study), name of the bachelor's degree, professional title, and internationalization.
Analysis of the data: Statistical measures
Reliability of the Nurse Professional Competence Scale per region and competency areas (CA).

Ethical considerations
This study was conducted according to the ethical principles of the Declaration of Helsinki. 21 Permission to collect data from the nursing students was obtained at each HEI in each respective country following their local and national ethical guidelines. Eligible nursing students received verbal and written information about the study at each HEI. The information focused on the voluntary nature of participation, their informed consent, that answering the questionnaire would be carried out anonymously, and that no student information that could be identified would be collected. Results based on the collected data are presented at group level to further ensure participants' anonymity. By completing and returning their response to the NPC Scale, participating nursing students gave their informed consent. The responsible researchers at each participating HEI have stored the data according to their specific ethical regulations.
Findings
The findings consist of the analysis of: (1) comparing nursing education programmes at the different HEIs in Europe, and (2) self-reported competence among nursing students graduating with bachelor's degrees in Europe.
Comparing nursing education programmes at the different HEIs in Europe
Health indicators of the participating countries in the study.
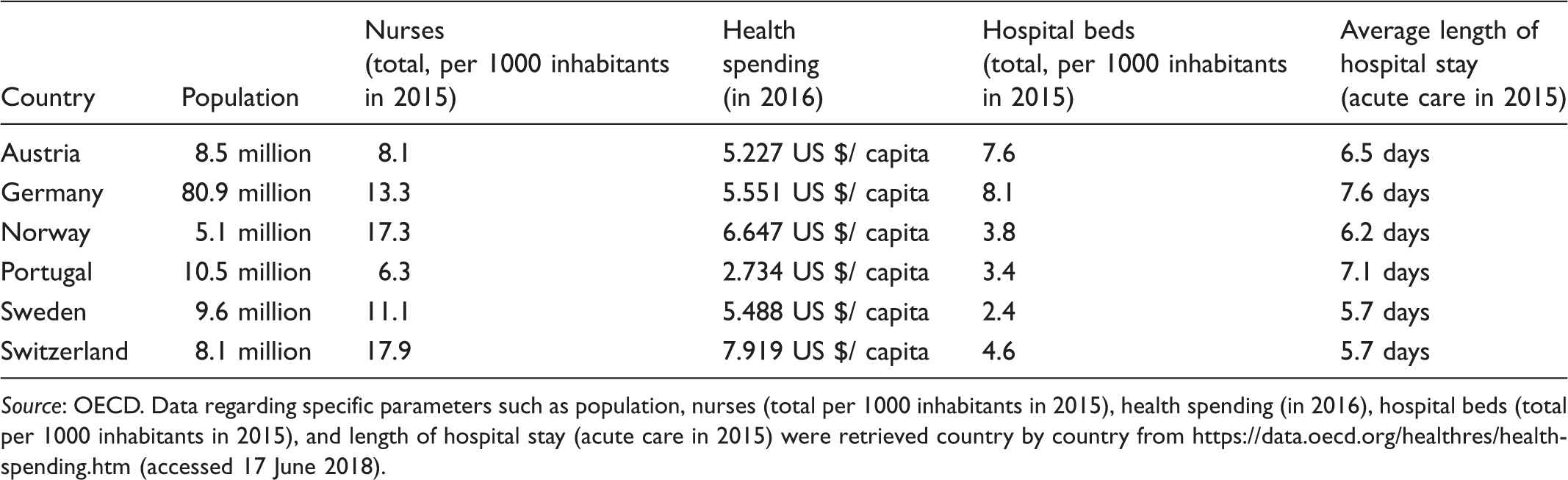
Source: OECD. Data regarding specific parameters such as population, nurses (total per 1000 inhabitants in 2015), health spending (in 2016), hospital beds (total per 1000 inhabitants in 2015), and length of hospital stay (acute care in 2015) were retrieved country by country from https://data.oecd.org/healthres/health-spending.htm (accessed 17 June 2018).
Of the six countries participating in this study, Germany has the largest population with 80.9 million inhabitants, while Norway has the smallest population with 5.1 million inhabitants. Regarding the number of nurses per 1000 inhabitants, Switzerland has almost three times more nurses per 1000 inhabitants than Portugal. Similar findings are found for health expenditure. The number of hospital beds per 1000 inhabitants is highest in Germany and lowest in Sweden. There is a variation in the average length of hospital stay ranging from 5.7 days in Switzerland and Sweden to 7.6 days in Germany.
