
Abstract
For patients in intensive care units, long periods of bed rest and restricted physical activity can result in adverse side effects. One of the conditions many patients experience during intensive care unit stays is breathing difficulty. Here, we aimed to identify and evaluate the evidence base for nonpharmacological or nontechnical interventions targeting breathing difficulties, and to propose interventions needing further investigations. This study is reported in accordance with PRISMA for Scoping Reviews. A systematic search was conducted in MEDLINE, EMBASE, and Cochrane. A scoping review was undertaken using the Arksey and O’Malley framework. In all, 1190 records were found and 27 of them were included in the review. Interventions targeting breathing difficulties were chest physiotherapy, breathing techniques, inspiratory muscle training, early exercise training, position-specific optimization, and other nonpharmacological interventions. Several of the interventions showed minor beneficial effects. However, because of limitations in the studies, the findings are inconclusive and need further research.
Background
Intensive care unit (ICU) patients, by definition, are critically ill. Most are mechanically ventilated, and require sedative and analgesic drugs to reduce distress, pain, and oxygen consumption during their stay. Long periods at the ICU with restricted physical activity and enforced bed rest can result in numerous alterations in body function, such as neuromuscular weakness, pressure ulcers, atelectasis, aspiration pneumonia, muscle weakness and atrophy, bone mineral loss, orthostatic hypotension, tachycardia, and decreased cardiac output.1–4 These ICU-acquired conditions can lead to significant impairment of function after the patients leave the unit. Many of the survivors develop new or worsening physical, cognitive, and/or mental impairments after ICU treatment,5–8 which now is recognized as post-intensive care syndrome (PICS). 9 This aspect is often ignored, which can lead to a reduced quality of life and increased suffering for these patients after ICU discharge.
One set of conditions many patients experience during ICU stay comprises breathing difficulties. For example, ICU patients are at high risk of dyspnea, 10 , 11 and this is a major cause of emotional distress and physical suffering for them. In one study, 171 ICU patients at high risk of dying were interviewed every other day for up to 14 days. Dyspnea was prevalent in 44% of the assessments and was the most distressing symptom. In this study, no differences were found in dyspnea intensity or distress ratings reported by patients who were mechanically ventilated versus those who were not. 12 It is worth noting that even if increased attention is being given to this symptom, 13 ICU clinicians often underestimate breathing discomfort in these patients. 14 , 15 In addition, other breathing difficulties are present in patients with serious illness, including cough, malignant pleural effusions, airway secretions and hemoptysis. Beyond physical effects, these symptoms exert significant psychological, social, existential, and spiritual impact on the patients’ experience. 16
Nurses working with ICU patients often have an important role in assessing and treating distressing symptoms as they are beside these patients during their whole ICU stay. For example, in a country like Norway, critical care nurses, who have a minimum of 1.5 years of further education after receiving a bachelor’s degree in nursing, play an important role regarding ICU patients’ breathing difficulties. Nurses mobilize and reposition these patients several times per day. Other procedures include secretion removal, oral care, oxygen therapy, and respiratory monitoring. 17 Often, these nursing interventions are nonpharmacological or nontechnical, and the effects of these interventions are not always clear. To be able to motivate patients to do these interventions, and to know that our work is based on best evidence, it is important to have an overview of which of these interventions are effective. For these reasons, a scoping review was conducted in order to systematically map the research done in this area, as well as to identify any existing gaps in knowledge. The aim of this study was therefore to provide an overview of the literature regarding such nursing interventions for ICU patients with breathing difficulties. We had two specific aims: first to identify and evaluate the evidence base for nonpharmacological or nontechnical interventions targeting breathing difficulties in ICU patients; and second, to propose similar interventions that need further investigation.
Methods
This study is reported in accordance with PRISMA for Scoping Reviews. 18 The present scoping review, was defined as a ‘form of knowledge synthesis that addresses an exploratory research question aimed at mapping key concepts, types of evidence, and gaps in research related to a defined area or field by systematically searching, selecting and synthesizing existing knowledge’. 19 (p.1292) To study the knowledge base for nursing activities and identify research gaps, we applied the framework suggested by Arksey and O’Malley. 20 This includes a five-step approach: 1) identification of the research question; 2) identification of relevant studies; 3) study selection; 4) charting the data; and 5) collating, summarizing, and reporting the results.
