
Abstract
The quality of basic nursing bachelor programmes nationally and internationally must regularly be assessed to ensure that they fulfil requirements and are appropriate in relation to developments and changes in societies and healthcare systems. There is a need for instruments in helping to assess this. The aim of this study was to investigate whether the Nurse Professional Competence (NPC) Scale could serve as a tool to measure and detect possible differences between universities/university colleges regarding nursing students’ self-reported competence. Totally, 543 nursing students who had just completed their academic three-year nursing bachelor programmes at 10 universities/university colleges in Sweden participated in the study (response rate 71%). The students answered the NPC Scale with its 88 items constituting eight competence areas (CAs) and two overarching themes. The results from using the NPC Scale by the students were then compared between the 10 universities/university colleges. Significant mean score differences were found between the universities/university colleges on all CAs and on both themes. The highest mean score differences were found for the CAs ‘Medical and technical care’ and ‘Documentation and information technology’. The lowest mean score differences were found for the CAs ‘Value-based nursing care’ and ‘Leadership in and development of nursing’. It is concluded that the NPC Scale can serve as a useful tool in national and international assessments of nursing bachelor programmes.
Keywords
Introduction
Nursing is a dynamic profession that has evolved throughout history. Registered nurses (RNs) most often represent the largest single healthcare profession within healthcare systems worldwide1,2 and therefore the educational level of RNs is an important factor in meeting the demands and requirements of different healthcare systems. In order to maintain safe and high-quality care, nurses with a high level of theoretical and clinical education and with academic degrees are of outmost importance. A higher proportion of nurses with a bachelor's degree in hospital wards has been identified in a European study as a factor that can reduce the number of deaths among patients being hospitalised. 3 In the United States, it has been proposed that the proportion of RNs with an academic degree in nursing should increase to 80% by 2020, and that RNs' leadership capacity is important in order to achieve better quality of care. 4
The European Parliament has noted that nursing education programmes must be customised for future healthcare. 5 Nursing education in some European countries, however, still differs from vocational education to academic level, and it is therefore recommended by the European Parliament that nursing education programmes consist of at least three years in order to provide nurses with knowledge and skills relevant to current and future nursing. 5 In addition, the European Parliament and the Council acknowledge the importance of RNs when they state ‘Continuous professional development should cover technical, scientific, regulatory and ethical developments and motivate professionals to participate in lifelong learning relevant to their profession’.5(p.134) In 2001, the World Health Organization 6 developed a common European strategy for the education of RNs to ensure that nursing education maintains a high and even standard across all member states. The WHO Munich Declaration also expresses the unique roles of RNs and the importance of their knowledge, skills and attitudes in healthcare to develop and deliver health service. 7
In Sweden, the National Board of Health and Welfare laid down formal requirements for RNs in order to clarify RNs' profession and professional practice. The aim was to contribute to high-quality and safe patient care. 8 It was recognised that new demands are constantly placed on the nursing profession regarding the ability to work independently, to possess multi-cultural expertise and to practice professional responsibility. 8 The rapid development in medicine and nursing, and the increased demands for improved quality and cost-effectiveness in healthcare, result in a need for the education of RNs to be constantly evolving and assessed. For more than 20 years, the requirement to become an RN in Sweden has been a three-year academic nursing bachelor programme (NBP), leading to both a professional qualification and a bachelor's degree. The NBP is regulated by national educational goals set up by the Swedish Higher Education Authority, 9 which stipulates that the programme shall consist of equal parts of evidence-based theoretical and clinical courses. Each university or university college must comply with national eligibility requirements, but local, specific learning goals and NBP curricula may be included.