Structure of the nursing programmes at participating HEIs.
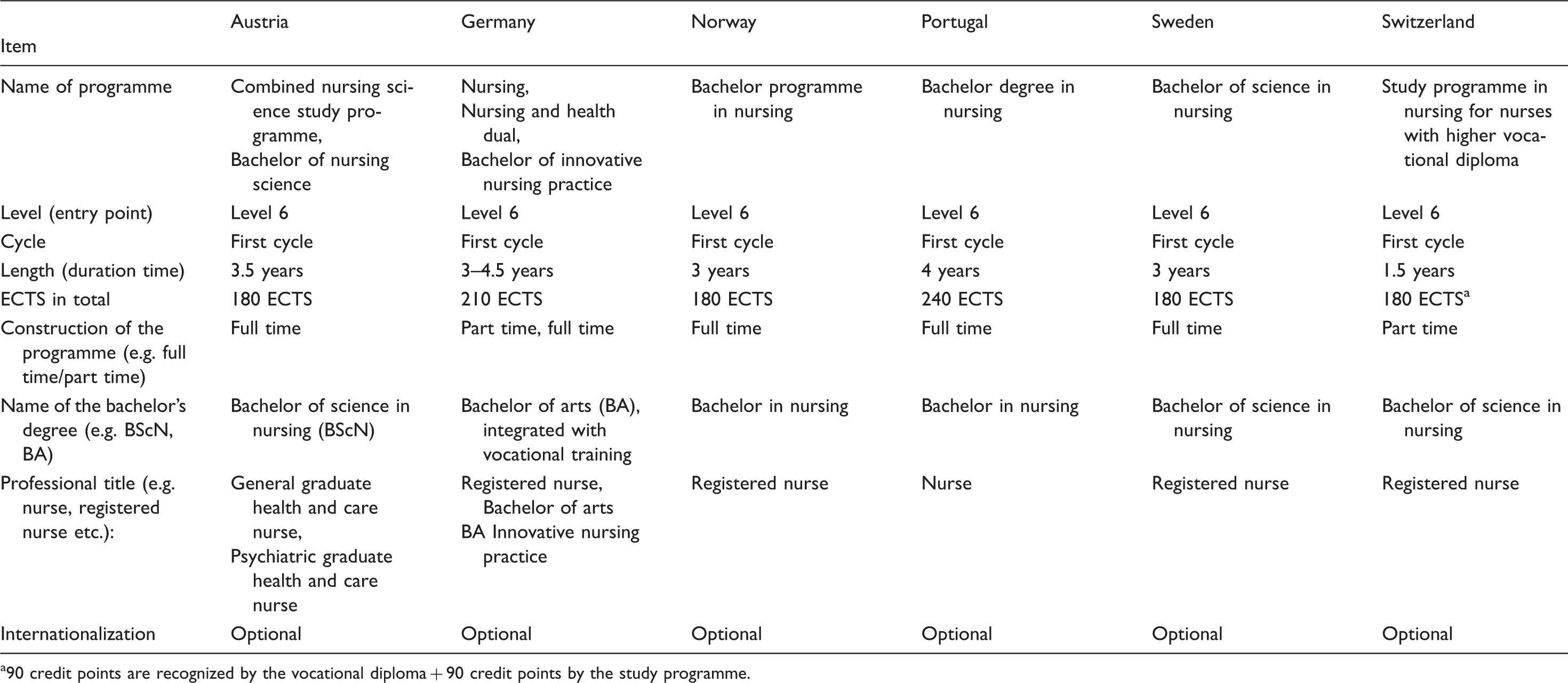
90 credit points are recognized by the vocational diploma + 90 credit points by the study programme.