Literature search
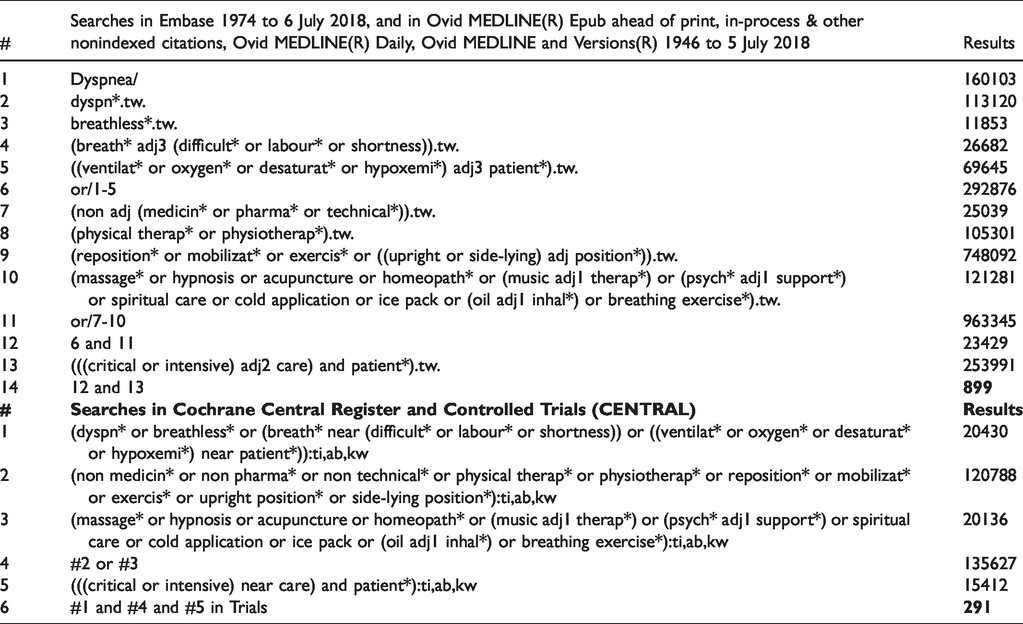
To identify potentially relevant documents, a systematic literature search was performed in cooperation with a health science librarian with expertise in systematic review searching. Medical subject headings and text words related to patients with breathing difficulties, ICU patients, and nonpharmacological and nontechnical nursing interventions were used. The search was conducted without any date limitations, and the keywords were broad to ensure we captured the current evidence. The search was conducted on July 9, 2018 and we searched MEDLINE, EMBASE, as well as the Cochrane Central Register of Controlled Trials. For further details, see Table 1.
Complete search strategy.
Inclusion and exclusion criteria
Three critical care nurses (the reviewers in this study) discussed inclusion and exclusion criteria for publications. To be included in the review, the following inclusion criteria were applied: patients were enrolled in an ICU (including both mechanically ventilated ICU patients and nonmechanically ventilated ICU patients), and aged 18 years or older; breathing difficulties were recorded as main or secondary outcomes; they needed to be original studies (i.e. no author opinions, case studies, or systematic reviews); and only English-language studies. Studies were excluded if they included pharmacological (i.e. medications) or technical (i.e. noninvasive ventilation [NIV] or mechanical ventilation) interventions. Protocols not leading to any publication were excluded, as were conference abstracts and unpublished data.
Study selection
After removing duplicates, conference abstracts, and records not in English, groups of two reviewers independently evaluated titles and abstracts from the records identified through database searching, followed by a discussion and final consensus about which studies to include as full-text articles. Thereafter, included full-text articles were read (also here in groups of two reviewers). Before final selection of the full-text articles to be included, the reviewers discussed any conflicting decisions, so that any disagreement was resolved by discussion and consensus before final study selection.