In 2005, and revised in 2015, the Standards and guidelines for quality assurances in the European higher education area (ESG) were adopted as part of the Bologna process with the aim to contribute to a common understanding of quality assurance of higher education among the member states (http://www.enqa.eu/index.php/home/esg/). On a national level, the universities and university colleges in Sweden have a shared obligation together with the Swedish Higher Education Authority to regularly perform quality assessments of all higher education institutions. The assessment should consist of e.g. site visits, audits, interviews and a written report by the students describing their view on how the internal quality assurance is performed at their universities/university colleges (http://english.uka.se/quality-assurance/quality-assurance-of-higher-education.html). Different types of quality assessments of all education programmes are important for disseminating information about specific programmes at different universities/university colleges. Two reasons for performing the quality assessments are to provide students with accurate information about any programme they are considering applying for, and for benchmarking between universities/university colleges. 10 Self-assessments by nursing students are seen as a possibility to develop and improve the NBPs. 11
The Nurse Professional Competence (NPC) Scale was published in 2014 and has proved to be valid and psychometrically sound. 12 It is based on the formal requirements stipulated by the National Board of Health and Welfare 8 and also conforms to the six core competencies identified by the Institute of Medicine. 13 In relation to nursing students, the scale has been used to investigate self-reported competence among nursing students on the point of graduation and in relation to background factors, 14 to assess the results of a new university education curriculum 15 to assess the effects of inter-professional education, 16 to assess the effects of internationalisation on self-reported competence 17 and to assess students' self-reported readiness to manage violence and serious events. 18
The aim of this study was to investigate whether the NPC Scale could serve as a tool to measure and detect possible differences between universities/university colleges regarding nursing students' self-reported competence after completing their nursing bachelor programme.
Material and methods
Sample and data collection
The sample consisted of nursing students at 10 out of a total of 25 universities/university colleges in Sweden offering NBPs. The universities/university colleges were purposively selected, evenly distributed geographically across the country, and included both universities (n = 4) and university colleges (n = 6) in major (>100,000 inhabitants) and minor cities.
An invitation letter was sent out to the 10 universities/university colleges, and all the principals gave their permission to perform the study. All nursing students at the 10 universities/university colleges who had passed all theoretical and clinical examinations were invited to participate in the study by answering the NPC Scale on one of the last days of their education programme. The students received information about the study from a lecturer at each university/university college who also handed out and then collected the NPC Scale questionnaire. The lecturer remained in the lecture hall to answer any potential questions. In total, 543 nursing students (response rate 71%) participated (mean age 28 [20–50] years, 86% women).
The Nurse Professional Competence Scale
The NPC Scale consists of 88 items presented as questions starting with ‘Do you think you have the ability to …’ followed by an example of a competence relevant to nursing. One example is ‘Do you think you have the ability to respectfully communicate with patients, relatives and staff ?’, another example is ‘Do you think you have the ability to independently perform or participate in examinations and treatments?’. The 88 items form eight competence areas (CAs), which in turn constitute two themes.
12
The CAs identified
12
are:
CA1: Nursing care (included in Theme I) CA2: Value-based nursing care (included in Theme I) CA3: Medical and technical care (included in Theme I) CA4: Teaching/learning and support (included in Theme I) CA5: Documentation and information technology (included in Theme I) CA6: Legislation in nursing and safety planning (included in Themes I and II) CA7: Leadership in and development of nursing (included in Theme II) CA8: Education and supervision of staff and students (included in Theme II)
The two themes are ‘Patient-related nursing’ (Theme I) and ‘Organisation and development of nursing care’ (Theme II). The 88 items are answered on a scale where 1 = to a very low degree and 4 = to a very high degree.
Statistical measures
Data were described with descriptive statistics and analysed using inferential statistics, using SPSS Statistics 22.0 by IBM for Windows (SPSS Inc., an IBM Company, Chicago, IL, USA). Mean scores were calculated for all CAs and the two themes. The mean scores were then transformed into a 1–100 scale, where higher scores indicated higher self-reported competence. The internal dropout was low, between 0 and 1.2% across all separate items. Missing item values were replaced by the imputed mean for the whole group.
One-way analysis of variance (ANOVA) with Bonferroni post hoc tests was used for comparing the self-reported competence of students at the different higher education institutions (HEIs). Statistical significance was set at p < 0.01 due to multiple comparisons. From the post hoc tests, Cohen's d estimates were used to analyse effect sizes using the mean differences between the HEIs with highest and lowest mean scores for computation. According to Cohen, effect sizes of 0.20 to 0.50 indicate a small difference, effect sizes of 0.51 to 0.80 a medium difference, and effect sizes >0.80 a large difference. 19
Ethical considerations
The voluntary nature of participation was stressed when the nursing students were informed about the study. Responses to the NPC Scale were provided anonymously. By choosing to respond to the NPC Scale, the participants were considered to have given their informed consent. In Sweden, the current law of research ethics 20 states that it is not necessary to request approval from an ethical committee to collect this kind of data.
Results
The mean scores for each university/university college for the eight CAs and for the two themes are shown in Figure 1. A very similar curve pattern was identified for all universities/university colleges although the mean scores were placed on different levels.