Self-reported competence among nursing students graduating with bachelor's degrees in Europe
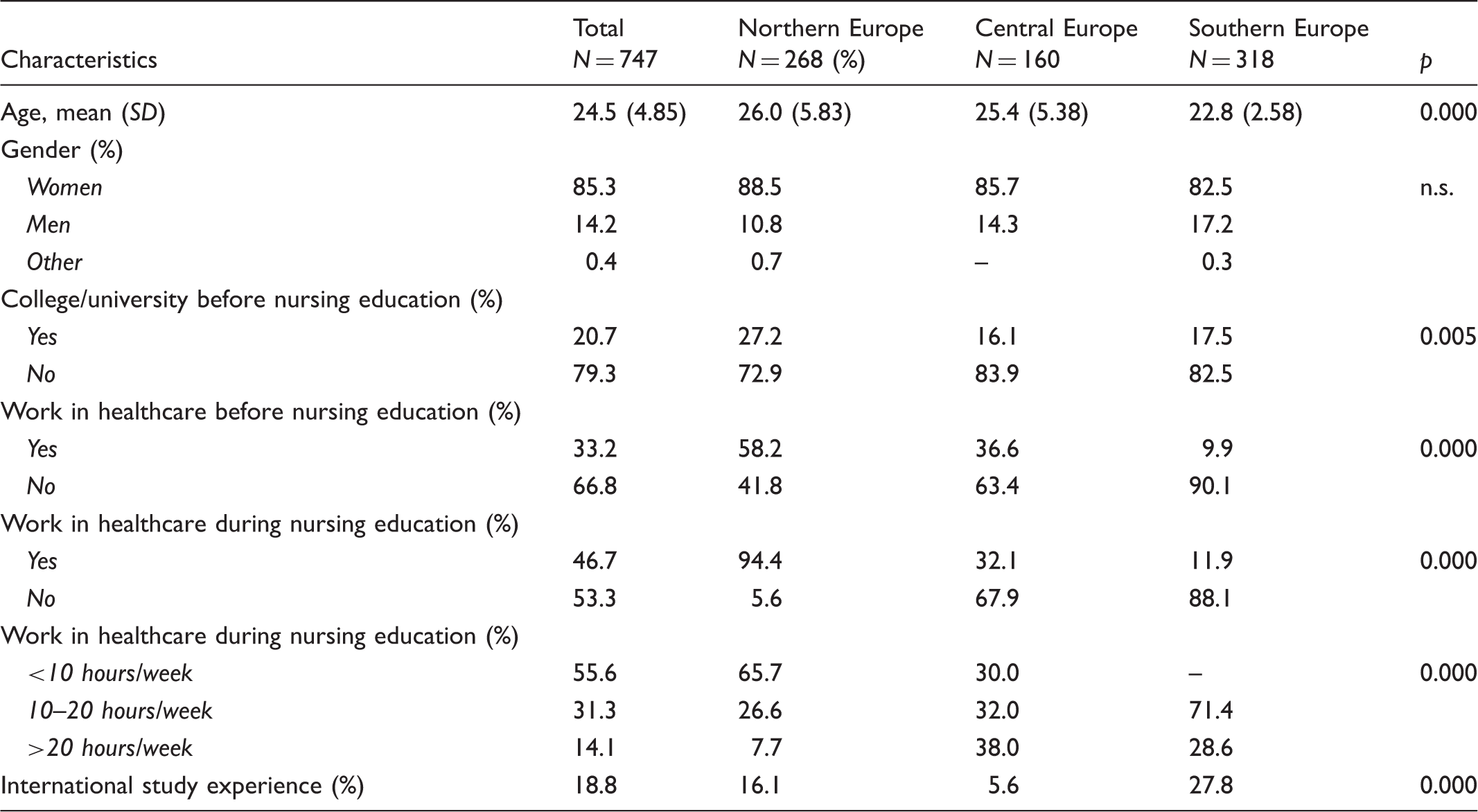
Characteristics of participating nursing students
Characteristics of nursing students in northern, middle and southern Europe.