Data extraction
Because this is a scoping review, we used data extraction and not quality appraisal. 20 A data-charting form was developed to determine which variables to extract. Groups of two reviewers read the included studies individually and extracted the following key information: author(s); year of publication; origin/country of origin (where the study was published or conducted); aims/purpose; study population and sample size; methodology; intervention type; comparators and details of these; duration of the intervention (if applicable); outcomes and details of these (if applicable); and key findings related to the scoping review question. Disagreements were resolved in a discussion between the three reviewers extracting the data.
Analysis
We grouped the studies thematically by the type of intervention used, resulting in six categories: chest physiotherapy; breathing techniques; early exercise training; inspiratory muscle training; position-specific optimization; and nonpharmacological interventions. The results were presented in a narrative format, in a flow diagram (Figure 1), and in tables (Table 2 and Table 3).
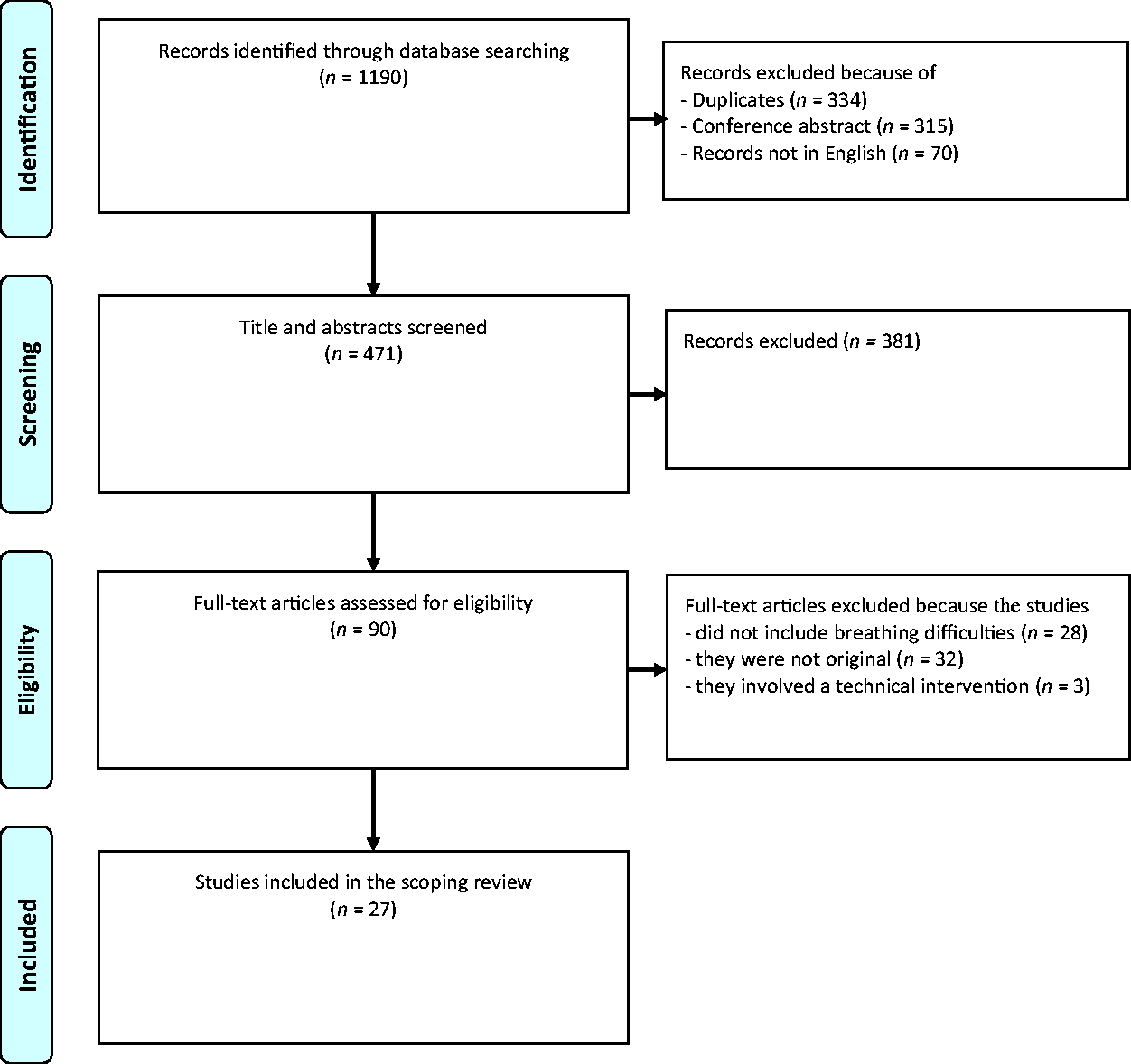
Identification and inclusion of studies.