The figure shows the mean scores for the eight competence areas (CA) and the two themes for each university/university college based on nursing students' self-reported competence. The universities/university colleges are referred to by the letters A, B, C etc.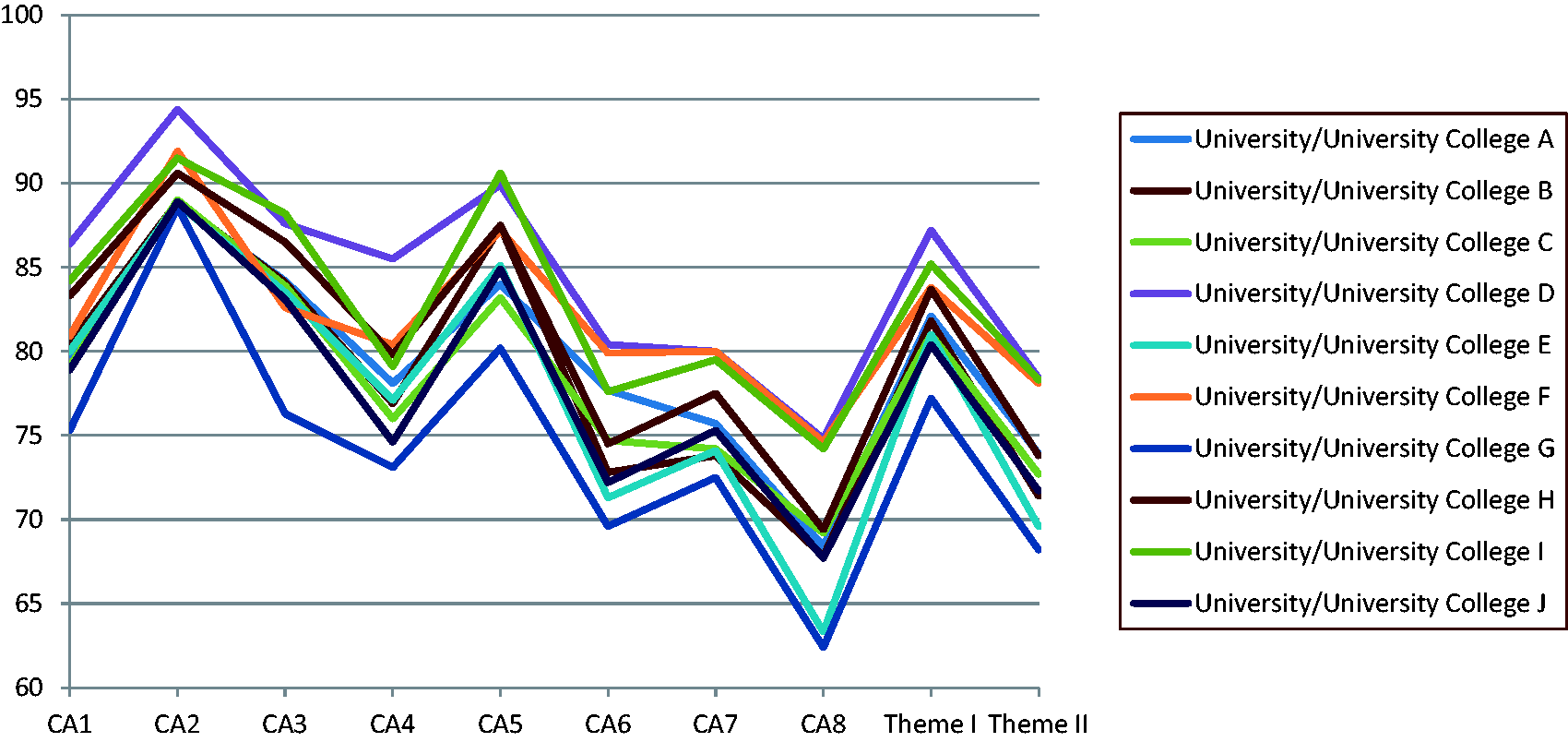
Mean scores and mean score differences for eight nursing competence areas and two themes measured by the NPC Scale. The data are based on self-reported competence by 543 nursing students who had just completed their nursing bachelor programmes.