Comparison of nursing students' self-reported competence
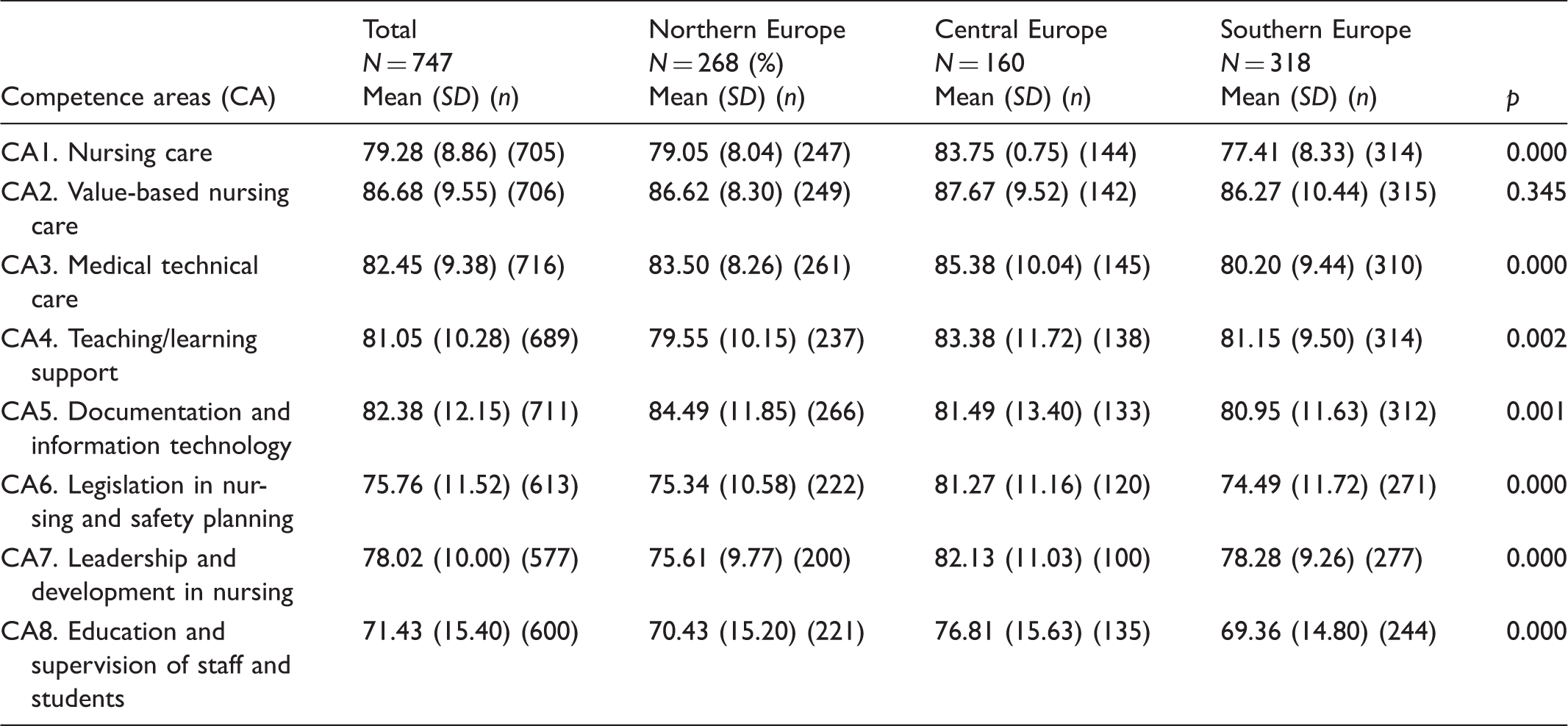
Comparison of self-reported competence (CA1–CA8) in northern, central and southern parts of Europe.
Answering ‘cannot decide’
The response alternative ‘cannot decide’ was used on all 88 items at a rate ranging from 0.1% to 14.3%, with a mean of 2.7%. On 18 items, more than 5% of the students utilized the response alternative ‘cannot decide’. Those 18 items belong to the following competence areas: CA6, Legislation in nursing and safety planning (5/9 items), CA7, Leadership and development in nursing (8/26 items), and CA8, Education and supervision of staff/students (5/5 items).
Discussion
Discussion of method
In this study, the NPC Scale 17 was used to assess self-reported nurse professional competence among nursing students about to graduate with bachelor's degrees in Europe. A literature review showed that among eight valid competence tools, the NPC Scale was the only tool that included items considered mandatory according to Austrian law. 22 The strength in this study is that it includes data from 747 nursing students from different parts of Europe and uses a well-validated questionnaire. Results from the current study showed that the reliability in terms of internal consistency was good, ranging from 0.76 to 0.95 per competence area and region. Another strength in this study is that all translations of the NPC Scale were recommended using the same procedure as the Swedish to English translation. 20
Limitations within this study could include that self-reported competence may be influenced by a number of variables that are beyond the scope of the study. There is a need to be critical of self-reported instruments, as they demand skills to be able to assess them. In addition, nurses need both appropriate knowledge and to be educated in relevant methods and approaches such as how to be self-reflective. 23 Further, the sample studied is not necessarily representative of the population of students in the different regions since it is neither a probabilistic nor a stratified sample. Categorizing the countries into three regions only gives a glimpse of the whole picture, as only six European countries were included in this study.