Overview of the included studies according to country of origin, aim, study population, and design.
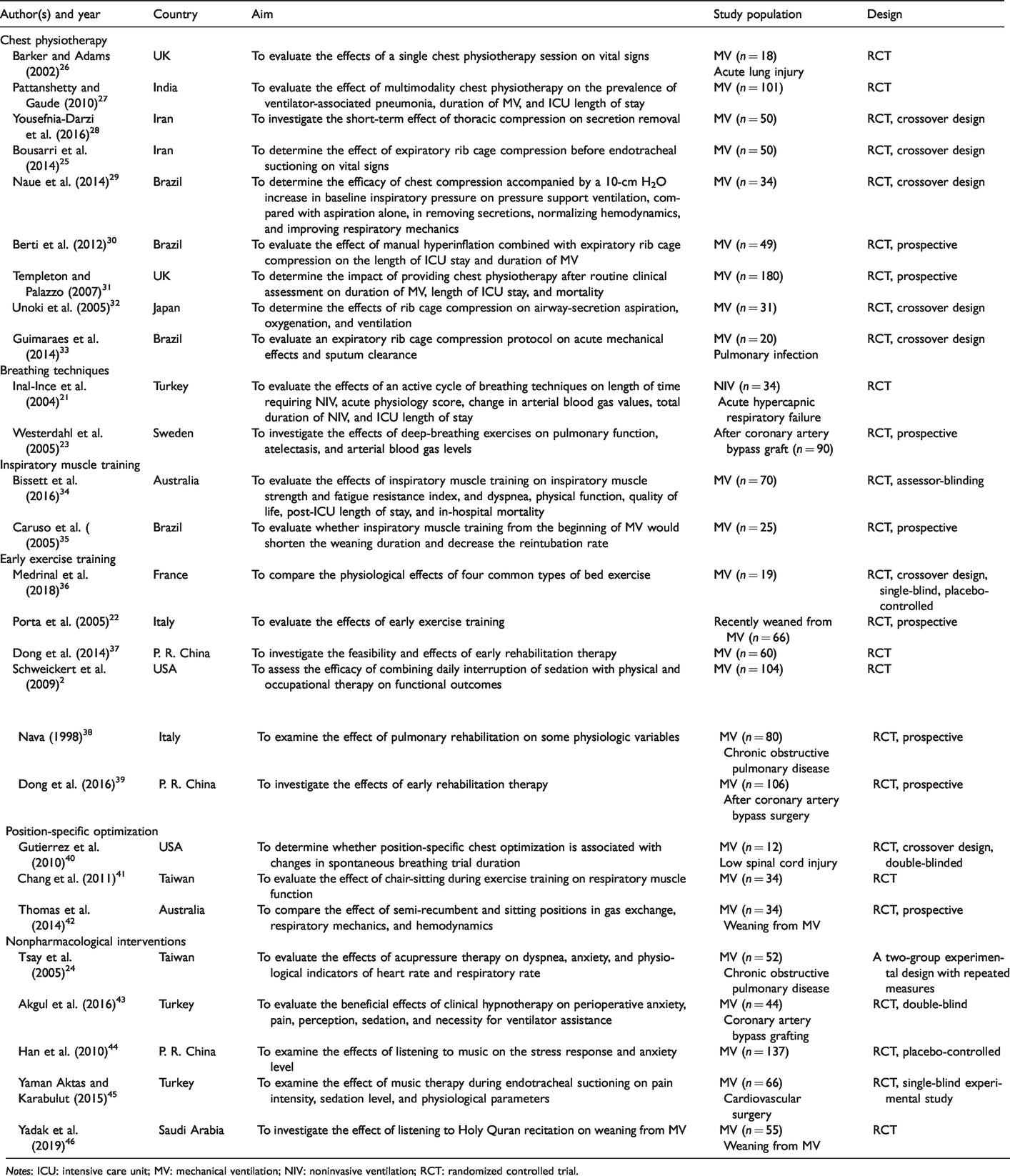
Notes: ICU: intensive care unit; MV: mechanical ventilation; NIV: noninvasive ventilation; RCT: randomized controlled trial.