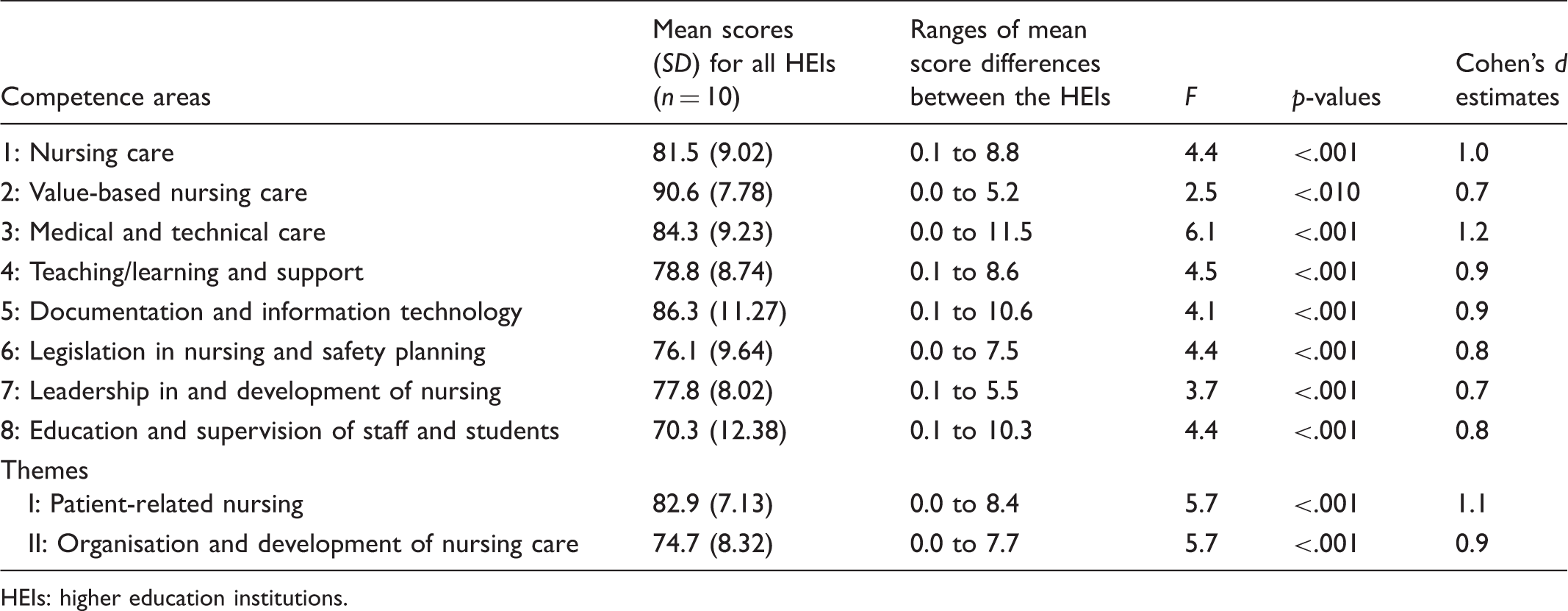
HEIs: higher education institutions.
Discussion
This study was undertaken to investigate whether the NPC Scale could serve as a future tool in quality assessments of NBPs. The study showed that the instrument indeed could measure and identify differences regarding nursing students' self-reported competence between samples of universities/university colleges.
Healthcare systems are faced with great challenges. Some examples are ageing populations with multi-morbidity, an increasing cultural diversity in many countries, a rapid development of new genetic diagnostic tools and treatments, the increased use of eHealth technology and better-informed patients with higher demands for power and influence over their care. Due to these challenges influencing healthcare systems, the curricula of NBPs must address peoples' rights and changing needs to ensure high quality and equitable healthcare. 7 It is therefore important to regularly assess the quality of NBPs to ensure that they fulfil requirements and are appropriate in relation to developments and changes in societies and healthcare systems. 21 By using the NPC Scale it was possible to detect differences in students' self-reported competence depending on which university/university college they had studied at. This can be seen as one important quality aspect of NBPs. In order to stimulate discussions about future benchmarking and quality development of the NBPs, the results from the study were reported back to the participating universities/university colleges. Each individual university/university college was informed of the results pertaining to themselves, while the results for the other universities/university colleges were only presented by means of a letter.