Nursing education programmes in Europe
Comparing the various nursing programmes of the six HEIs in European countries revealed that there are dissimilarities in terms of length, number of credits, and the structure of the programmes. However, the outcomes are similar, as the students will become nurses with bachelor's degrees. Besides regulatory issues such as the scope of nursing practice, the biggest challenge for some countries is ‘moving nursing from a vocational training model to a university model’.24(p.155) Having an adequately educated workforce is – as the research findings of Aiken et al. 3 emphasize in their RN4CAST study – not something nice to have but something which is a necessity since nursing qualifications are related to patient mortality.
Students' self-reported competence in Europe
In their work providing safe and high-quality care to patients, nurses' professional competence has been acknowledged as an important factor. The present study showed that the youngest group of nursing students are found in southern Europe. In addition, this group has less experience in working in healthcare prior to and during their nursing education programme than students in central and northern Europe. Having no experience of working in healthcare could be one reason for these students scoring lower levels of self-reported competence. Another interesting finding is that international study experience among nursing students is significantly higher among students in southern Europe. This could be linked to the fact that these students are the youngest in this study, which could mean more of them live alone without children or other family commitments, as has been mentioned in another study about students' international experience. 25
In terms of competence, students from central Europe assessed their competence as being significantly higher than students from southern and northern Europe on six out of eight competence areas. These findings could be partially explained by the different structures and contents of the respective nursing programmes. As mentioned above, the nursing programmes in central Europe differ from the ones in northern and southern Europe. Depending on the entry point to the undergraduate studies, students in central Europe have a wide variety of work experience. Some of these students have already worked as registered nurses and obtain their bachelor's degrees after their professional degrees (RN), while others have worked as registered nurses during their last study phase. These circumstances might explain why they assess themselves as having higher competence than their peers in southern and northern Europe. Differences among regions in self-reported competences may also be attributed to students' different expectations regarding the scope of practice and the professional role and expectations of nurses in different countries. In addition, students' self-reported competence may be influenced by expectations from healthcare providers as well as the degree of autonomy in nursing care.
The largest differences seen in self-reported competence between southern, central, and northern Europe are in CA6, Legislation in nursing and safety planning, CA7, Leadership and development in nursing, and CA8, Education and supervision of staff and students. These competence areas have also been named in international research as weak areas that need to be highlighted and further developed in current and future nursing education programmes internationally. 26 These findings are congruent with students’ responses on the NPC Scale using the alternative ‘cannot decide’ for CA6, CA7, and CA8. Nursing students from northern Europe scored higher on CA5, Documentation and information technology, which could indicate that nursing systems in these countries are further integrated and more commonly used within the field of digitalization in healthcare than they are in southern and central Europe.
It is worth noting that the results of the nursing students in the countries in southern and northern Europe that have moved nursing education into universities are much more similar in their self-assessments than the students from nursing programmes in central Europe.
Conclusion
According to nursing students' self-reported professional competence, the findings represent a non-homogenous picture of the current situation at some HEIs in six countries in Europe. In order to standardize and further develop nursing education in Europe, the assessment of nursing-related competences is of crucial importance. To understand the long-term impact of nursing education and competence development, other study designs are needed, for example a cohort study over a long time-frame, or follow-up studies of different kinds. Findings from this comparative study could be used as a means of raising and further develop the standard and quality of nursing education programmes at each specific HEI in each country, and to facilitate mutual exchanges between European countries as outlined in the Bologna Declaration.
Footnotes
Author contributions
Study conception/design and drafting of manuscript: Jan Nilsson, Margret Lepp, Maria Mischo-Kelling, and Andrea Thiekoetter. Data collection: Jan Nilsson, Maria Mischo-Kelling, Andrea Thiekoetter, Aida Cruz Mendes, Daniela Deufert, Ananda Fernandes, Jörg W. Kirchhoff, and Margret Lepp. Data analyses: Jan Nilsson and Margret Lepp. Critical revisions for important intellectual content: Jan Nilsson, Maria Mischo-Kelling, Andrea Thiekoetter, Aida Cruz Mendes, Daniela Deufert, Ananda Fernandes, Jörg W. Kirchhoff, and Margret Lepp.
Acknowledgements
We would like to thank Ursina Baumgartner, for collecting data at the Kaladois Fachhochschule Gesundheit, Careum Campus, Zürich, Switzerland, and Gabrielle Mackay Thomsson for language revision.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.