Presentation of the results.
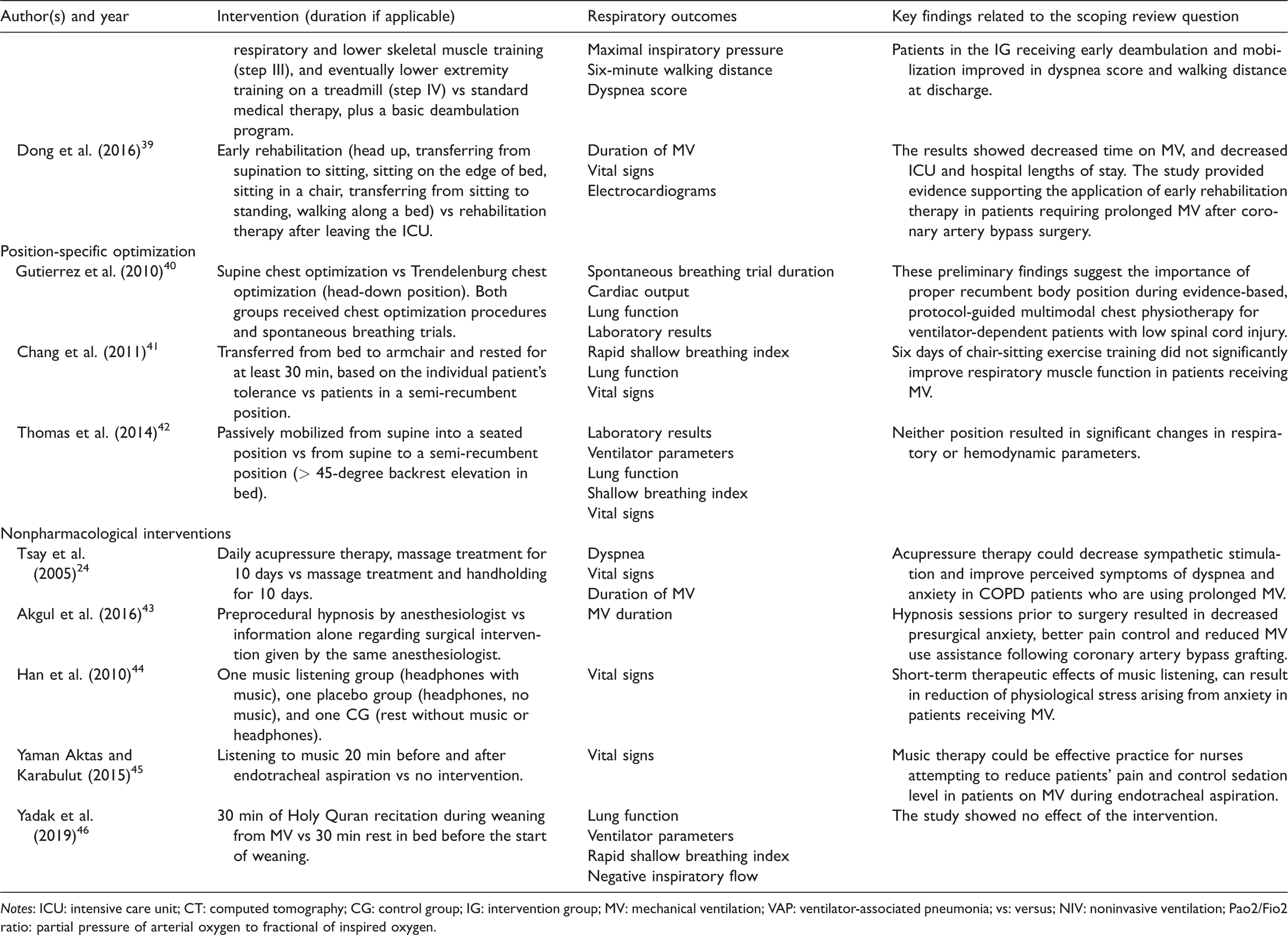
Notes: ICU: intensive care unit; CT: computed tomography; CG: control group; IG: intervention group; MV: mechanical ventilation; VAP: ventilator-associated pneumonia; vs: versus; NIV: noninvasive ventilation; Pao2/Fio2 ratio: partial pressure of arterial oxygen to fractional of inspired oxygen.