The significant mean score differences on all CAs between the universities/university colleges mirror the nursing students’ self-reported competence regarding 88 nursing competencies. The lowest mean score difference between the universities/university colleges was found for CA2 ‘Value-based nursing care’ including items about e.g. the ability to respectfully communicate with patients, relatives and staff; to contribute to a holistic view of the patient when performing nursing care and showing respect for humanistic values, autonomy, integrity and dignity, values and beliefs; to act upon patients’ and relatives’ wishes and needs; and the use of principles of research ethics. The highest mean score difference was found for the CA3 ‘Medical and technical care’, including items about e.g. the ability to independently perform or participate in examinations and treatments; following up on the patient's condition after examination and treatments; managing drugs and drug administration with knowledge of clinical pharmacology; independently administering prescriptions; posing questions about unclear instructions and applying hygienic principles and routines. The reasons for the reported differences in self-reported competence are not known and are outside the scope of this study. Whether the same differences in perceived competence would be identified if the nursing students’ competence had also been objectively measured cannot be answered in the context of this study. However, to investigate this, the clinical and theoretical results from the Swedish National Clinical Examination 22 (http://www.nkse.se/index.php/in-english) are currently being combined with data from the NPC Scale (unpublished data).
Another interesting finding in this study was that a very similar curve pattern was identified for all universities/university colleges, although the mean scores were placed on different levels (Figure 1). All universities/university colleges in Sweden that offer an NBP must present a curriculum that complies with the national education objectives set by the Swedish Higher Education Authorities. 9 These in turn are based on the Bologna Declaration, 23 which creates a basis for a common European educational framework, harmonising European higher education systems and creating convergence in terms of curriculum structures and competencies. 24 All curricula for NBPs in Sweden must adhere to the national educational goals and be structured into three levels of learning goals: ‘Knowledge and understanding’, ‘Skills and abilities’ and ‘Judgement and approach’. This is a model for structuring the learning process for the nursing students with a progression in complexity. The use of national educational goals and the use of a similar model for structuring the learning process may be a reasonable explanation for the very similar curve pattern found in this study for the eight CAs and the two themes.
The NPC Scale has previously been evaluated for face validity, data quality, construct validity, reliability and known-group validity. 12 The results from the current study stimulate further studies of using the NPC Scale both nationally and internationally in pedagogical quality work. An example of the latter is an on-going research project, initiated by the European Network Nursing Academies (ENNA, http://en-na.eu) using the NPC Scale to compare self-reported competence among nursing students at the point of graduation in six European countries. The NPC Scale has been translated into English, 25 Norwegian, German and Portuguese and additional translations are in progress into Dutch and Italian. In Austria, the German translation of the NPC Scale has rendered a recommendation of being taken into use, as the NPC Scale is considered the only scale that fulfils the Austrian legally defined competence areas. 26 Nursing students have found the NPC Scale relevant to answer 12 and the internal dropout in the current study was very low. Nevertheless, a shorter version of the NPC Scale with 35 items has been developed 27 to facilitate the use of other instruments together with the NPC Scale. The short form is likely to be possible to use to compare HEIs regarding nursing students' self-reported competence although this remains to be shown.
Conclusion
In this study the main finding was that the NPC Scale could detect differences between universities/university colleges with regard to nursing students' self-reported competence. It is concluded that the NPC Scale can be used as a tool for quality assessments, benchmarking projects and improvements of nursing education programmes at national and international levels.
Footnotes
Acknowledgements
We are grateful to all the nursing students who took the time to participate in the study during the final days of their nursing education, to lecturers at the universities who kindly helped handing out and collecting the NPC Scale questionnaire, and to Hilary Hocking, Östersund, Sweden, for language revision. The research was conducted within the NPC-research network: ![]()
Author contributions
Study conception/design: AG and JN. Data collection: AG, JN, JF, JL, ML, CL, EJ and KT. Data analyses: JF, JN, AG, MC (statistical advisor) and EJ. Main authors: AG and JN. Critical revisions for important intellectual content: AG, JN, MC, JF, GN, ML, JL, CL, KT and BW-L. All authors read and approved the manuscript.
Funding
This study was supported by grants from the Alice Lindström Fund and research allocations from the authors’ universities.
Conflict of interest
The authors declare that there is no conflict of interest.
Note
In memory of our friend and colleague Eva Johansson, RN, PhD, Associate Professor at the Department of Neurobiology, Care Sciences and Society, Division of Nursing, Karolinska Institutet, Stockholm, Sweden, who contributed to the study.