Results
The systematic database search yielded 1190 records. After removing duplicates (n = 334), conference abstracts (n = 315), and records not in English (n = 70), 471 records remained, the titles and abstracts of which we read. After excluding records not fitting the inclusion criteria (n = 381), 90 articles were included to read as full-text articles. Of these, 63 articles were excluded because the studies did not include breathing difficulties (n = 28); they were not original (n = 32); or because they involved a technical intervention (n = 3). This left 27 studies for analysis.
The studies included in this review were published over 20 years (from 1998 to 2018), and represented countries all over the world (for details see Table 2). In all, 1621 patients were included. Most of the studies (n = 24) included mechanically ventilated patients. However, one study included patients receiving NIV, 21 one included patients recently weaned from ventilation, 22 and one included patients not receiving any type of ventilation. 23
The design in 26 of the 27 studies was that of a randomized controlled trial (RCT), and one had a two-group experimental design with repeated measures. 24 Eight of the RCTs had a crossover design. Overall, the interventions used in the included studies could be divided into six types: chest physiotherapy (n = 9); breathing techniques (n = 2); inspiratory muscle training (n = 2); early exercise training (n = 6); position-specific optimization (n = 3); and other nonpharmacological interventions (n = 5). For an overview of the countries of origin, aims, study populations, designs, interventions, respiratory outcomes, and key findings, see Tables 2 and 3.
Discussion
Chest physiotherapy
We identified nine original research studies investigating the effects of chest physiotherapy in ICU patients.25–33 These studies included 533 patients, a strength when evaluating the effect of such interventions. Chest physiotherapy includes several different interventions such as thoracic squeezing, expiratory rib cage compression and chest wall percussion, or different combinations of interventions, such as positioning, manual hyperinflation, and suctioning. Regarding the respiratory effects of these interventions in ICU patients, several studies suggest that chest physiotherapy has positive effects for them, such as a decrease in the occurrence of ventilator-associated pneumonia, 27 increased removal of airway secretions, 28 , 29 accelerated weaning from mechanical ventilation, 30 and accelerated ICU discharge. 30 Other studies show no effects of chest physiotherapy interventions.31–33 However, when evaluating the effects of these interventions, there was a challenge in that several of the studies included mixed interventions. For example, in one study, chest wall percussion was combined with positioning, manual hyperinflation, and suctioning. 27 These multimodal interventions make it difficult to decide which of the interventions, or a combination thereof, was associated with the findings.
Breathing techniques
Only two of the included studies had interventions regarding breathing techniques. 21 , 23 The breathing techniques used in these studies were either an active cycle of breathing exercises 21 (4–6 breathing control breaths, 3–4 thoracic expansion exercises, and the forced expiration technique including 4–6 breathing control breaths combined with 2–3 huffs), or deep-breathing exercises 23 (30 slow, deep breaths performed with a positive expiratory pressure blow-bottle device). These two studies included 124 patients. The patients were either receiving NIV for acute hypercapnic respiratory failure or were nonmechanically ventilated patients recovering after coronary bypass grafting. The two studies suggested that these breathing techniques showed patients had shorter times requiring NIV, smaller atelectatic areas, and better pulmonary function. However, it is worth noting that deep-breathing intervention did not show any effect on arterial oxygen tension, carbon dioxide tension, or durations of ICU or hospital stay. One of the studies evaluated the patients’ subjective experience. In the deep-breathing group, 72% of the patients experienced a subjective benefit from the exercises. 23
Inspiratory muscle training
Regarding inspiratory muscle training, only two studies were included. 34 , 35 Patients enrolled in these two studies were ventilated mechanically or newly extubated. Training was performed by adjusting the trigger sensitivity threshold of the ventilator, 31 or by using an inspiratory muscle training device. 30 Only a small number of patients were included in these studies (n = 95) which might diminish the generalizability of the findings. One of these studies showed increased inspiratory muscle strength, 34 but in the other this tended to stay constant. 35 These two studies showed no statistically significant differences in fatigue resistance index, physical function, dyspnea, 34 weaning duration, and reintubation rate. 35 Even if the interventions in these two studies were more technical than in the other studies included, one of them evaluated the patients’ quality of life, and revealed that improvement in this measure was greater in the intervention group compared with the control group. 34
Early exercise training
Six different studies included interventions regarding early exercise training. 2 , 22 ,36–39 These interventions included a passive range of movements, passive cycle-ergometry, electrical stimulation of the quadriceps muscles, functional electrical stimulation combined with cycling, supported arm exercise training, and head-raising, transferring from supination to sitting, sitting on the edge of the bed, sitting in a chair, transferring from sitting to standing, and walking alongside a bed. Several positive effects of these interventions were found, such as earlier ‘first day out of bed’, 37 shorter duration of delirium, 2 improvement in the dyspnea score, 38 and decreased durations of mechanical ventilation, and hospital and ICU stays. 39 One strength of this form of intervention was that 435 patients were included. However, the studies included several different interventions, which made it difficult to compare the results with each other and with the overall findings. There was also a limitation in that a definition of ‘early’ was not clear in several of the studies using this intervention.
Position-specific optimization
Three studies included in this category evaluated the effect of position-specific optimization.40–42 The interventions included different position-specific chest optimizations, chair-sitting, and semi-recumbent and sitting positions. One study evaluated whether position-specific chest optimization was associated with changes in the duration of a trial of spontaneous breathing. 40 These preliminary findings suggest the importance of proper recumbent body position during evidence-based, protocol-guided multimodal chest physiotherapy for ventilator-dependent patients with low spinal cord injuries. It is worth noting that only 12 patients were included in this study. Another study evaluated chair-sitting exercise training. 41 The intervention did not significantly improve respiratory muscle function in mechanically ventilated patients. The third study compared the effect of semi-recumbent and sitting positions. 42 Neither patient position resulted in significant changes in respiratory or hemodynamic parameters. Both positions can be applied safely in patients being weaned from ventilation. It is worth noting that only a few patients (n = 80) were included in these three studies (range 12–34 per study).
Nonpharmacological interventions
Five studies (n = 354 patients) were included in the group of interventions we have called nonpharmacological. 24 ,43–46 The interventions included acupressure therapy, 24 clinical hypnotherapy, 43 listening to music, 44 , 45 and listening to recitations from the Holy Quran. 46 Several of them evaluated symptoms such as anxiety and pain. However, respiratory measures were often secondary outcomes, so these studies have been included here with caution. Acupressure therapy helped decrease sympathetic stimulation and improve perceived symptoms of dyspnea and anxiety in patients with chronic obstructive pulmonary disease. 24 Hypnosis prior to surgery was an effective complementary method in decreasing presurgical anxiety, and resulted in a reduced need for ventilator assistance following coronary artery bypass grafting. 43 One study showed short-term therapeutic effects of listening to music, resulting in substantial reductions in physiological stress responses (including respiratory rate) arising from anxiety in mechanically ventilated patients. 44 Another study showed that music therapy could be effective in reducing patients’ pain and controlling the sedation level in mechanically ventilated patients during endotracheal aspiration, 45 but there were no differences in vital signs such as oxygen saturation. Finally, listening to recitations from the Holy Quran showed no positive effects on rapid shallow breathing index, respiratory rate, heart rate, oxygen saturation, exhaled carbon dioxide, or blood pressure. 46 As the interventions in this category varied widely between studies, it is difficult to conclude whether they might be effective in targeting breathing difficulties in ICU patients.
Interventions needing further investigation
It is interesting that alternative methods such as nonpharmacological therapies could be useful and used as adjuncts when treating patients in an ICU. Scoping reviews of other areas, such as pain relief, suggest the use of comprehensive multimodal interventions to investigate the effects of nonpharmacological treatment protocols on pain intensity and pain proportion and their impact on opioid consumption, 47 as the possibly serious adverse effects of these drugs should be considered when applied in treatment. 48 Nonpharmacological and nontechnical interventions have few negative effects, are cheap, easy to provide, and safe, 49 and might be beneficial when combined with classical pharmacological therapies. Several single studies included here found positive effects on some respiratory outcomes in ICU patients. However, it is difficult to recommend which nonpharmacological or nontechnical nursing interventions to use. There were several limitations in these studies regarding the effects of the interventions for ICU patients with breathing difficulties. Because of the diversity of interventions, low number of studies, and small numbers of patients included in the studies, it was impossible to perform statistical analyses for effects using meta-analysis. Even though some studies included many patients, several included as few as 12, 18, or 20, which could have introduced the possibility of selection bias. The evidence we included was sometimes further hampered by unclear descriptions of methods, and different study populations, which made it difficult to draw firm conclusions. Several studies also had multimodal interventions, which made it difficult to determine the causes of any effects. In addition, some outcomes were short-term measures during ICU treatment (e.g. effects on vital signs, aspiration of secretions, oxygenation saturation levels, other blood gas values, and atelectasis), while other outcomes were longer term (e.g. duration of mechanical ventilation, length of ICU stay, and mortality rates). Note that some of the interventions in the included studies were short and repeated only a few times. ICU patients with breathing difficulties could be part of a long treatment chain during hospitalization. When evaluating the long-term effects of different short-term interventions, it is difficult to distinguish between the effects of the selected interventions and other interfering elements during the treatment chain.
The aims of this study were to identify and evaluate the evidence base for interventions targeting breathing difficulties in ICU patients, and to propose interventions and further investigations. However, it is not clear which type of healthcare professional should be responsible for performing the interventions described here. Some of the interventions, such as chest physiotherapy and breathing techniques, might be regarded as the physiotherapist’s field. However, nurses are at the patient’s bedside most of the day, and interventions such as different position-specific optimization, breathing techniques, and rib cage compression might be appropriate for them to perform during the day. Members of several different professions might perform interventions for patients in an ICU, based upon availability, culture, and professional description at each hospital. However, coordinated teamwork between the different healthcare professional groups might be the best option.
ICU patients are a vulnerable patient group. Breathing difficulties such as dyspnea are shown to be among the most distressing symptoms in ICU patients. 12 However, even though breathing difficulties was the main focus in the present study, research shows that ICU patients experience and suffer from several distressing symptoms during their ICU stay. New research highlights for example that dyspnea, pain, and thirst are the most prevalent, intense, and distressing symptoms for ICU patients, 50 in addition to anxiety, poor sleep quality and/or insomnia. 13 In addition, these symptoms also might have an impact on each other. 51 The findings stress the importance of nursing assessing several symptoms in ICU patients, focusing on the fact that different symptoms might have an impact on each other, and being aware of the complexity in symptom burden in these patients. Only in this way, a holistic care of the ICU patients may be performed.
Limitations
Our scoping review has some limitations. The search strategy in the present study could have been made even more comprehensive. It may have yielded more relevant studies. In addition, this was a scoping study and there are several limitations to such methods. 20 For example, they do not appraise the quality of evidence in the primary research reports in any formal sense. The quantity of data generated can be considerable, which can lead to difficult decisions about how far the breadth of information might be more important than its depth. In addition, a scoping study does not address the issue of the ‘synthesis’ of any particular intervention. However, scoping studies provide a narrative or descriptive account of available research and this was warranted for ICU patients with breathing difficulties. Therefore, we think the scoping method was suitable for the aim of this study.
Conclusions
Several of the interventions used to assist ICU patients with breathing difficulties showed beneficial effects. Some interventions also revealed effects other than respiratory, such as lowering anxiety and pain, which in turn may contribute to positive respiratory effects. However, because of limitations in several of the studies included in this review, the low numbers of studies and few patients included, our findings are inconclusive. We recommend further research on this topic.
Footnotes
Acknowledgments
We would like to thank Julie Skattebu who participated in this study by carrying out the literature search. We also acknowledge Østfold University College for funding the study.
Funding
Østfold University College funded the study.
Conflict of interest
The authors declare that there is no conflict of interest.